
Abstract
Background:
Knowledge of clinical outcomes and return to artistic activities after endoscopic shelf acetabuloplasty (ESA) for acetabular dysplasia in artistic athletes is lacking.
Hypothesis:
Hip arthroscopic surgery including ESA will enable artistic athletes to return to their activities with a high success rate, significantly improved acetabular coverage, and preserved joint cartilage.
Study Design:
Case series; Level of evidence, 4.
Methods:
We reviewed 28 hips in 23 female artistic athletes (14 ballet, 9 rhythmic gymnastics, 4 dance, and 1 baton twirling) who underwent arthroscopic labral preservation, capsular plication, and ESA. Their mean age was 25.8 ± 10.2 years. Preoperatively, all patients had generalized joint laxity (Beighton score, 7.1 ± 1.8). We evaluated preoperative and postoperative radiographs and outcome scores including the modified Harris Hip Score (mHHS), Nonarthritic Hip Score (NAHS), International Hip Outcome Tool 12 (iHOT-12), Vail Hip Score (VHS), and Hip Outcome Score–Sports (HOS— Sports). Statistical analysis was performed using paired t tests and Bonferroni correction.
Results:
The mean follow-up was 32.5 ± 12.5 months. The mean lateral center-edge angle significantly increased from preoperatively (15.7° ± 5.3°) to postoperatively (39.8° ± 8.2°; P < .001) and at the final follow-up (33.7° ± 8.6°; P < .001). The vertical-center-anterior angle significantly improved from preoperatively (16.2° ± 8.8°) to final follow-up (33.6° ± 8.0°; P < .001). All hips maintained a Tönnis grade of 0 or 1 at the final follow-up. Overall, 20 patients (87%) were able to return to their preinjury level. All outcome scores improved from preoperatively to postoperatively: mHHS, from 68.5 ± 18.1 to 88.3 ± 18.5; NAHS, from 50.8 ± 17.7 to 69.0 ± 11.4; iHOT-12, from 36.9 ± 19.3 to 75.2 ± 19.8; VHS, from 53.8 ± 13.7 to 79.4 ± 19.4; and HOS--Sports, from 59.9 ± 17.0 to 79.6 ± 21.3 (P < .001 for all). In total, 3 patients could not return to artistic activities as the result of postoperative deep gluteal syndrome.
Conclusion:
ESA concomitant with labral repair, cam osteoplasty, and capsular plication to treat dysplastic hips in patients with joint laxity enabled artistic athletes to return to their activities with a high success rate.
Keywords
Artistic sports such as dance require an extreme range of motion (ROM) of the hips. 4 Repeated exposure to extreme hip ROM in artistic athletes with underlying bony deformities can result in chondrolabral injuries, predisposing individuals to osteoarthritis (OA) of the hip joint. A higher prevalence of radiographic hip OA has been reported in retired ballet dancers than in the general population. 13
A systematic review reported that 128 of 462 professional dancers had hip/groin injuries, for an injury rate of 27.7%. Of 1539 student dancers, 217 hip/groin injuries were recorded, for an injury rate of 14.1%. 21 Harris et al 6 reported the prevalence of cam deformity and hip dysplasia in a series of 47 dancers; 89% of dancers had hip dysplasia or borderline hip dysplasia, with significantly greater prevalence in female dancers than male dancers. To address intra-articular pathologies, including cam deformities and labral tears in artistic athletes, hip arthroscopic procedures are truly invaluable. A previous case series study showed that >90% of active patients were able to return to their activity after endoscopic shelf acetabuloplasty (ESA). 22
In addition, recent studies have shown that ESA is less invasive than periacetabular osteotomy (PAO) and also enables active patients to return to their preinjury level of sports activity. 22 A recent surgical technique report described the case of a rhythmic gymnast with a rim stress fracture in the setting of acetabular dysplasia who returned to play after ESA concomitant with fragment fixation, labral repair, and shoelace capsular plication. 24 However, the existing literature lacks a clear explanation of the effectiveness of ESA for acetabular dysplasia in artistic athletes.
The purpose of this study was to investigate clinical outcomes and return to artistic activities after ESA combined with labral repair and capsular plication for the treatment of acetabular dysplasia in artistic athletes. It was hypothesized that hip arthroscopic surgery, including ESA, would enable these athletes to return to artistic activities with a high success rate, significantly improved acetabular coverage, and preserved joint cartilage.
Methods
The study protocol received institutional review board approval, and all study participants provided informed consent. We retrospectively reviewed the medical records of 273 hips from between 2012 and 2019 in which ESA was performed along with arthroscopic labral preservation, cam osteochondroplasty, and capsular closure; all procedures were performed by a single surgeon (S.U.). A total of 245 hips from nondancers were excluded; thus, 28 hips (23 patients) were eligible for the current study. None of the included patients were lost to follow-up (Figure 1).

Flowchart showing the recruitment of patients with developmental dysplasia of the hip undergoing endoscopic shelf acetabuloplasty (ESA) in this study.
The inclusion criteria were as follows: ESA was indicated for symptomatic acetabular dysplasia, defined as recalcitrant pain in the hip and/or groin unresponsive to nonoperative treatment for a minimum of 3 months (eg, nonsteroidal anti-inflammatory drugs, modification of painful sports and/or hip flexion-related activities, and physical therapy); a lateral center-edge angle (LCEA) of Wiberg of <20° on pelvic anteroposterior (AP) radiographs and/or a vertical-center-anterior (VCA) angle of <17° on false-profile radiographs (Figure 2, A and B); positive provocative maneuvers (anterior impingement and/or flexion abduction external rotation [FABER] tests); and intra-articular pathology, including acetabular labral tears, as detected on 3.0-T magnetic resonance imaging (Figure 2E). Contraindications for hip arthroscopy concomitant with ESA in acetabular dysplasia were an LCEA <0°, excessive femoral torsion, anterior undercoverage, severe OA (Tönnis grades 2 and 3), and Legg-Calve-Perthes disease.
The characteristics of the study patients, including sex, age, involved side, sports, and Beighton scores, are shown in Table 1. Their mean of Beighton score was 7.1 ± 1.8.

Preoperative diagnostic images from an 18-year-old female ballet dancer who presented with right hip pain for 14 months. (A) A pelvic anteroposterior radiograph showed a lateral center-edge angle (LCEA) of 16°, a Tönnis angle of 14°, and a Sharp angle of 48°. (B) A false-profile radiograph showed a vertical-center-anterior angle of 14°. (C) A modified Dunn radiograph showed an alpha angle of 62°, suggesting a cam lesion. (D) A 3-dimensional computed tomography scan showed a shortage of coverage of the lateral acetabulum and the protruding anterior inferior iliac spine. (E) A T2*-weighted coronal magnetic resonance image showed an acetabular labral tear (arrow).
Characteristics of the Included Artistic Athletes (N = 23 patients; 28 hips) a
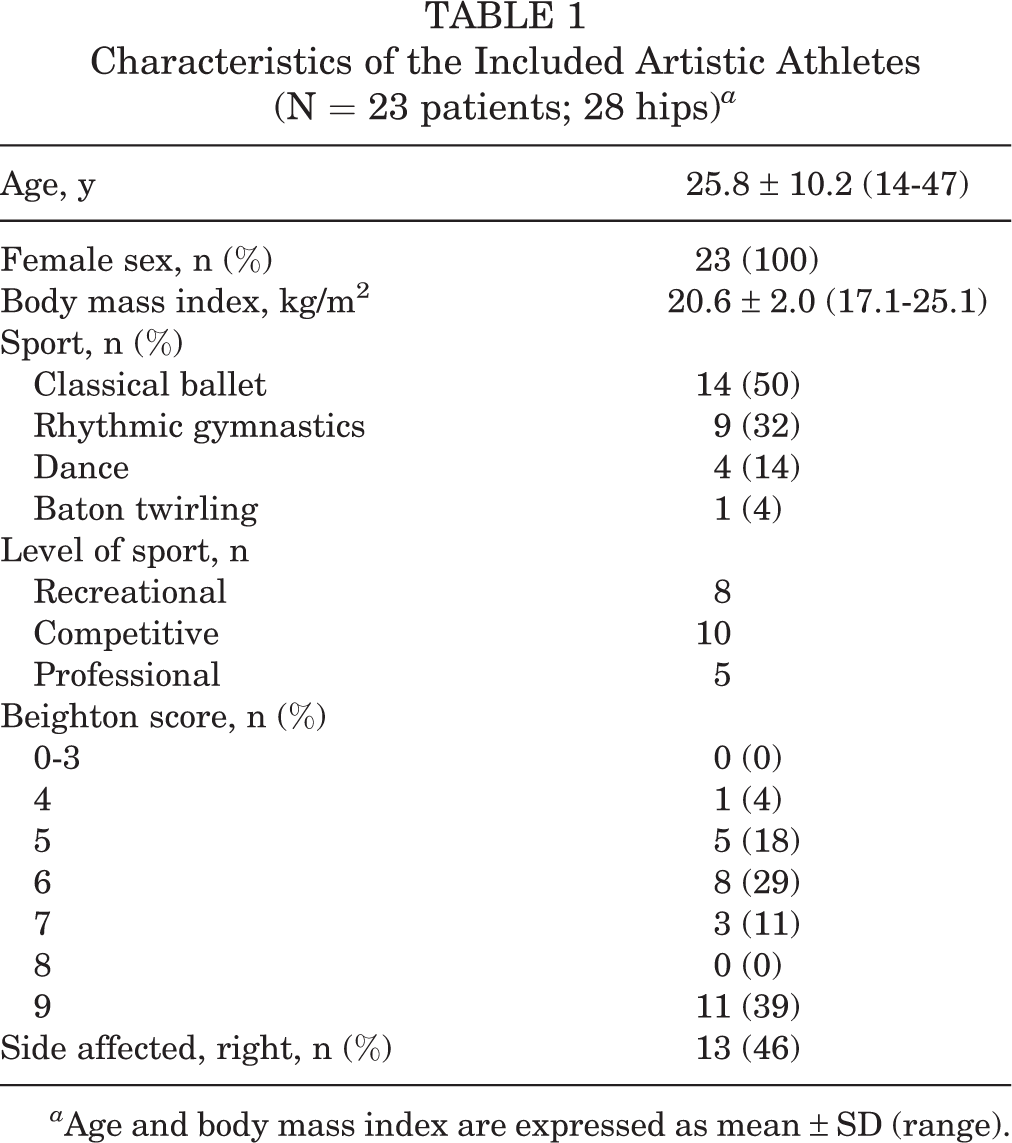
a Age and body mass index are expressed as mean ± SD (range).
Patient-reported outcome (PRO) scores, including the modified Harris Hip Score (mHHS; 100 possible points), Nonarthritic Hip Score (NAHS; 100 possible points), International Hip Outcome Tool 12 (iHOT-12; 100 possible points), Hip Outcome Score–Sports (HOS— Sports; 100 possible points), and Vail Hip Score (VHS; 100 possible points), were evaluated preoperatively and postoperatively at the final follow-up. 27 The minimal clinically important difference (MCID) in the mHHS, NAHS, iHOT-12, HOS--Sports, and VHS was calculated by the distraction method. 14 The passive ROM in flexion and abduction in the supine position and in internal and external rotation in the prone position was examined using a goniometer at the time of visit. The ROM data were recorded preoperatively and at the final follow-up.
Radiographic Evaluation
We assessed the preoperative radiographs of all included hips. All radiographic measurements were manually assessed by 2 authors (H.U. and S.K.) using a picture archiving and communication system. We determined the LCEA, Tönnis angle, femoral neck-shaft angle, Sharp angle, presence or absence of a broken Shenton line on the pelvic AP view, VCA angle on a false-profile view, and alpha angle on a cross-table lateral view or modified Dunn view (Figure 2, A-C). 12,15,28
We also evaluated all preoperative and annual postoperative radiographs for osteoarthritic changes using the Tönnis OA grade classification system. 20 In addition, we determined femoral anteversion and acetabular anteversion on cross-sectional computed tomography. 18
Preoperative Planning
The graft size depended on the preoperative LCEA. We usually insert a shelf graft at least 20 mm in depth in a slot. The remaining lateral side of the graft can contribute to coverage of the femoral head. Thus, we can preoperatively estimate the size of the graft. First, we measured the preoperative LCEA, and then, we attempted to target the postoperative LCEA at approximately 35° (Figure 3).

Preoperative planning. LCEA, lateral center-edge angle.
Surgical Technique
Supine hip arthroscopy was performed with the patient on a traction table under general anesthesia. Anterolateral, midanterior, and proximal midanterior portals were created. An interportal capsulotomy was performed. Intra-articular pathologies, including acetabular chondrolabral damage and femoral head chondral damage, were assessed and documented (Figure 4A). 1 Microfracture chondroplasty was performed if International Cartilage Regeneration & Joint Preservation Society (ICRS) grade 3 or 4 chondral defects were present.

Surgical findings of endoscopic shelf acetabuloplasty. (A) Supine arthroscopic view from the anterolateral portal showing an anterior superior labral tear and suture anchors placed at the acetabulum. (B) The protruding anterior inferior iliac spine was decompressed. (C and D) Labral repair with a suture anchor. (E and F) Arthroscopic view from the midanterior portal showing cam osteoplasty. (G and H) Shoelace capsular closure using Ultratape. (I) A free bone graft harvested from the ipsilateral iliac crest with 2 parallel 1.5-mm Kirschner wires. (J) Four 2.4-mm guide wires were introduced into the planned location of the shelf through the midanterior portal. (K) A cannulated drill was used via the guide wires to make a shelf slot. (L) A free bone autograft was inserted into the slot through the guidewires with press-fit fixation. (M) Anterior view and (N) lateral view on 3-dimensional computed tomography showing the location of the shelf graft.
Next, labral tears were addressed with suture anchor repair (mattress repair) after conservative rim trimming using a motorized bur to create a bleeding bone surface. (Figure 4, B-D). Labral repair was performed using bioabsorbable suture anchors (OsteoRaptor, Smith & Nephew; or Gryphon BR, DePuy Mitek) with knots tied on the capsular side of the labrum. Arthroscopic dynamic examination was performed to assess cam impingement (Figure 4E). When necessary, cam osteochondroplasty using a motorized round bur was performed (Figure 4F). After cam impingement evaluation and femoral osteochondroplasty, capsular plication was performed with the hip at 40° of flexion. Our technique for capsular plication evolved during the study period (Figure 4, G and H). Between 2012 and 2016, we performed side-to-side plication. Between 2016 and 2018, we performed single-shoelace capsular plication. Since 2018, we have performed double-shoelace capsular plication.
ESA was then performed as previously described. 22,24 A 30° arthroscope was positioned in the extracapsular space under guidance with fluoroscopic imaging. After the surgeon identified the straight head and reflected head of the rectus femoris and debrided the latter with a shaver and radiofrequency ablator (DIONICS RF probe; Smith & Nephew), 4 parallel, 2.4-mm guide wires were introduced using the drill guide through the midanterior portal along the anterior acetabular rim adjacent to the capsule (Figure 4J). The surgeon enlarged the slot using a 5-mm cannulated drill for each guide wire. The width of the slot was enlarged with an osteotome to measure approximately 5 to 6 mm in height, 25 mm in width. and at least 20 mm in depth. The optimum width and depth were confirmed using a custom-made dilator. An autologous tricortical bone graft was harvested from the ipsilateral iliac crest (Figure 4I). Two 1.5-mm Kirshner wires were introduced in 1.8 mm—diameter drill holes, helping to control the graft position during endoscopic insertion into the aforementioned anterolateral periacetabular slot (Figure 4I). Finally, the free bone graft was secured at the appropriate position, with the cortical surface facing the femoral head in close contact with the intervening capsule, using a press-fit technique with a cannulated bone tamp (Smith & Nephew) (Figure 4). Under endoscopic guidance, corticocancellous bone chips were inserted above the new shelf.
Postoperative Management and Rehabilitation Protocol
Patients were instructed to use flat-foot weightbearing for the first 3 weeks. If microfracture had been performed, weightbearing limitations were extended to 6 to 8 weeks. Patients were placed in a brace (Philippon hip brace; Bledsoe) for 2 to 3 weeks to protect the hip and limit flexion (0°-120°), abduction (0°-45°), and rotation (external rotation, 0°). Gentle passive ROM exercise was initiated during the first week under supervision of a physical therapist. Circumduction was performed at 70° of hip flexion and neutral hip flexion for the first 2 weeks. Then, continuous passive motion was used to avoid adhesive capsulitis by applying 0° to 90° of hip flexion for up to 4 hours a day for 2 weeks.
During phase 2 (weeks 6-12), patients improved their mobility, stability, and proprioception activity. Endurance strengthening commenced only after the ROM was maximized and good stability in gait and movement was demonstrated. Patients were allowed to progress to phase 3 (weeks 12-16) only if the passive ROM was symmetrical and pain-free and there was a normal gait pattern. Aerobic conditioning was increased using an elliptical machine with a goal of 30 minutes of continuous exercise at low to moderate intensity.
Patients were allowed to progress to physical activity only if the passive ROM was symmetrical and pain-free and there was a normal gait pattern. The goal of phase 4 was to engage in safe and gentle sports drills and prepare patients to return to their artistic or work activities. Gentle sport-specific or work agility exercises were initiated. 19
Statistical Analysis
Statistical analyses of clinical outcomes and radiographic parameters of all 23 patients (28 hips) were performed using SPSS (Version 13; SPSS). Power analysis was conducted using G*Power (Version 3.1; Universität Dusseldorf). The α error was set to .05, and the 1 − β error was set to 0.80.
Paired t tests were used to compare paired nonparametric data, and the Mann-Whitney U test was used to analyze nonparametric paired data. P ≤.05 was considered significant. Power analysis was performed for the initial 6 patients comparing preoperative versus postoperative NAHS. The effect size and sample size were calculated as 2.19 and 5 (actual power [1 – β] = 0.93), respectively. Post hoc power analysis showed that the actual power of this study was 1.0.
The inter- and intraobserver reproducibility of the radiographic measurements was analyzed using the intraclass correlation coefficient (ICC). For intraobserver reliability, a single hip surgeon (S.U.) measured each radiograph 3 times with an interval of at least 1 week between measurements. For interobserver reliability, 2 hip surgeons (H.U. and A.H.) independently reviewed each radiograph and were blinded to the clinical data and details of the radiology reports. The strength of the agreement was interpreted according to Landis and Koch 11 as follows: ICC >0.80, almost perfect; 0.61-0.80, substantial; 0.41-0.60, moderate; and 0.21-0.40, fair agreement.
Results
Inter- and Intraobserver Reliability
The respective inter- and intraobserver ICCs for the measurements were as follows: LCEA, 0.938 and 0.989; Tönnis angle, 0.692 and 0.854; Sharp angle, 0.787 and 0.891, alpha angle, 0.787 and 0.991; and VCA angle, 0.982 and 0.977. Based on the interpretations proposed by Landis and Koch, 11 our measurements showed substantial agreement.
Preoperative Radiographic Assessments
Preoperative radiographic assessments are shown in Table 2. The mean LCEA was 15.7° ± 5.3° (range, 3°-23°), the mean Tönnis angle was 15.2° ± 3.9° (range, 8°-23°), and the mean VCA angle on false-profile view was 16.8° ± 9.0° (range, 2°-32°).
Preoperative Radiographic Assessments

a Reported as number of hips.
Arthroscopic Findings and Operative Procedures
The arthroscopic findings and arthroscopic procedures performed are shown in Table 3. With respect to labral management, all 28 hips underwent labral repair, and no hips underwent labral reconstruction with iliotibial band autografts. All 28 hips underwent femoral osteoplasty for cam impingement: 14 hips underwent side-to-side capsular repair, 12 hips underwent single-shoelace capsular plication, and 2 hips underwent double-shoelace capsular plication. In total, 2 hips with rim stress fractures underwent arthroscopic fragment fixation using bioabsorbable threaded pins, 1 hip with a large bone cyst of the femoral head underwent retrograde bone grafting, and 3 hips required microfracture.
Arthroscopic Findings and Procedures a

a ICRS, International Cartilage Regeneration & Joint Preservation Society; MAHORN, Multicenter Arthroscopy Hip Outcome Research Network.
PRO Scores and Return to Artistic Activities
The final follow-up was at a mean of 32.5 ± 12.5 months (range, 24-72 months). The preoperative and postoperative PRO scores are detailed in Table 4. All scores improved significantly between preoperative assessments and final follow-up (P < .001 for all). The MCID scores (with percentage of patients who achieved MCID) were as follows: mHHS, 9.1 (71.4%); NAHS, 8.9 (75.0%); iHOT-12, 9.7 (85.7%); VHS, 6.9 (85.7%); and HOS--Sports, 8.5 (70.4%). For each PRO score, the average improvement was higher than the corresponding MCID. According to Patient Acceptable Symptom State (PASS) values after hip arthroscopy for femoroacetabular impingement (FAI) as described by Chahal et al, 2 the percentages of patients who achieved PASS on the mHHS and HOS--Sports were 82.1% and 80.0%, respectively.
Patient-Reported Outcome Scores From Preoperative Assessment to Final Follow-up a

a Data are shown as mean ± SD (range). Bolded P values indicate statistically significant difference between preoperative assessment and final follow-up (P ≤ .05; paired t test). HOS, Hip Outcome Score; iHOT, International Hip Outcome Tool; mHHS, modified Harris Hip score; NAHS, Nonarthritic Hip Score; VHS, Vail Hip Score.
FABER significantly improved from preoperatively to the final follow-up. There was no significant improvement in internal rotation (Table 5).
Changes in Range of Motion From Preoperative Assessment to Final Follow-up

a Data are shown in degrees as mean ± SD.
b Bolded P values indicate statistically significant difference between preoperative assessment and final follow-up (P ≤ .05).
All but 3 artistic athletes (87%) were able to return to their preinjury sports level. A total of 3 artistic athletes (2 competitive dancers and 1 recreational dancer) could not return to artistic activities due to postoperative deep gluteal syndrome (DGS) as a complication. 9,23 These 3 patients underwent continued physical therapy and occasional ultrasound-guided injection of 1 mL of 1% bupivacaine and 9 mL of normal saline. One of them underwent surgical decompression of the sciatic nerve and posterior femoral cutaneous nerve in a deep gluteal space.
Radiographic Changes
The mean LCEA significantly increased postoperatively relative to the preoperative assessment but partially decreased at the final follow-up. The mean Tönnis angle decreased postoperatively and partially increased at the final follow-up. The mean VCA angle also improved from the preoperative assessment to the final follow-up but partially decreased at the final follow-up. All hips maintained a Tönnis grade of ≤1 at the final follow-up (Table 6). A total of 3 hips with grade 2 ICRS cartilage damage progressed from Tönnis grade 0 to 1.
Radiographic Changes From Preoperative Assessment to Final Follow-up a

a Data are shown as mean ± SD unless otherwise noted. Bolded P values indicate statistically significant difference among the 3 time periods (P ≤ .05).
b The mean radiographic parameters among the 3 periods were tested by the Friedman test. The Tönnis grade was compared by chi-square test.
Postoperative radiographs (AP and false-profile views) showed improvement in the LCEA and the VCA angle (Figure 5, A and B). Radiographs at 1 year after surgery showed that the shelf graft was inserted anterosuperior to the hip joint (Figure 5C).

Pelvic anteroposterior (top) and false-profile (bottom) radiographs of a single patient over time. (A) Preoperative radiographs show a shallow acetabulum with a vertical-center-anterior (VCA) angle of 14° and lateral center-edge angle (LCEA) of 16°. (B) Immediately after surgery. (C) Radiographs 18 months postoperatively show a VCA angle of 30° and an LCEA of 35°.
Discussion
The main findings of this study were as follows: (1) The PRO scores of those patients who returned to artistic activities significantly improved from preoperatively to the final follow-up after surgery. (2) Overall, 89% of the artistic athletes with acetabular dysplasia were able to return to their activities after ESA combined with labral repair, cam osteoplasty, and capsular plication. (3) Finally, 3 artistic athletes could not return to their activities as the result of postoperative DGS with no improvement in PRO scores.
Several studies have assessed the rate of return to artistic activity and clinical outcomes after hip arthroscopic surgery. Kocher et al 10 described a series of 30 patients undergoing hip arthroscopic labral debridement and noted significant improvements in the mHHS and decreases in the pain score after surgery. However, only 73% (22 patients) returned to dance. Labral debridement, which is no longer recommended, was used. Nwachukwu et al 16 showed that the rates of accomplishing clinical success at 5 years after arthroscopic labral repair, capsular closure, and cam osteoplasty for FAI were not significantly different between patients with borderline hip dysplasia and those with normal coverage of the acetabulum. In a series of 24 patients with borderline hip dysplasia undergoing hip arthroscopic labral preservation, capsular plication, and cam osteoplasty, Domb et al 3 reported significant improvement in PRO scores, and 81% of patients had no requirement for revision surgery at a minimum of 5 years postoperatively. Ukwuani et al 26 showed that 97% of self-identified dancers with FAI were able to return to dance after hip arthroscopic FAI correction and labral repair. In that study, all patients underwent cam osteoplasty because arthroscopic findings confirmed dynamic impingement caused by cam lesions. However, these studies did not include dancers with acetabular dysplasia. In contrast to the high rates of successful clinical outcomes after hip arthroscopic surgery for borderline hip dysplasia, several studies have reported risk factors for failure. In a previous study, 7 we reported results in 45 hips with symptomatic borderline hip dysplasia and found that predictors for poor clinical outcomes were age >42 years, OA, a broken Shenton line, a VCA angle <17°, and a Tönnis angle >15°. From this evidence, our indications for ESA for borderline hip dysplasia are a VCA angle <17° and a Tönnis angle >15°. OA or severe chondral damage are still not indications for ESA.
Some studies have reported the rate of return to competitive sports in active patients with acetabular dysplasia undergoing periacetabular osteotomy (PAO). In a series of 41 patients undergoing PAO, Heyworth et al 8 reported that 80% of patients returned to sports. Those investigators found that the University of California, Los Angeles (UCLA) activity scores were maintained, with a mean UCLA score of 8 points. In a series of 58 patients undergoing PAO, Okoroafor et al 17 demonstrated that 67% returned to play at the preoperative level or higher after PAO. In the largest series of patients who underwent PAO (n = 161), Hara et al 5 reported that the rate of participation in sports increased from 31.1% preoperatively to 55.3% postoperatively. Those investigators also revealed that participation in sports was not associated with the progression of OA after PAO. Our findings suggest a higher rate of return to artistic activities (87%) than that reported in other studies, with 80.0% of the patients achieving PASS on the HOS--Sports after ESA.
In our study, 3 dancers (13%) experienced postoperative DGS, defined as a nondiscogenic sciatic nerve with entrapment in the deep gluteal space. 9 The diagnosis of DGS was based on a detailed clinical history, including a description of the current condition, date of onset, mechanism of injury (traumatic or nontraumatic), factors that increased or decreased pain, prior consultations, prior surgical interventions, pain level, and narcotics use. A recent study 23 in a series of 1167 patients undergoing hip arthroscopy reported that the incidence of postoperative DGS was 0.9%, and predictors for postoperative DGS after hip arthroscopic surgery were female sex, generalized joint laxity, multiple hip surgical procedures, and acetabular dysplasia. This rate is obviously higher than the traditional rates reported in the literature. In the current study, we did not measure the time of traction in all patients. We believe the traction time and the amount of traction to be the same as those in patients with FAI. ESA may cause more postoperative bleeding than FAI surgery. Blood can expand into the deep gluteal space, prompting adhesions to surrounding nerves in the deep gluteal space. We believe this procedure may carry a risk of DGS. In agreement with previous findings, all of our patients were female, and 22 of 28 patients were defined as having generalized joint laxity (Beighton score >5). These findings suggest that caution is warranted in artistic athletes with acetabular dysplasia. 23
The clinical significance of this study is that it provides evidence-based support for the addition of a minimally invasive alternative to open acetabular reorientation osteotomy for not only sedentary but also athletic patients with symptomatic mild to moderate dysplasia. Most orthopaedic practitioners perform either shelf acetabuloplasty or PAO; we specified indications for acetabular dysplasia. In our practice, patients with acetabular dysplasia with an LCEA approximately between 10° and 20°, with predictably good outcomes from hip arthroscopy alone, may still be candidates for ESA to add bony support. This is in addition to the benefits of concurrent hip arthroscopy to treat coexistent intracapsular pathologies. Nevertheless, we believe that severe acetabular dysplasia, with an LCEA of <10°, is an indication for PAO.
In this study, the mean LCEA significantly increased postoperatively relative to the preoperative assessment but partially decreased at the final follow-up. Bone resorption of shelf grafts has been known to occur occasionally. This has been attributed to the lack of sufficient pressure against the underlying femoral head and interposed capsular ligament. 22 It may be judicious to use an appropriately sized bone graft to enable sufficient anterolateral coverage. 22
This study has several limitations. This was a retrospective, short-term case series in only female patients, without a control group and involving a single surgeon. A comparative study with a larger number of patients of both sexes is needed to confirm our findings. The VCA angle was measured; however, given the variance in pelvic positioning on false-profile views, it was difficult to precisely measure the VCA angle. Some studies have shown that the VCA angle is not reliable for accurately determining the anterior coverage of the acetabulum. 25 Another limitation was the lack of a strict definition of “athlete,” which was an inclusion criterion. We did not compare artistic sports activity with other kinds of sports activity because the clinical outcomes appeared to be similar. Although the HOS—Sports was used as a measure of sports-related activity, a limitation was the absence of data on the frequency and duration of resumed athletic endeavors. In addition, the included hips underwent treatment with different capsular management strategies, because we were in the process of developing the surgical techniques for capsular plication. This could have had a substantial effect on the clinical outcomes, reproducibility, and generalizability of our findings. Cam osteoplasty, capsular treatments, and labral repair may have helped in part of the shelf procedure. Thus, it is unknown how much of the improvement was due to ESA versus the other procedures.
Conclusion
In the current study, artistic athletes were able to return to their activities with a high success rate after ESA concomitant with labral repair, cam osteoplasty, and capsular plication to treat hip dysplasia for joint laxity.
Footnotes
Acknowledgment
Final revision submitted July 7, 2021; accepted July 19, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.U. has received research support from Smith & Nephew and consulting fees from Smith & Nephew and ConMed. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Occupational and Environmental Health, Kitakyushu, Japan (No. H28-095).