
Abstract
Background:
Understanding specific risk profiles for each patient and their propensity to experience clinically meaningful improvement after anterior cruciate ligament reconstruction (ACLR) is important for preoperative patient counseling and management of expectations.
Purpose:
To develop machine learning algorithms to predict achievement of the minimal clinically important difference (MCID) on the International Knee Documentation Committee (IKDC) score at a minimum 2-year follow-up after ACLR.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
An ACLR registry of patients from 27 fellowship-trained sports medicine surgeons at a large academic institution was retrospectively analyzed. Thirty-six variables were tested for predictive value. The study population was randomly partitioned into training and independent testing sets using a 70:30 split. Six machine learning algorithms (stochastic gradient boosting, random forest, neural network, support vector machine, adaptive gradient boosting, and elastic-net penalized logistic regression [ENPLR]) were trained using 10-fold cross-validation 3 times and internally validated on the independent set of patients. Algorithm performance was assessed using discrimination, calibration, Brier score, and decision-curve analysis.
Results:
A total of 442 patients, of whom 39 (8.8%) did not achieve the MCID, were included. The 5 most predictive features of achieving the MCID were body mass index ≤27.4, grade 0 medial collateral ligament examination (compared with other grades), intratunnel femoral tunnel fixation (compared with suspensory), no history of previous contralateral knee surgery, and achieving full knee extension preoperatively. The ENPLR algorithm had the best relative performance (C-statistic, 0.82; calibration intercept, 0.10; calibration slope, 1.15; Brier score, 0.068), demonstrating excellent predictive ability in the study’s data set.
Conclusion:
Machine learning, specifically the ENPLR algorithm, demonstrated good performance for predicting a patient’s propensity to achieve the MCID for the IKDC score after ACLR based on preoperative and intraoperative factors. The femoral tunnel fixation method was the only significant intraoperative variable. Range of motion and medial collateral ligament integrity were found to be important physical examination parameters. Increased body mass index and prior contralateral surgery were also significantly predictive of outcome.
Keywords
Implementing value-based health care and shared decision-making models within orthopaedic surgery has challenged clinicians and policy makers to determine which metrics should be considered in determining patient-defined success. Patient-reported outcome measures (PROMs) are subjective metrics that are useful for evaluating a patient’s perceived state of health and function before and after treatment. Psychometric transformations of PROMs, such as defining a minimal clinically important difference (MCID), enhance their value by overcoming the challenge of interpreting raw numeric values and by allowing providers to understand what magnitude of outcome change is perceivable and important to the patient. Not achieving a clinically meaningful improvement may increase the risk of diminished patient satisfaction and suboptimal outcome. Therefore, it is imperative to gain a better understanding of which patients may not experience this level of improvement postoperatively, especially for common sports medicine procedures where many patients have high preoperative expectations and functional demands.
Many orthopaedic sports medicine subspecialties concerning procedures such as hip arthroscopy and cartilage preservation of the knee have endeavored to determine which patient-specific factors are predictive of clinically meaningful outcome improvement. Various factors such as age at the time of surgery, sex, body mass index (BMI), preoperative outcome scores, and prior surgery have been shown to be associated with outcome. 2,6,25,31 However, a major limitation to these studies is that they provide associations on a global scale and may not accurately represent individual patient risk. This is especially true concerning outcomes after anterior cruciate ligament reconstruction (ACLR), where there is a paucity of literature exploring patient-specific risk and clinically meaningful outcome improvement. Indeed, the International Knee Documentation Committee (IKDC) Subjective Knee Evaluation Form is one such PROM frequently used to assess outcomes after ACLR; however, risk factors for not achieving clinically meaningful outcome improvement for the IKDC Subjective Knee Form are not well defined at the global or patient-specific levels.
Machine learning is a subset of artificial intelligence and differs from basic statistical modeling in that the methodology prioritizes making repeatable and accurate predictions over providing interpretability. 3 The application of machine learning has gained recent interest given its robust methods for feature selection and outcome classification, thereby allowing clinicians to better understand risk for events such as complications. Furthermore, machine learning has demonstrated validity in predicting clinically meaningful outcome improvement after common orthopaedic procedures. 15 –17,23 This allows for risk prediction at the individual patient level, overcoming the limitations of current sports medicine literature. The purpose of the current study was to develop machine learning algorithms to predict achievement of the MCID on the IKDC score at a minimum 2-year follow-up after ACLR. The authors hypothesized that the best-performing machine learning model would have excellent discriminatory performance (area under the curve, ≥0.9) for predicting the MCID.
Methods
Guidelines
The Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD) guidelines and the Guidelines for Developing and Reporting Machine Learning Models in Biomedical Research were followed for this analysis. 7,21 The TRIPOD guidelines represent a systematic checklist of reporting recommendations to which researchers should adhere when performing predictive modeling and machine learning analyses to optimize reporting clarity and the potential for methodological reproducibility.
Study Population
Institutional review board approval was obtained before performing the query and analysis. Patients were identified from the ACL registry of a large academic tertiary care center that comprises 2111 patients from 27 fellowship-trained sports medicine surgeons. Included patients underwent primary ACLR between 2011 and 2013. Exclusion criteria consisted of (1) revision ACLR cases, (2) missing preoperative (after injury but before surgery) IKDC outcome data, and (3) <2-year follow-up data for the IKDC subjective form. Of the initial 2111 patients, 281 (13.3%) were excluded for undergoing revision ACLR. The final cohort of patients was obtained based on exclusion of patients who did not provide 2-year outcome responses. Analysis of baseline characteristics indicated that these patients did not significantly differ based on age (P = .16), BMI (P = .85), or sex (P = .15).
Primary Outcome
The primary outcome of interest was the MCID for the IKDC score at a minimum of 2 years postoperatively. The IKDC survey was administered electronically via the Outcomes Based Electronic Research Database platform both preoperatively and at a minimum of 2 years postoperatively. The MCID was calculated using a distribution-based method where the threshold was equal to one-half the standard deviation of the mean change in IKDC outcome scores between 2-year postoperative and preoperative time points. 8 The MCID threshold was determined to be a change of 9.2 points for our specific population.
Covariate Prediction Features and Management of Missing Data
Thirty-six preoperative and intraoperative features routinely collected in the ACL registry were tested for predictive value (Appendix Table A1). All physical examination maneuvers, including the Lachman test, were performed manually. Exploration of the registry revealed that data were missing at random, and therefore multiple imputation was appropriate. No covariates exceeded >30% missing data; therefore, all 36 features were eligible as potential predictors. 18,26 We accounted for missing data using the predictive mean matching method of multiple imputation, 9,19 thereby demonstrating the ability of the machine learning algorithms to address random “missingness” within the registry.
Algorithm Development
Recursive feature elimination with random forest algorithms 12 was applied to determine the covariate features with the highest predictive value (importance). Recursive feature elimination utilizes backward selection by creating a model with all covariates, assigning each variable an importance score and then removing features with the lowest importance scores. After this elimination step, another unique model is built, and the process is repeated until a subset of features that optimizes model performance is selected. These specific variables are used to train the machine learning algorithms.
Algorithm Performance Assessment
The study population of patients was randomly partitioned into training and independent testing (hold-out) sets using a 70:30 split (Figure 1). Six machine learning algorithms (stochastic gradient boosting, random forest, neural network, support vector machine, adaptive gradient boosting, and elastic-net penalized logistic regression [ENPLR]) were trained using 10-fold cross-validation 3 times. Each algorithm uses a different method of optimizing prediction on the training data set based on differences parametricity, assumptions, and methods of “learning.” Algorithm performance was then evaluated on an independent testing set of patients (remaining 30%), allowing for internal validation. To determine which model has optimal performance, 4 methods were used to assess each algorithm: (1) discrimination, 29,30 (2) calibration, 29,30 (3) Brier score, 4,14 and (4) decision-curve analysis 29 (Appendix Table A2).

Machine learning algorithm development methodology. ACL, anterior cruciate ligament; MCID, minimal clinically important difference.
Algorithm Fidelity Assessment
Global variable importance plots and local (patient-specific) interpretable model-agnostic explanations (LIME) were used to assess model fidelity. LIME is a quantitative visualization technique that provides insight into the decision-making process of complex “black box” machine learning models. 27 Briefly, LIME trains interpretable models to provide numeric and visual representations of the decision the model used to predict the outcome (Appendix Table A2). The best-performing machine learning model (defined as the model with the best discriminatory capability and calibration that had a Brier score less than that of the null Brier score) was subsequently transformed into an open-access application accessible on desktops and smartphones.
Results
Study Population
A total of 442 eligible patients were identified. The median age and BMI were 29.0 years (interquartile range [IQR], 21.0-40.3 years) and 24.2 (IQR, 21.9-26.6), respectively. A total of 231 (52.3%) patients were male. The complete list of preoperative and intraoperative features for the study cohort that were tested for predictive value are listed in Appendix Table A1. The prevalence of patients who achieved the MCID for the IKDC score at a minimum of 2 years postoperatively was 91.2%.
Feature Selection
A combination of the following 8 features optimized algorithm performance: age, BMI, preoperative IKDC score, preoperative Lysholm score, medial collateral ligament (MCL) examination from extension to 30° (grades 0-3), femoral tunnel fixation (intratunnel or suspensory), history of contralateral knee surgery, and preoperative degree of knee extension (recurvatum, neutral, or extension loss). This model did not identify ACL graft type as a feature that optimized algorithm performance.
To determine the relative contribution of the features to the overall predictions, we created and explored a total of 50 unique cases of LIME with 5000 permutations. Subsequently, preoperative IKDC score >62.1, preoperative Lysholm score between 50 and 64, and BMI >27.4 were associated with not achieving the MCID. Furthermore, use of suspensory femoral fixation, MCL examination grades 2 to 4, previous contralateral knee surgery, knee extension loss or recurvatum, and age >40 or <21 years were consistently feature categories associated with not achieving the MCID.
Relative Algorithm Performance
Performance characteristics of the 6 algorithms are displayed in Table 1. The best-performing algorithm based off of these metrics was the ENPLR model. This model indicated that the 5 most important features for predicting the MCID for the IKDC score were (1) a history of contralateral knee surgery, (2) preoperative knee extension, (3) MCL examination from extension to 30°, (4) method of femoral fixation, and (5) BMI (Figure 2A). This model had a C-statistic of 0.82 (Figure 2B), calibration intercept of 0.10, calibration slope of 1.15 (Figure 3), and Brier score of 0.068. The null model Brier score was 0.077, indicating that this algorithm calibrated predictions appropriately. Decision-curve analysis demonstrated that changes in management based off of the ENPLR model confer the greatest net benefit for optimizing whether a patient would achieve the MCID (Figure 4).
Algorithm Performance in Independent Testing Set (n = 131) a

a Data in parentheses are 95% CIs.
b Null model Brier score = 0.077.

(A) Global variable importance plot and (B) discrimination performance from the elastic-net penalized logistic regression model on the independent testing set. Each predictive weight of each variable is compared among the other 7 variables chosen from recursive feature elimination. The global variable importance plot represents the predictive value of each variable in descending order, with variables having lower predictive value as one moves down the y-axis. This plot indicates that a history of contralateral knee surgery is the most important predictor of achieving the minimal clinically important difference, whereas the importance of the preoperative Lysholm score is negligible. bmi, body mass index; contknee, history of contralateral knee surgery; ext, preoperative knee extension; femfix, femoral tunnel fixation method; FPR, false-positive rate; IKDC, International Knee Documentation Committee; mclexext, medial collateral ligament examination from extension to 30°; ROC, receiver operating characteristic; TPR, true-positive rate.
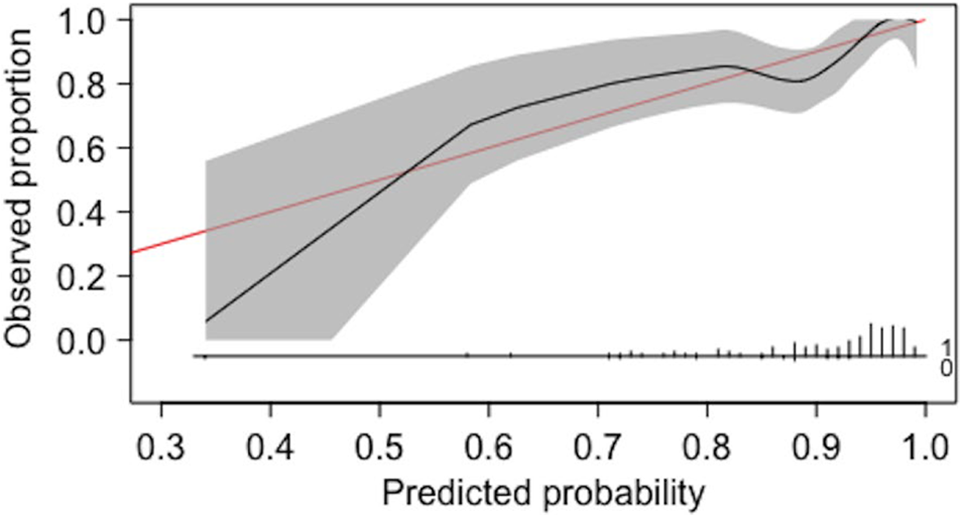
Calibration plot for the elastic net penalized logistic regression (ENPLR) model on the independent testing set of patients. The y-axis displays the true observed proportion of those who achieved the minimal clinically important difference, while the x-axis displays the corresponding predictions made by the ENPLR model. The shaded area indicates the 95% CI of the predicted probabilities. The red line represents perfect prediction.

Decision-curve analysis for the elastic-net penalized logistic regression (ENPLR) model on the independent testing set of patients. The y-axis shows the standardized net benefit of changing management based off of the model (ENPLR), the best-performing variable (BPV; history of contralateral knee surgery), for all patients, and for no patients. The x-axis demonstrates risk thresholds for not achieving the minimal clinically important difference (MCID) as a percentage, as well as the cost to benefit ratio (ratio of false-positive outcomes to true-positive outcomes). (A) View of decision-curve for wide range of risk thresholds. (B) View of decision curves for higher-risk thresholds. When risk is very high (80% likelihood of not achieving MCID), management changes based off of the ENPLR model give greater net benefit (higher likelihood of achieving the MCID) than changing management based on the other decisions.
Application Development
The open-source application is available online (http://orthoapps.shinyapps.io/ACLR_IKDC). This application demonstrates how combinations of patient-specific factors can provide risk assessment on a case-by-case basis. An example of the use of this prediction application is shown in Figure 5.
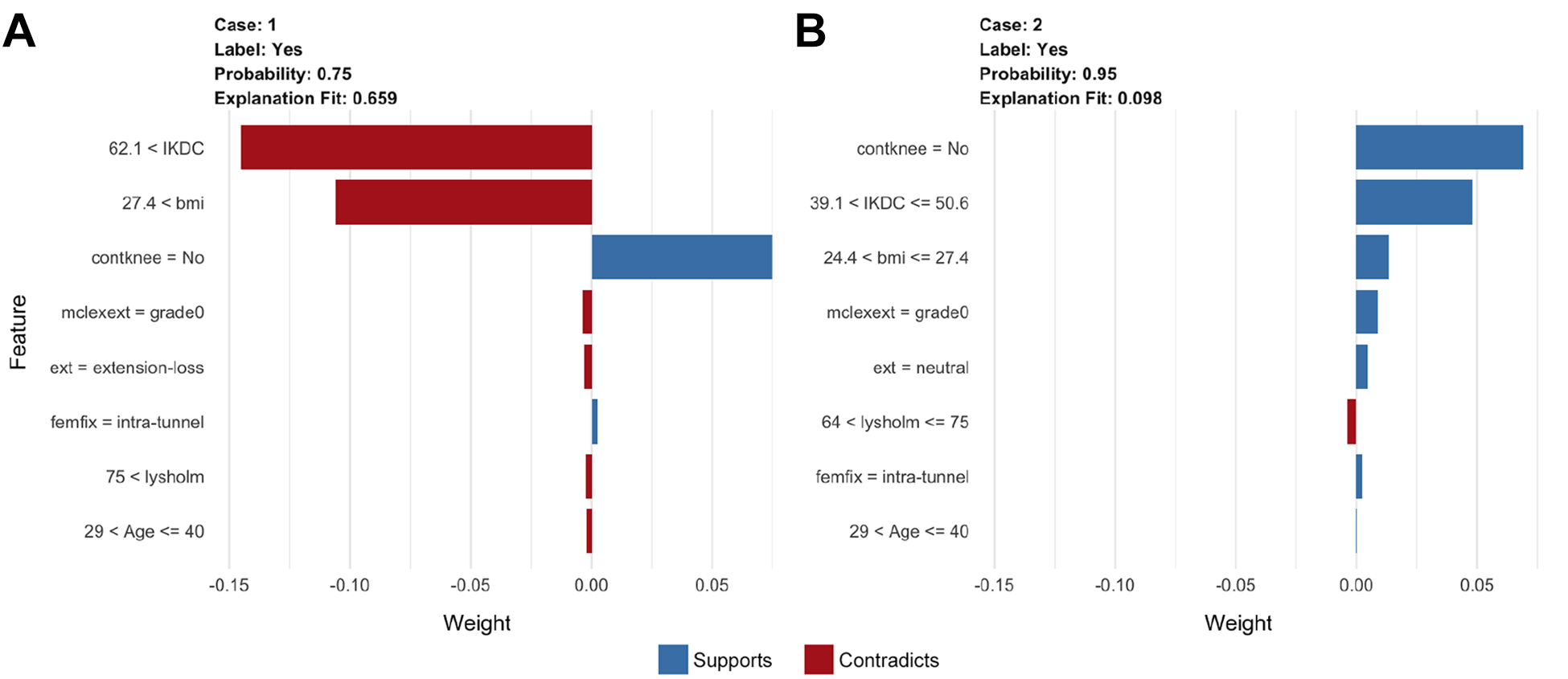
Demonstration of the clinical effect that application of the clinical decision-making tool derived from the elastic-net penalized logistic regression model can have if applied during the preoperative period. The red bars indicate features that support the probability of achieving the minimal clinically important difference (MCID), and the blue bars indicate features that put the patient at risk of not achieving the MCID. (A) Case 1: A 30-year-old patient with an anterior cruciate ligament tear and body mass index (BMI) of 31 is evaluated at the clinic. The patient has a relatively high level of function (International Knee Documentation Committee [IKDC] score, 75; Lysholm, 80). The patient has never had a contralateral knee surgery. On examination, the patient demonstrates a grade 0 medial collateral ligament examination and has an extension loss; the decision is made to operate using an intratunnel femoral fixation technique. Given this decision, at 2 years postoperatively, there is a 25% chance the patient will not achieve a clinically meaningful improvement in symptoms and function. (B) Case 2: Instead of pursuing surgery, the patient is recommended to first optimize his current health state. The patient is able to decrease BMI into the normal category (BMI, 27) and obtain neutral extension on examination via physical therapy. By using the current algorithm to optimize his health state based off of their specific risk factors, this patient improved the probability of achieving a clinically meaningful improvement in symptoms and function to 95% at 2 years postoperatively. bmi, body mass index; contknee, history of contralateral knee surgery; ext, preoperative knee extension; femfix, femoral tunnel fixation method; mclexext, medial collateral ligament examination from extension to 30°.
Discussion
The main findings of the current study are (1) 6 machine learning algorithms were developed, with the ENPLR model demonstrating good ability to predict the MCID for the IKDC score at a minimum of 2 years postoperatively, and (2) the 5 most important features found to predict the MCID for the IKDC score were a history of contralateral knee surgery, preoperative knee extension, MCL examination grade from extension to 30°, method of femoral fixation, and BMI. These findings have important implications for preoperative patient counseling and shared decision-making strategies.
Machine learning describes statistical processes that exhibit experiential “learning” associated with human intelligence and the capacity to improve via the application and refinement of algorithms. 3 These algorithms learn to make specific decisions based off of this training and can then be modified or enhanced, allowing for the development of a model with powerful ability to transform inputs into an accurate prediction. 3 These predictions are compared against the true outcomes present in the data to determine the accuracy of the algorithms, and models can be modified again to further optimize performance. 13 The current study applied this methodology to predict clinically meaningful outcome improvement after ACLR and potentially enhance the treatment using customized risk predictions.
The 5 most important features for predicting clinically meaningful improvement after ACLR are semimodifiable. For example, in Figure 5, by undergoing a theoretical period of preoperative optimization of knee function, a patient improved the probability of experiencing clinically meaningful improvement by 20% from the previous baseline estimate. Furthermore, it is important that the selected features are clinically plausible. Through multiple permutations of LIME, the current study specifically determined the following 8 preoperative variables as consistently being predictive of not achieving the MCID: IKDC score >62.1, preoperative Lysholm score between 50 and 64, BMI >27.4, use of suspensory femoral fixation, MCL examination grades 2 to 4, previous contralateral knee surgery, knee extension loss or recurvatum, and age >40 or <21 years.
Recent studies have examined all of these factors. Indeed, the importance of the integrity of the MCL as a major restraint to anteromedial instability, 33 the knee extension deficits as a risk factor for poor outcomes and Cyclops syndrome, 10 the potential effect of femoral tunnel fixation methods when used, 32,35 and the associations between characteristic and preoperative PROMs with postoperative outcomes have all been documented. 11 Interestingly, although the method of femoral tunnel fixation demonstrated significant predictive value, graft type was not found to optimize algorithm performance in this specific cohort, while previous studies 5,34 have reported associations between graft type and functional outcomes. However, the significant relationship found with fixation may have indirectly been due to graft type. Beyond the scope of the current study, however, it is possible that graft type was not a significant predictor in this cohort given that (1) the majority of patients received autografts, and recent literature has demonstrated inconsistent findings with regard to knee laxity and failure rates among autograft types 28 ; and (2) the IKDC score specifically has been demonstrated not to statistically differ among autograft types, suggesting that it may not be sensitive to this specific factor. 1,28,34
The performance of the ENPLR machine learning model demonstrated excellent discrimination and calibration for predicting which patients will achieve the MCID for the IKDC score at a minimum of 2 years after primary ACLR. Furthermore, the relatively low Brier score of the ENPLR model indicated that the predictions were calibrated well, and decision-curve analysis suggested that patients will experience the greatest benefit from changes in management based off of this model when their risk of not achieving the MCID is high. These findings not only support the validity of the development and performance of the ENPLR model but also the clinical utility that this model confers. The ENPLR model was transformed into an open-access online application that can be used in office-based settings. This type of resource has the potential to enhance shared decision making and improve outcomes for patients undergoing primary ACLR.
A few limitations should be discussed in the context of the current study results. First, although the current study explored a very large number of potential variables, it did not study other variables that may have associations with achieving the MCID for the IKDC score. There remain certain semimodifiable features, such as graft tunnel placement, time from injury to surgery, meniscal integrity, cartilage status, chronicity of MCL laxity, and tibial slope, that have been demonstrated in recent literature 20,22,24 to be associated with outcomes after ACLR and were not routinely collected in the prospective repository used for this study.
Furthermore, in accordance with the purpose of the study and model, which is aimed at allowing for preoperative intervention, we chose features that were modifiable or semimodifiable. This may have also narrowed the potential feature pool. However, we used recursive feature elimination, a powerful statistical tool, to ensure that the variables included in the algorithm development had high predictive value. An additional limitation of the machine learning models in the current study was that they underwent internal validation on patients at a large academic medical center from 27 surgeons but still may not be generalizable to patients in other geographic locations. External validation is required to confirm the performance of these algorithms in heterogeneous populations before using this online tool for active clinical decision making. However, this tool provides value as an educational aid and demonstrates the value and power of machine learning to integrate individualized patient data to perform clinically useful predictions.
Finally, as this study was not performed prospectively, it is possible that there was heterogeneity in the physical examinations of the 27 surgeons. For example, although knee extension loss and recurvatum were highly predictive variables of not achieving a clinically important outcome, it is theoretically possible that testing specifically for hyperextension was not performed in all patients. However, testing for knee hyperextension is a routine part of the knee examination by sports medicine surgeons at our institution, and the rate of missing data was low for this variable, adding confidence to the knee extension findings and predictive performance of this variable.
Conclusion
Machine learning, specifically the ENPLR algorithm, demonstrated good performance for predicting a patient’s propensity to achieve the MCID for the IKDC score after ACLR based on preoperative and intraoperative factors. Femoral tunnel fixation method was the only significant intraoperative variable. Range of motion and MCL integrity were found to be important physical examination parameters. Increased BMI and prior contralateral surgery were also significantly predictive of outcome.
Footnotes
Authors
Kyle N. Kunze, MD (Department of Orthopedic Surgery, Hospital for Special Surgery, New York, New York, USA); Evan M. Polce, BS (University of Wisconsin School of Medicine and Public Health, Madison, Wisconsin, USA); Anil S. Ranawat, MD; Per-Henrik Randsborg, MD, PhD; Riley J. Williams III, MD; Answorth A. Allen, MD; Benedict U. Nwachukwu, MD, MBA (Department of Orthopedic Surgery, Hospital for Special Surgery, New York, New York, USA); HSS ACL Registry Group (Andrew Pearle, MD; Beth S. Stein, MD; David Dines, MD; Anne Kelly, MD; Bryan Kelly, MD; Howard Rose, MD; Michael Maynard, MD; Sabrina Strickland, MD; Struan Coleman, MD; Jo Hannafin, MD, PhD; John MacGillivray, MD; Robert Marx, MD; Russell Warren, MD; Scott Rodeo, MD; Stephen Fealy, MD; Stephen O’Brien, MD; Thomas Wickiewicz, MD; Joshua S. Dines, MD; Frank Cordasco, MD, MS; and David Altcheck, MD [Department of Orthopedic Surgery, Hospital for Special Surgery, New York, New York, USA]).
Final revision submitted May 7, 2021; accepted June 23, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.S.R. has received research support from DePuy and Stryker; consulting fees from Ceramtec, Medtronic, Moximed, Smith & Nephew, and Stryker; speaking fees from Ceramtec, Medtronic, Smith & Nephew, and Stryker Mako; and royalties from DePuy, Saunders/Mosby–Elsevier, Springer, and Stryker Mako and has stock/stock options in ConforMIS and Enhatch. R.J.W. has received research support from Histogenics; consulting fees from Arthrex, JRF Ortho, and Lipogems; royalties from Arthrex; hospitality payments from Stryker and has stock/stock options in BICMD, Cymedica, Engage Surgical, Gramercy Extremity Orthopedics, Pristine Surgical, and RecoverX. A.A.A. has received consulting fees from Arthrex and has stock/stock options in Pristine Surgical and Rom3. B.U.N. has received royalties from Remote Health. D.D. has received consulting fees and royalties from Zimmer Biomet. A.K. has received education payments from Arthrex. B.K. has received consulting and nonconsulting fees and royalties from Arthrex and speaking fees from Synthes GmbH. M.M. has received education payments from Arthrex. S.S. has received consulting fees from DePuy, Flexion Therapeutics, Pfizer, and Vericel and honoraria from JRF Ortho and Vericel. S.C. has received education payments from Pinnacle, consulting fees from Stryker, and nonconsulting fees from Smith & Nephew. J.H. has received hospitality payments from Smith & Nephew. R.W. has received royalties from Zimmer Biomet and nonconsulting fees from Arthrex. S.R. has received consulting fees from Flexion Therapeutics, nonconsulting fees from Smith & Nephew, honoraria from Fidia Pharma, and royalties from Zimmer Biomet and is a paid associate editor for The American Journal of Sports Medicine. S.F. has received royalties from Encore Medical. J.S.D. has received consulting fees from Arthrex, Merck Sharp & Dohme, Trice Medical, and Wright Medical; speaking fees from Arthrex; and royalties from Linvatec. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Hospital for Special Surgery (study No. 2016-908).
APPENDIX
Performance Metric Interpretation Guide a

| Metric | Description |
|---|---|
| Discrimination | Assessed through performing ROC analyses and quantifying the AUC (also referred to as the concordance statistic [C-statistic]). The C-statistic is described as the probability that the machine learning model will assign a greater predicted probability to a randomly selected positive case (patient who achieved the MCID) relative to a randomly selected negative case (false-positive case, ie, a patient who did not achieve the MCID). |
| Calibration | Assesses the agreement between predictions made by the machine learning models and the true observed outcomes. A calibration slope of 1 and calibration intercept of 0 are indicative of perfect prediction by the model. Performance is assessed through quantifying the calibration slope (precision of predictions) and calibration intercept (tendency for model to overestimate or underestimate the observed outcome). |
| Brier score | A proper scoring function that assesses overall performance and is an extension of calibration and discrimination. The Brier score for each model is equal to the mean squared difference between the true observed outcomes and the model prediction probabilities as a benchmark to quantitatively ensure that the machine learning models are providing valuable predictions and not demonstrating class imbalance; the null model Brier score (Brier score where the predicted probabilities of the null model are equal to the outcome prevalence of the entire study cohort) is calculated. The Brier score of each machine learning model is subsequently compared with this value. In general, lower Brier scores indicate that predictions are better calibrated (with zero being perfect performance and calibration), and Brier scores lower than the null model score indicate model usefulness. |
| Decision-curve analysis | An analysis that provides insight into potential clinical utility of making changes in patient management based off of the machine learning model and alternative scenarios by comparing the predicted net benefit of using the model at varying risk thresholds. Decision-curve analysis specifically compares changes in management based off of the model, the best-performing predictive variable alone, changes for all patients, and changes for no patients. As the risk threshold probability increases, the cost to benefit ratio (and consequently the weight attributed to false-positive classifications made by the model) increases. |
| Local interpretable model-agnostic explanations | LIME samples local input variable distributions using a predefined number of permutations and assesses the effect of specific ranges of values for each predictor feature on the primary outcome. The importance of each feature is computed and carried forward based on similarities between the features and the model predictions. LIME then explains model fit (here, how well this local example represents both the global model behavior and its plausibility) and provides a visual explanation of how each feature contributes to the overall predictions, demonstrating how each variable on a case-by-case basis either supports (increases the probability of achieving the MCID) or contradicts (decreases the probability of achieving the MCID) the prediction. A ridge regression model with the Gower distance function and a kernel width of 1.25 was used to optimize LIME in the current study. |
a AUC, area under the curve; LIME, local interpretable model-agnostic explanations; MCID, minimal clinically important difference; ROC, receiver operating characteristic.