
Abstract
Background:
Female servicemembers sustain higher rates of lower extremity injuries as compared with their male counterparts. This can include intra-articular pathology in the hip. Female patients are considered to have worse outcomes after hip arthroscopy for femoroacetabular impingement and for hip labral repair.
Purpose:
To (1) compare published rates of hip arthroscopy between male and female military servicemembers and (2) determine if there are any sex-based differences in outcomes after hip arthroscopy in the military.
Study Design:
Systematic review; Level of evidence, 3.
Methods:
We reviewed the literature published from January 1, 2000, through December 31, 2020, to identify studies in which hip arthroscopy was performed in military personnel. Clinical trials and cohort studies were included. The proportion of women within each cohort was identified, and results of any between-sex analyses were reported.
Results:
Identified were 11 studies that met established criteria. Studies included 2481 patients, 970 (39.1%) of whom were women. Surgery occurred between January 1998 and March 2018. Despite women accounting for approximately 15% of the active-duty military force, they represented 39.1% (range, 25.7%-57.6%) of patients undergoing hip arthroscopy. In most cases, there were no differences in self-reported outcomes (pain, disability, and physical function), return to duty, or medical disability status based on sex.
Conclusion:
Women account for approximately 15% of the military, but they made up 40% of patients undergoing hip arthroscopy. Outcomes were not different between the sexes; however, definitive conclusions were limited by the heterogeneity of outcomes, missing data, lack of sex-specific subgroup analyses, and zero studies with sex differences as the primary outcome. A proper understanding of sex-specific outcomes after hip arthroscopy will require a paradigm shift in the design and reporting of trials in the military health system.
Keywords
Women, in general, are poorly represented in exercise and sports medicine research. 11,16,34,51 The shift within the past decade to open combat military occupations to individuals of both sexes elevates the importance of understanding sex-specific outcomes in this setting. Women make up approximately 15% of all military servicemembers 13 and 10% of servicemembers who are deployed. 3 Research has shown that females in the military have up to 3 times greater risk of sustaining lower extremity musculoskeletal injuries than their male counterparts. 9,58 This has led to symposiums, 53 task forces, 29 and calls for a greater research focus on the issue of injuries in female military servicemembers. 35 These calls align strongly with a push to improve research on sex-based disparity in general 25 and female athletes in particular, which is currently lacking. 47 The National Institutes of Health (NIH) has stated that the overreliance on male animals and cells can obscure the influence of key sex influences on health processes and outcomes. 40
Nonacute injuries are the most common type of lower extremity musculoskeletal injury. The hip is a commonly injured joint in the lower extremity, most often by stress fractures, and is particularly problematic among female military members. 59 Surgical treatment of nonacute hip pain in young athletes is becoming mainstream, with an 18-fold increase from 1999 to 2009 in the United States. 10 In the Military Health System, hip arthroscopy is rising at similar rates. 46 The data are conflicting on the influence of female sex on outcomes after hip arthroscopy. 22
Given the increased attention on injuries in female military servicemembers, the purpose of this study was to explore differences in outcomes after hip arthroscopy in the military based on sex. The aims were to (1) compare published rates of hip arthroscopy between male and female military servicemembers and (2) determine if there are any sex-based differences in outcomes after hip arthroscopy in the military. The hypothesis was that female patients would have worse outcomes than men.
Methods
Scoping reviews are used primarily to examine the extent, range, and nature of a particular research activity, as well as to identify evidence gaps, provide recommendations for future research, and determine strengths and limitations of a current body of evidence that is often heterogenous and complex (ie, various study designs and outcomes). 2,56 We reviewed the literature to identify the extent of sex-specific reporting in all studies conducting hip arthroscopy on active duty military servicemembers, following the PRISM-ScR guidelines (Scoping Review Extension of the Preferred Reporting Items for Systematic Reviews and Meta-analyses). 55
Search Strategy
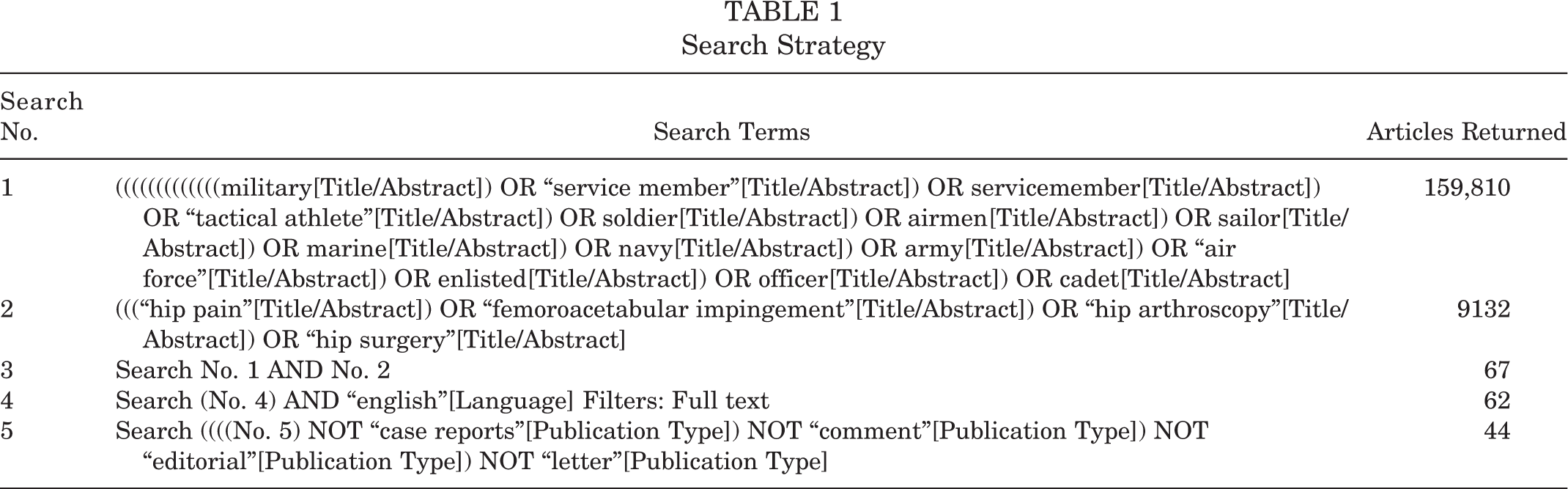
A search of MEDLINE/PubMed, Embase, and CINAHL was conducted for abstracts and titles containing search terms related to hip arthroscopy and active-duty military servicemembers (full search strategy and results are in Table 1). Studies published between January 2000 and December 2020 and available in English full text were included. To increase the homogeneity of the sample, we excluded studies in which hip arthroscopy was performed primarily because of infection, fracture, loose body, avascular necrosis, or osteoarthritis.
Search Strategy
Data Synthesis
Two reviewers (D.R. and A.W.) abstracted the proportion of total female patients and collected all characteristic and descriptive variables categorized by sex when reported. Studies were screened for duplicate publication of the same cohort (i.e., same authors, dates, location, and sample size). The reviewers also identified and noted any results reported by the authors when there was a comparison between men and women. Data were made available from 2 studies 33,46 which allowed further analysis on sex-specific outcomes for those 2 studies. The quality of studies was assessed using the NIH quality assessment tool for observational cohort and cross-sectional studies (rating of good, fair, or poor) 41 and the PEDro quality score for clinical trials (Physiotherapy Evidence Database; range, 1-10, with 10 being the highest quality). 50
Results
The search identified 44 studies for full-text review (Table 1), of which 11 were eligible for inclusion (10 cohort studies and 1 randomized controlled trial) (Figure 1). # The 11 studies represented 2481 patients, of whom 970 (39.1%) were women (Table 2).** Femoroacetabular impingement syndrome was the only diagnosis in 7 of 11 studies 5,14,17,18,33,49,54 and the most common and primary diagnosis in 3 studies, 8,15,46 while labral tear was the primary diagnosis in 1 study. 43 The proportion of women ranged from 25.7% to 57.6%. Dates of surgery ranged from January 1998 through March 2018. Reporting of characteristic and descriptive information was inconsistent, and female-specific characteristic variables were obtained from just 2 studies. 33,46 Only 1 study 33 provided sex-specific data regarding duration of symptoms before surgery (mean ± SD, 3.7 ± 3.9 years for men vs 3.2 ± 2.7 years for women). There was the potential for redundancy of patients in multiple studies: 1 study 46 included consecutive cases from within the Military Health System from June 2004 through July 2013 (N = 1254), and 2 studies 17,18 with the same author and similar time frames could have used the same data. The methodological quality was poor for 4 cohort studies 8,14,43,49 and fair for 6 studies, 5,15,17,18,46,54 and the PEDro score for the 1 clinical trial was 8 of 10.

Flow diagram of study inclusion.
Descriptive Data for All Studies Included a

a CS, cross-sectional; NR, not reported; prosp, prospective; RCT, randomized controlled trial; retrosp, retrospective.
b Overall sample size included 13 civilians.
c Female-only data reported as No. (%) of females.
There was large heterogeneity of outcomes, with return to duty being the most common primary outcome (3 studies 5,17,43 ) (Table 3). Some form of subgroup analysis by sex was performed in 6 studies, and data extracted from 2 studies 33,46 provided sex-specific outcomes for a total of 8 of 10 studies. None of the studies specified differences in sex as the primary outcome and therefore were likely not powered to answer this question. Women had higher rates of medical disability and lower return-to-duty rates in 2 studies assessing these outcomes 43,54 ; there was no difference in return-to-duty rates between the sexes in 1 study (odds ratio = 1.30; 95% CI, 0.55-3.09; P = .551) 15 ; and 1 study cited a higher return-to-duty rate for women. 33 There were no differences in pain and disability between the sexes in 3 studies that provided these sex-specific self-reported outcomes. 5,17,33
Sex-Specific Outcomes for Included Studies a

a ADL, activities of daily living; FAA, Functional Activity Assessment; HOS, Hip Outcome Score; iHOT-33, 33-item International Hip Outcome Tool; MEB, Medical Evaluation Board; mHHS, modified Harris Hip Score; NAHS, Non-arthritic Hip Score; OR, odds ratio; VAS, visual analog scale.
b More than 1 outcome listed indicates that no measure was listed as the primary outcome.
Rhon et al 46 had the largest cohort (N = 1254), which likely had some of the same patients in the other studies providing data by sex according to the year range from 2004 to 2013. There appeared to be a steady rise in annual rates of surgery for men and women across this 10-year period, with <20 surgical procedures in 2004 and close to 300 in 2013 (Figure 2). Military men in this study 46 had less hip-related medical care in the year before surgery, with a mean 10.9 ± 8.0 visits as compared with 13.7 ± 10.4 in women. In the 2 years after surgery, the mean number of hip-related medical visits did not differ between the sexes, but the mean costs of hip-related medical care were higher for men ($16,233; 95% CI, $15,247 to $17,283) versus women ($13,900; 95% CI, $12,980 to $14,886) (Table 3). Labral repairs were coded equally between sexes (Current Procedural Terminology [CPT] code 29916; 183 [26.8%] men vs 146 [25.6%] women), but femoroplasty and acetabuloplasty occurred at a higher rate in men than women (CPT 29914, 224 [32.8%] vs 80 [14.0%] for femoroplasty; CPT 29915, 141 [20.6%] vs 74 [13.0%] for acetabuloplasty, respectively). These data represent patients who remained in the health system for a minimum of 2 years and, because CPT codes 29914 to 29916 were introduced in 2011, allow for representation of these latter procedures in just 2 of the 10 years of study surveillance. Many patients may have been medically separated before 2 years after surgery; therefore, this sample may not be representative of all individuals undergoing hip arthroscopy in this setting.
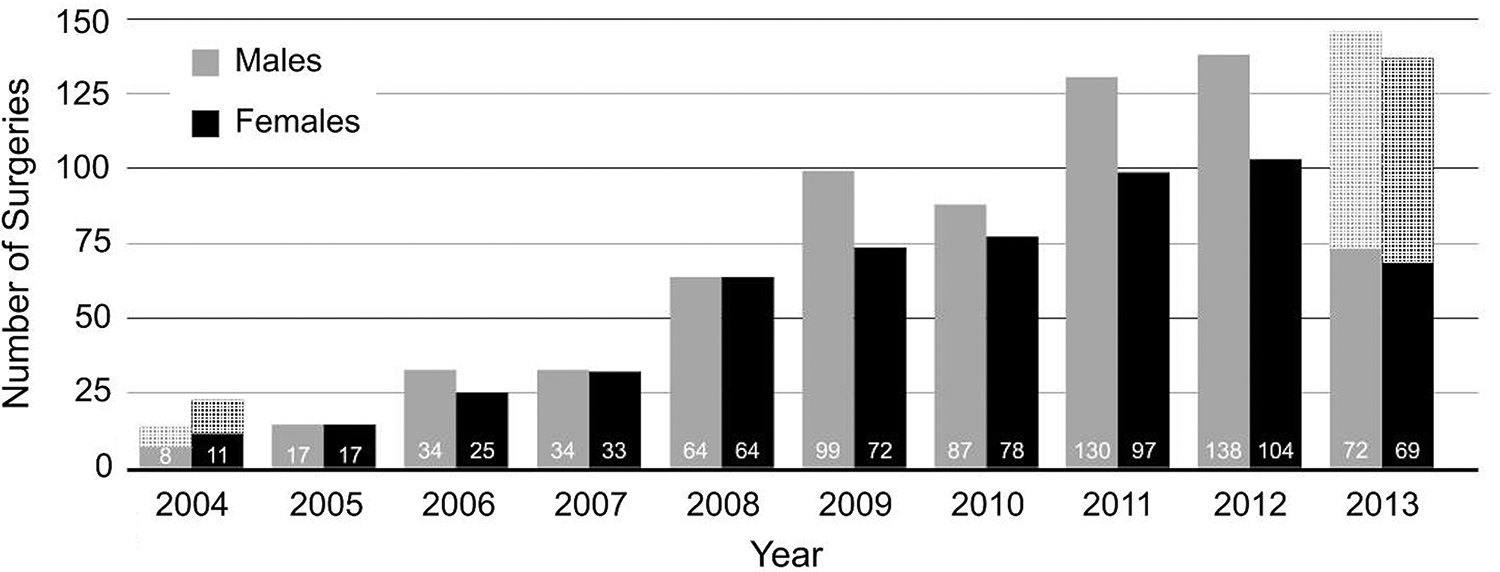
Annual proportion of surgical cases compared by sex. Annual count of cases (unique individuals) between June 30, 2004, and July 1, 2013. Hatched bars indicate annual estimates for partial years based on caseload available during that year (2004 and 2013). Data based on N = 1254 from 1 study. 46
Discussion
This review revealed poor reporting for sex-specific outcomes in studies on hip arthroscopy conducted in military servicemembers. Only 2 studies noted baseline and characteristic variables according to sex, and just 1 study cited duration of symptoms before surgery according to sex. The ability to characterize female patients undergoing surgery in this setting is limited by poor reporting of these variables in the current literature. To maintain a high level of quality in clinical research, the NIH expects that sex will be factored into research design, analysis, and reporting of all human studies. 40 Despite representing only 15% of the total military force, 44 females accounted for 39.1% of the patients undergoing hip arthroscopy in these studies. This leads to 2 possible conclusions based on the available data. (1) There is a much higher rate of military women developing chronic hip pain disorders. (2) The rate and severity of hip disorders are equal between the sexes, but women are much more likely than men to undergo surgical correction for this condition (i.e., men are more likely to use nonsurgical treatment). Either conclusion leads to a large and relevant disparity between male and female military servicemembers and highlights the need to conduct research appropriately designed to better understand this apparent disparity. There is also the possibility that currently published data do not reflect the actual caseload seen. Some studies excluded patients without at least 1 or 2 years of eligibility in the health system. In other settings, a recent systematic review concluded that female sex was predictive of negative outcomes after arthroscopy for femoroacetabular impingement, 52 making this a relevant question within the military population. This is the first study to our knowledge providing rates of surgery proportional to the population. 52
Hip arthroplasty is another common procedure with rates in the veteran population that do not differ between men and women. 6 However, these figures came from the Veterans Health Administration based on patient empanelment rather than the veteran population in general. The surgical rate in proportion to the population rate of women could have been higher. A history of disparities in women’s health services for veterans has also been identified, 30 which could account for reduced numbers undergoing surgery in comparison with the veteran population at large. Rates for sustaining an orthopaedic injury appear to be higher in active-duty women than men, although some studies show that the difference is substantially reduced when physical fitness levels are accounted for. 19,39 A survey from the general population revealed that women have higher rates and severity of osteoarthritis but are less likely to undergo arthroplasty than men. 23 The opposite appears to be true with hip arthroscopy in the military. Prior hip arthroscopy may increase complication rates during hip arthroplasty, 57 yet other outcomes may not be worse. 24 With hip arthroscopy rates on the rise over the past 20 years in the United States, the impact on the future of hip arthroplasty in veteran populations is unknown.
Despite the anecdote and perception that women in the military have worse outcomes than men, the available evidence does not support this. Perhaps this sentiment is carried over from findings in civilian cohorts, where older female patients were reported to have worse outcomes. 20,21 Age was a predictor of poor outcomes in those studies, with younger women often doing much better than older women (those aged ≤30 years having the best outcomes). 20,21 A study of patients (N = 229) undergoing hip arthroscopy with a mean age of 31.6 years demonstrated no differences in outcomes between the sexes at 2 years. 28 Younger women, especially athletes, are more likely to return to sport after hip arthroscopy than older nonathlete women (mean age, 19.1 years for athletes vs 39.3 years for nonathletes). 20 The mean age of women in the studies in our review ranged from 28.5 to 31.0 years (there were only 2 studies with these data). 33,46 One study in our review postulated that lower return-to-duty rates in women were due to a less experienced surgeon. 54 Because the studies in the present review were not powered to answer this question, a critical gap in the literature remains. Most studies did not stratify characteristic variables by sex or age, limiting the extent of subgroup analyses. The findings from the present review highlight the need for research that aims to identify and address disparities in sex-specific outcomes for chronic hip pain.
It seems reasonable to conclude that hip injury rates are higher in women. Several studies have revealed an increased incidence of lower extremity stress fractures in military women versus men, attributing this disparity to lower fitness levels in female recruits upon entering military service. 31 This places individuals at an increased risk for injury as the rapid rise in training load during basic training may exceed the body’s biological capability to adapt. Other risk factors for stress fractures in military women include reduced muscle mass and wider pelvic breadths, which place increased stress on the hips and knees. 59 Women with lower extremity stress fractures additionally have increased rates of anemia and iron deficiency as compared with their male counterparts. 37 These same risk factors may explain the increased incidence of femoroacetabular impingement syndrome in women, as the excessive load leading to stress fracture is also occurring at the acetabulum with the body’s inability to offset load through sufficient muscle mass. The ability to compare percentage load and total body mass between the sexes would be insightful, as women may be incurring greater stress than men owing to the weight of military equipment making up a greater percentage of body mass. In addition, there are morphological differences in hip anatomy that may influence the onset and progression of pain. 26
The ability to compare male and female fitness levels as a confounder to injury risk would be valuable. Many differences exist in strength and lower extremity kinematics between men and women. 32 Female athletes had better outcomes after hip arthroscopy than nonathletes in 1 study, 20 strengthening the argument that fitness levels may be an important consideration when determining prognosis. In other military cohorts, an almost equal proportion of injury rates between men and women was seen after adjusting for occupational demands and levels of fitness. 1,4 Age- and occupation-adjusted discrepancies between cardiorespiratory and muscular performances exist between men and women in the military, and this could be another target for injury-reduction programs. 12
If injury rates were the same between sexes but surgical correction was a more common treatment for women, it could highlight a potential disparity in treatment approaches based on sex. Surgical selection bias is a possibility. 36 Utilization rates of some interventions were different between the sexes. While there is no comparison with controls who did not have hip surgery, women were much more likely than men to use physical therapy services in the year before surgery (N = 1254; 63.7% vs 56.5%, respectively). 46 Women also sought more care in general for the hip before surgery i.e., visits and referrals). One study indicated poorer hip function before surgery in women over men, 28 which could explain the greater medical care utilization before surgery.
Surgical approaches were different between the sexes, with men undergoing a higher proportion of femoroplasty and acetabuloplasty procedures in 1 study. 46 Female sex has been identified as a risk factor for hip arthroscopy failure, 42 although 1 study in this review 46 noted that revision rates were no different between men and women in the military. Again, definitive conclusions are limited by the fact that none of the studies were designed to properly answer these questions.
Certain comorbidities can moderate outcomes after orthopaedic injury. 7,38,45 A higher prevalence of comorbidities in women could help explain higher rates of disability from chronic hip pain. One study in our review (N = 469) cited a strong correlation between women not returning to duty and the presence of an Axis I psychiatric disorder, a higher correlation than found in men. 54 Data from another study (N = 1254) revealed that women were more likely to have a mental health disorder diagnosis after surgery (43.7% women vs 33.2% men). 46 Military women were also more likely to receive a concurrent chronic pain diagnosis after surgery (30.5% vs 21.7%). 46 Reporting prevalence of comorbidities by sex may help improve our understanding of any potential disparities in outcomes.
Other factors may help identify reasons for the disproportional rates; however, most characteristic variables were missing or not reported by sex in current studies. For example, socioeconomic status is a known predictor of chronic opioid use after surgery in military populations, 27,48 but these data were not presented by sex in most studies included in this review. One study (N = 1254) found a higher rate of women than men in the junior enlisted category (31.9% women vs 21.1% men) but a higher rate of men in the senior enlisted category (59.2% men vs 43.5% women). 46 Some of these factors may better explain the discrepancy in hip arthroscopy rates between the sexes, and future studies should consider improved reporting of these data.
Limitations
These findings may not generalize to other settings, even in the military (the majority took place in the United States). Several studies excluded patients without a minimum of 1- to 2-year follow-up, which would exclude cases that separated from the military before this point. Other studies in this setting indicated that 45.8% of participants were no longer in service 2 years after surgery 33 and just 39% returned to service after surgery. 54 Variations in disability evaluation systems likely also exist within individual service (e.g., army vs navy), and even different occupations within the same military service will have unique considerations associated with being able to return to full duty. Several studies in this review used retrospective data based on procedure and diagnostic codes. These values have evolved over the 20-year period represented across these studies, possibly changing the specificity of the data over time. However, these limitations would likely not influence just 1 sex, meaning that any potential bias would affect rates equally between the sexes. Substantial heterogeneity in outcomes across these studies made comparisons difficult, and no studies were powered to examine between-sex differences.
Conclusion
Hip arthroscopy appears to occur in a much higher proportion of female than male military servicemembers. Women account for approximately 15% of the active duty military but make up 40.1% of all servicemembers who undergo this procedure, highlighting the importance of studies designed to properly understand this disparity. Based on limited and low-quality evidence, there does not appear to be a disparity in outcomes between men and women. This review serves as a call to improve the quality of research addressing the apparent disparities in hip arthroscopy for female servicemembers to ultimately improve their outcomes.
Footnotes
Final revision submitted June 6, 2021; accepted August 4, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding was received from an internal grant from the US Defense Health Agency (W911QY-15-1-0016 to D.I.R.). This work was also supported in part by the Uniformed Services University, Department of Physical Medicine and Rehabilitation, Musculoskeletal Injury Rehabilitation Research for Operational Readiness (HU00011920011). J.F.D. has received education payments from Supreme Orthopaedic Systems and nonconsulting fees from Arthrex. D.I.R. has received royalties from Medbridge and is the owner of Clinically Relevant Technologies. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.