
Abstract
Background:
Ligamentum teres (LT) reconstruction is an appropriate alternative in select cases of LT full-thickness tears, resulting in hip micro- or macroinstability. Graft fixation at the acetabular fossa is critical to achieving the best functional results.
Purpose:
The purpose of this study is to compare the pullout strength of 2 graft fixation methods used for LT reconstruction of the hip.
Study Design:
Controlled laboratory study.
Methods:
In 7 cadaveric specimens, the acetabular socket was prepared after the native LT was transected and the femoral head was removed. Seven separate tibialis anterior grafts were then prepared by suturing a running-locking No. 2 suture on each tail of the graft. Three specimens had fixation of the graft to the acetabulum using an adjustable cortical suspension suture button; the remaining 4 were fixed to the acetabulum using a knotless suture anchor. Specimens were then mounted onto a custom jig within a mechanical test frame to allow for the in-line pull of the graft fixation construct. After a preload of 5 N, each specimen was loaded to failure at 0.5 mm/s. Stiffness and load to failure were measured for each specimen construct.
Results:
Suture button fixation had a higher mean load to failure when compared with the knotless anchor fixation method (mean ± SD, 438.1 ± 114.3 vs 195.9 ± 50.0 N; P = .01). There was no significant difference in mean stiffness between the methods of fixation (24.5 ± 1.4 vs 26.5 ± 5.8 N/mm; P = .6).
Conclusion:
In this cadaveric study, the suture button fixation demonstrated greater load to failure than the knotless anchor fixation.
Clinical Relevance:
Results of this study can guide surgical decision making when selecting an acetabular fixation method for LT reconstruction.
There has been an exponential increase in the number of hip arthroscopy procedures being performed annually. 14,18 With this increase, the prevalence of numerous, previously undescribed pathologies has been revealed, including that of ligamentum teres (LT) tears. Partial or complete tearing of the LT has been treated with debridement 2,10 ; however, a subset of patients continues to experience hip instability attributed to this injured structure. 6 In the past decade, there has been growing interest in the functional importance of the LT, 15 especially concerning its contributions to complex hip instability. 3,6,8 While debridement is a valid treatment option in cases of partial tearing, arthroscopic LT reconstruction is an appropriate alternative in select cases of full-thickness tears. 2,5,9,11,12,20,26
Increased prevalence of LT tears is noted in the setting of borderline dysplasia, generalized ligamentous laxity, and female sex. 6,8,13 The presence of LT tears may indicate advanced instability and portend slightly inferior outcomes in patients with borderline dysplasia who received arthroscopic labral treatment, femoroacetabular impingement correction, and capsular plication. Their presence may also be a sign that periacetabular osteotomy treatment is warranted to begin with. 6 In a systematic review on different treatment options for LT tears, the authors concluded that LT debridement may provide short-term relief of hip pain in patients with partial-thickness tears failing conservative management, whereas reconstruction may be more beneficial in cases of full-thickness tears. 24 However, in a 2021 systematic review on LT reconstructions, Shapira et al 25 concluded that current evidence supports LT reconstruction for patients experiencing refractory instability, particularly in a revision hip arthroscopy setting. Nevertheless, there is a paucity in the literature regarding biomechanical data on the LT itself, and, to date, no biomechanical study has been performed evaluating the pullout strength of acetabular fixation methods of LT reconstruction grafts. 17 The technical variations in the LT reconstruction fixation choice at the acetabular fossa are subtle but critical to achieve optimal outcomes. 22,23
The purpose of this study was to compare in-line pullout mechanics between 2 possible acetabular fixation methods for LT reconstruction: an adjustable cortical suspension suture button versus a single 3.9-mm polyether ether ketone (PEEK) suture anchor. We hypothesized that the suture button fixation would have better in-line load to failure when compared with suture anchor fixation.
Methods
The study sponsor provided in kind 8 fresh-frozen nonpaired cadaveric specimens (Science Care) from the limbs of donors with no preexisting medical history of structural hip joint abnormalities and/or previous surgery. All specimens were thawed to room temperature and dissected to the hip joint with the removal of all surrounding tissue, including the muscle and capsule. The native LT was then transected, and the femoral head was removed. The entire native acetabulum was isolated in continuity, including the pubic ramus, ilium, and ischium, and mounted in a custom testing device. The pulvinar was excised, consistent with prior descriptions of LT reconstructions, 2,5,9,11,12,20,26 to allow for optimal visualization of the cotyloid fossa for placement of the button or anchor fixation device. Eight separate tibialis anterior allografts were prepared by suturing a running-locking No. 2 suture (FiberWire; Arthrex) on each tail of the graft. Specimens were then mounted on a custom jig within a mechanical test frame (MTS Systems) to allow for the in-line pull of the graft fixation construct, eliminating any angular or torsional torque. Four randomly selected specimens were prepared with an adjustable cortical suspension suture button (BicepsButton; Arthrex), and the remaining 4 specimens were prepared with a PEEK 3.9-mm knotless anchor (Corkscrew; Arthrex) per prior surgical technique and manufacturer-recommended instructions.
For the suture button group, the graft was doubled over, and a No. 2 nonabsorbable braided suture (FiberWire) was looped through the middle of the graft. This suture was then passed through the button with a Keith needle to allow the tension-slide mechanism to work as designed. To avoid injury to the obturator neurovascular bundle, a 3.2-mm pilot hole was drilled bicortically through the medial wall in the posteroinferior quadrant of the cotyloid fossa, consistent with prior technique descriptions. 5,9,11,12,20 The button was placed on the inserter, pushed through the pilot hole, and deployed on the inner cortex of the quadrilateral plate. The suture tails were then tensioned, pulling the end of the graft flush with the cotyloid fossa. The graft was secured by tying 5 alternating half-hitches, pushing the knot as deep into the tunnel as possible.
For the anchor group, a 3.1-mm unicortical pilot hole was drilled in the posteroinferior quadrant through a drill guide, and the 3.9-mm knotless PEEK anchor was inserted and screwed into place. Excellent anchor fixation was noted in all specimens. The No. 2 repair suture was then passed through the looped portion of the doubled graft. The repair suture was shuttled through the passing suture loop and into the anchor’s locking mechanism. The repair suture was then maximally tensioned, with the graft pulled flush with the cotyloid fossa.
Each specimen was securely mounted in the fixture within the mechanical test frame, with the graft tails secured between the serrated grip faces of the dovetail clamp, while the attached sutures were looped through the clamp and tied as backup fixation (Figure 1). The system was tared with the graft completely slack, and slack was removed from the system by applying a nominal preload of 5 N in tension. After the preload, each specimen was loaded to failure at 0.5 mm/s. Stiffness was calculated as the slope within the elastic region (ie, linear region before the yield point) of the load-deflection curve. The MTS actuator was then loaded until failure of the reconstructed specimen in each group. The load to failure was measured as the maximum load achieved before failure, indicated by an unrecovered decrease in load. Mode of failure was also recorded for each test.

Test setup showing (from top to bottom) test frame actuator, dovetail clamp, ligament graft, mounted acetabulum, base, and load cell.
Statistical Analysis
The stiffness of the construct in each specimen and the measured changes in load to failure between the tested conditions were compared among the specimens. Groups were compared statistically using an unpaired 2-tailed Student t test, with statistical significance set at P ≤ .05.
Results
A single specimen from the suture button group was excluded from the study owing to early failure of the construct during the mechanical testing protocol, leaving 3 specimens in the suture button group and 4 in the PEEK knotless anchor group. The mean age of the remaining 7 specimens was 56 ± 6 years (the same for each group; P = .9). The suture button fixation method had a significantly higher load to failure as compared with the knotless PEEK anchor fixation method (438.1 ± 114.3 vs 195.9 ± 50.0 N; P = .01) (Table 1, Figure 2). Furthermore, all specimens within the suture anchor group had lower loads to failure than the lowest specimen in the suture button group. There was no significant difference in mean stiffness between the methods of fixation. Individual specimen data are presented in Table 2.
Age, Stiffness, and Load to Failure Between the Button and Anchor Groups a

a Data are reported as mean ± SD. Bold P value indicates statistically significant difference between fixation methods (P < .05).
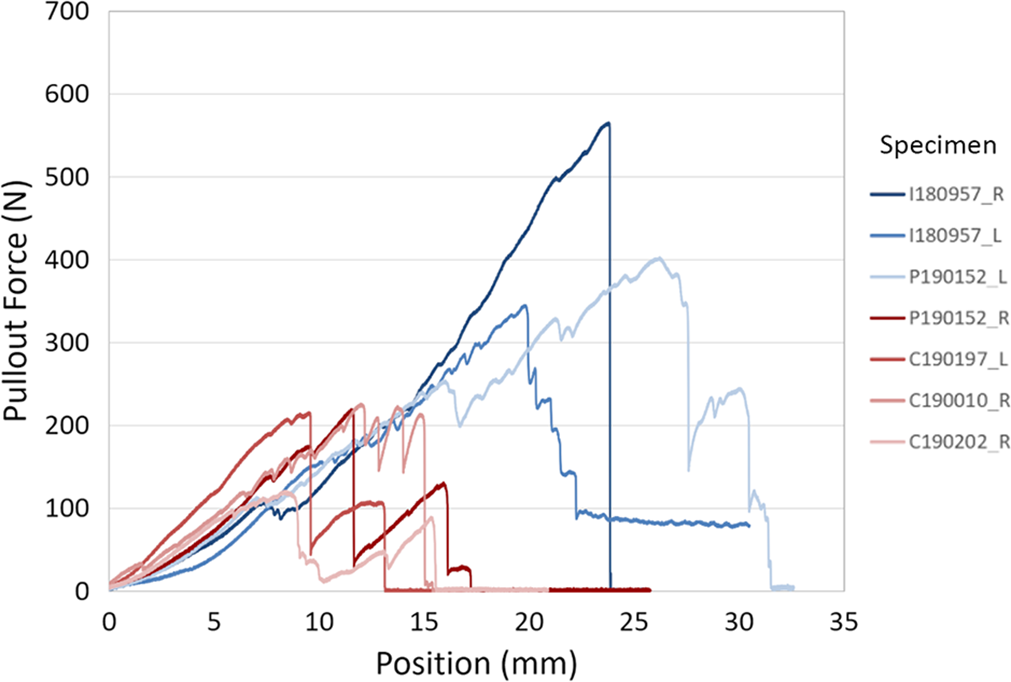
Load-to-failure plots as a function of actuator position between the methods of fixation across the specimens. Blue, button group; red, anchor group. L, left; R, right.
Characteristics, Methods of Fixation, and Biomechanical Properties Across Specimens a

a All specimens were male. L, left; R, right.
Discussion
This cadaveric study highlighted the differences in load to failure between the methods of LT reconstruction graft fixation at the acetabulum. The suture button–type fixation demonstrated significantly higher load to failure than the knotless PEEK anchor fixation. There was no significant difference in mean stiffness between the methods of fixation. To our knowledge, this is the first study comparing the different methods of graft fixation utilized in LT reconstruction on the acetabular side.
A few previously published cadaveric studies highlighted the quantitative anatomy 17 and functional biomechanical properties of the LT. 3,15 Mikula et al 17 reported the LT to have 6 distinct points of attachment on the acetabulum, with the ischial attachment at the 8:07 clockface position having the largest cross-sectional attachment area. According to Martin et al, 15 the LT provided restraint to terminal internal and external rotations of the hip in deep hip flexion (beyond 90°). Also, the LT has been shown to serve as a secondary hip stabilizer, restricting subluxation in high flexion, adduction, and external rotation. 3 Although there are no data on existing loads on the LT during normal activities, the LT with its native attachments achieved a mean yield load of 75 N and ultimate failure load of 204 N according to a cadaveric study by Philippon et al 21 that verified LT structural properties. The measured load to failure across the LT-reconstructed specimens in our study was much higher than what was noted in this study, emphasizing that either technique would be sufficient.
Advancement in arthroscopic techniques to address intra-articular pathology of the hip has led to the increased understanding of how the LT tear plays a role in complex hip instability. 3,6,15 Persistent instability after a failed hip arthroscopy with anterior capsular plication or capsular reconstruction is a specific indication, provided that another intra-articular pathology has been addressed. 9,20,22 Simpson et al 26 were the first to describe their technique for LT reconstruction in 2011; later, several reports were published with technical variations. 9,11,12,20 This procedure is technically demanding with a steep learning curve and is therefore more frequently undertaken at certain high-volume centers. 9,19,20,22 The short-term outcome results for LT reconstruction are promising in appropriately selected patients. 7,19,20,22,24
Techniques have varied in fixation and graft choice, ranging from the use of knotless anchors, knotted anchors, or suture buttons on the acetabular side in combination with semitendinosus allograft, tibialis anterior allograft, or iliotibial band autograft. 11,12,20,26 Based on the concept of safe zones for transacetabular drill holes presented by Wasielewski et al, 27 the optimal position for the drill holes required for LT reconstruction is in the posteroinferior and posterosuperior quadrants of the acetabulum in an effort to avoid injury to obturator neurovascular bundle. In a cadaveric study, Brady et al 5 showed that when the acetabular tunnel was drilled through the femur, placing the femur in 15° of internal rotation and 15° of abduction successfully avoided the obturator vessels in 100% of cases. Most surgical techniques suggest using the posteroinferior portion of the cotyloid fossa as the primary anchor point for acetabular fixation. 1,11,20,26 All but 1 technique 6 suggest drilling the femoral tunnel through the lateral cortex of the femur. This tunnel may then be used for the preparation and drilling of the acetabular tunnel. The drill depth and direction are equally important in the acetabular-side LT graft fixation. The drill that is meant for either the anchor or the suture button should not be directly aimed medially or anteriorly in the pulvinar area, to avoid the obturator vessels that traverse the quadrilateral plate reaching the obturator foramen. If the drill is placed in these high-risk regions, the depth is entirely determined by the thickness of the quadrilateral plate.
Collectively, the aforementioned studies examined several important aspects of LT reconstruction that led to an increased body of evidence favoring this procedure; however, there is a lack of consensus in the literature regarding the method of graft fixation at the acetabulum. Furthermore, the literature lacks quantitative biomechanical data regarding the pullout strength of the LT reconstruction graft. Per the description from the manufacturer (Arthrex), the fixation strength for the PEEK knotless anchors is 800 N for 5-mm displacement, determined as load to failure in the cadaveric study, and 375 N for ultimate load, using a foam block study; for adjustable-loop suture, the ultimate load to failure is 357 N. According to Mickelson et al, 16 the adjustable-loop cortical button had a time zero failure load of 700 N. According to Barber et al, 4 who reported on suture anchors for single-pull load-to-failure strength, the mean cortical failure loads were in the order of 386 N for Corkscrew FT III, 712 N for SwiveLock C, and 168 N for PEEK SutureTak. In this study, we found significant differences in mechanical behavior by comparing the 2 common graft fixation methods utilized in LT reconstruction at the acetabulum. Specifically, this study identified that suture button–type fixation has greater load to failure (438 N) than the knotless PEEK suture anchor fixation (196 N). While it is possible that the aged specimens, with their differences in bone density, could be a reason for these differences in observation compared with the knee literature, one cannot rule out the role played by differences in soft tissues (tibialis anterior tendon vs patellar tendon).
Owing to the nature of this study as an evaluation of the biomechanical properties of cadaveric specimens under controlled conditions, limitations are inherent. The small sample size in our study is a limitation, and we had little control over specimen age and sex. We agree that specimens comparable to populations at risk would have been younger and female. Instead, to mitigate issues with specimen failure attributed to bone density, male specimens without prior hip conditions and with similar age ranges were chosen. Since our intention was to isolate the effects of LT reconstruction graft fixation methods at the acetabulum, the native LT, femoral head, and all other soft tissues were removed from the specimens. For the same reason, femoral-side fixation was not included to specifically evaluate acetabular aspects of graft fixation while avoiding the additional confounding effect of graft fixation in the femoral head, which is potentially weaker than acetabular fixation.
Although the current literature does mention variability in acetabular-side LT graft fixation with single–suture button versus 2-anchor repair, we chose a single anchor versus button (akin to knee anterior cruciate ligament literature comparing cortical and aperture fixation) to provide a head-to-head comparison while limiting the number of confounding variables. It is possible that 2-anchor fixation constructs might have better mechanical properties; however, they are technically more challenging and are likely associated with increased neurovascular injury risk. We acknowledge that the LT reconstruction in-line pullout strength testing method that we utilized in this study is not representative of a true mode of failure in vivo; however, it was felt to be the most reproducible method for biomechanical testing during our head-to-head comparison. Additionally, it is possible for the construct to fail at different positions other than what was observed in our study, if the graft was handled in another manner (eg, suture abrasion against the tunnel could result in suture button fixation failure). Also, testing of cadaveric specimens demonstrates biomechanical properties of graft fixation strength at time zero but does not account for the progressive degeneration or healing that occurs in actual patients.
Conclusion
This cadaveric study examined differences in pullout strength between the methods of acetabular-side graft fixation that are commonly utilized in LT reconstruction. The suture button–type fixation demonstrated greater load to failure than the knotless PEEK anchor fixation. Results of this study can help guide surgical decision making when selecting an acetabular fixation method for LT reconstruction.
Footnotes
Acknowledgment
The authors thank Dr Glenn Fleisig, Chandler Harris, and Harrison Reich for their contributions to this study.
Final revision submitted July 22, 2021; accepted August 2, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was sponsored by Arthrex in the form of direct funding as well as in kind donations of cadaveric specimens and surgical products used in the completion of the study aims. A.C.L. has received research support from Arthrex, Stryker, and Medacta; education payments from Arthrex, Medwest, and Smith & Nephew; consulting fees from Arthrex and Graymont Medical; and hospitality payments from Zimmer Biomet. M.K.R. has received research support from Arthrex, education payments from Smith & Nephew, and hospitality payments from Prime Surgical. R.P.R. has received research support from Arthrex and education payments from Arthrex and Smith & Nephew. P.J.R. has received hospitality payments from Arthrex, Stryker, and Smith & Nephew. D.R.M. has received hospitality payments from Arthrex, Stryker, and Smith & Nephew. B.A.E. has received consulting fees, nonconsulting fees, and royalties from Arthrex. B.G.D. has received research support from Arthrex, ATI, Stryker, and Pacira Pharmaceuticals; education payments from Arthrex, Breg, and Medwest; consulting fees from Adventist Hinsdale Hospital, Arthrex, MAKO Surgical, Medacta, Pacira Pharmaceuticals, and Stryker; speaking fees from Arthrex and Pacira Pharmaceuticals; honoraria from Medacta; and royalties from Amplitude, Arthrex, DJO Global, MAKO Surgical, Medacta, Stryker, and Orthomerica. B.G.D has also had ownership interests in Hinsdale Orthopaedics, the American Hip Institute, SCD#3, North Shore Surgical Suites, and Munster Specialty Surgery Center. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.