
Abstract
Background:
To investigate the effect of ulnar collateral ligament stretching due to the "creep phenomenon," the effect of accumulating elbow valgus stress on ligaments must be clarified.
Purpose:
To evaluate the effect of continuous elbow valgus stress on the medial elbow joint space (JS).
Study Design:
Controlled laboratory study.
Methods:
The authors measured the JS of the nondominant elbow joints of 20 healthy male university students (age, 21.4 ± 0.5 years; height, 171.4 ± 6.5 cm; weight, 65.7 ± 9.1 kg). The participants were seated with their shoulder at 90° of abduction and external rotation and their elbow at 30° of flexion, and elbow valgus stress was maintained at loads of 30 and 60 N using a Telos stress device. The JS was measured on ultrasound images of the medial elbow joint with the elbow in the start limb position (0 N) and then immediately (0 seconds) and at 60, 120, 180, 240, and 300 seconds after loading. In addition, muscle activity of the pronator teres muscle during JS measurement was monitored to examine the presence or absence of defensive contraction due to pain. Analysis of variance and the Bonferroni method for post hoc testing were used for statistical analysis.
Results:
No participants showed defensive contractions of the pronator teres. At 30 N, JS was significantly larger 60 seconds after loading compared with immediately after loading (P = .007). At 60 N, JS was significantly larger after 120 seconds, as the loading time of valgus stress increased, compared with immediately after loading (P = .002).
Conclusion:
JS was significantly larger immediately after loading of valgus stress, with an increase in continuous elbow valgus stress after 60 seconds at 30 N and after 120 seconds at 60 N. These results suggest that a creep phenomenon may develop around the soft tissue of the elbow when loaded by a continuous valgus stress.
Clinical Relevance:
JS is significantly increased by continuous elbow valgus stress.
Ulnar collateral ligament (UCL) injury is a common sports injury among overhead athletes 21 and is thought to be caused by repeated elbow valgus stress. 11 The UCL is considered to represent the primary ligamentous stabilizer for elbow valgus stress. 15 At the time of pitching, elbow valgus stress of up to about 64 N·m is applied to the elbow. 7 However, the maximum strength of the UCL has been reported to be about 34 N·m. 2 That is, elbow valgus stress at the time of pitching seems to exceed the braking strength of the UCL. The elbow valgus braking function of the flexor muscles of the forearm is thus considered very important. 4,6,8,9,13,18,19,22,23
The medial elbow joint space (JS) is used as an index to quantitatively evaluate the elbow valgus braking function. 3,16 JS measurements have also been reported as useful in assessing UCL flaccidity and damage. 3,19 Hattori et al 10 had high school baseball players make a total of 100 pitches and measured the JS every 20 pitches. They reported that JS was significantly increased after 60 pitches compared with before pitching. In addition, Millard et al 14 performed repeated wrist flexion exercises in healthy adults and measured the maximum wrist flexion muscle strength and JS under gravity stress on the forearm before and after exercise. They reported that the maximum muscle strength of the wrist joint decreased significantly and JS increased significantly; the cause of the increased JS was considered to be muscle fatigue. However, since muscle contraction was not performed during JS measurement, whether JS increased because of muscle fatigue remains unknown.
On the other hand, ligaments show a creep phenomenon whereby they stretch under constant load. 5 JS may thus have increased not because of muscle fatigue but rather because of UCL extension as a result of the creep phenomenon. To investigate the effect of UCL stretching due to the creep phenomenon, the effect of accumulating elbow valgus stress on the ligaments must be clarified.
Therefore, the purpose of this study was to investigate the influence of continuous elbow valgus stress on JS. We hypothesized that JS would be significantly larger immediately after loading of valgus stress compared with the starting limb position, and the JS would increase after 120 seconds at 30 and 60 N.
Methods
Study Participants
Included in this study were 20 healthy male university students (age, 21.4 ± 0.5 years; height, 171.4 ± 6.5 cm; weight, 65.7 ± 9.1 kg). The elbow joint on the nondominant hand side of the patients was used for measurements. Exclusion criteria were a history of orthopaedic disease in the elbow joint or the presence of elbow joint pain at the time of measurement. Handedness was confirmed using the Edinburgh Handedness Inventory. 17
This study was carried out with the approval of the university ethics review committee and conducted in accordance with the Declaration of Helsinki. All participants provided informed consent before enrollment.
Measurement of the Medial Elbow JS
All measurements were conducted while the participant was seated in a chair with their shoulder at 90° of abduction and external rotation and their elbow at 30° of flexion. Loading was set using a Telos stress device (Aimedic MMT) (Figure 1). An ultrasonography system (Aplio 500; Toshiba Medical Systems) and high-frequency linear probe (PLT-1204BT, 12 MHz; Toshiba Medical Systems) were used for JS measurement. With reference to a study by Ciccotti et al, 3 the probe was applied to the medial side of the elbow joint, and the anterior bundle of the UCL was visualized with the humeral trochlea and ulnar sublime tubercle as landmarks. The JS was defined as the distance from the medial distal end of the humeral trochlea to the proximal end of the ulnar sublime tubercle and measured with calipers on the ultrasonogram (Figure 2). The load was set as 30 or 60 N, which was randomly performed. Considering the effects of fatigue, measurements for each load were performed on separate days within 1 week. All measurements were made by a single physical therapist (M.E.).
The measurement protocol was to first take an ultrasound image of the medial elbow joint at the starting limb position (0 N load) within 10 seconds. After that, the load was gradually increased by 10 N/s. When the predetermined load was reached, images were taken at 0, 60, 120, 180, 240, and 300 seconds while maintaining the load (Figure 3).

Measurement position for the medial elbow joint space using the Telos stress device. The participant sat in a chair at 90° of shoulder abduction and external rotation, 90° of forearm supination, and 30° of elbow flexion.

Measurement of the medial elbow joint space using ultrasonography. (A) Measurement site at the ulnohumeral joint. (B) Long-axis image of the ulnohumeral joint. 1 = medial epicondyle; 2 = medial distal end of the humeral trochlea; 3 = proximal end of the ulnar sublime tubercle; 4 = anterior bundle of the ulnar collateral ligament. The white line demonstrates the measurement of the joint space opening.
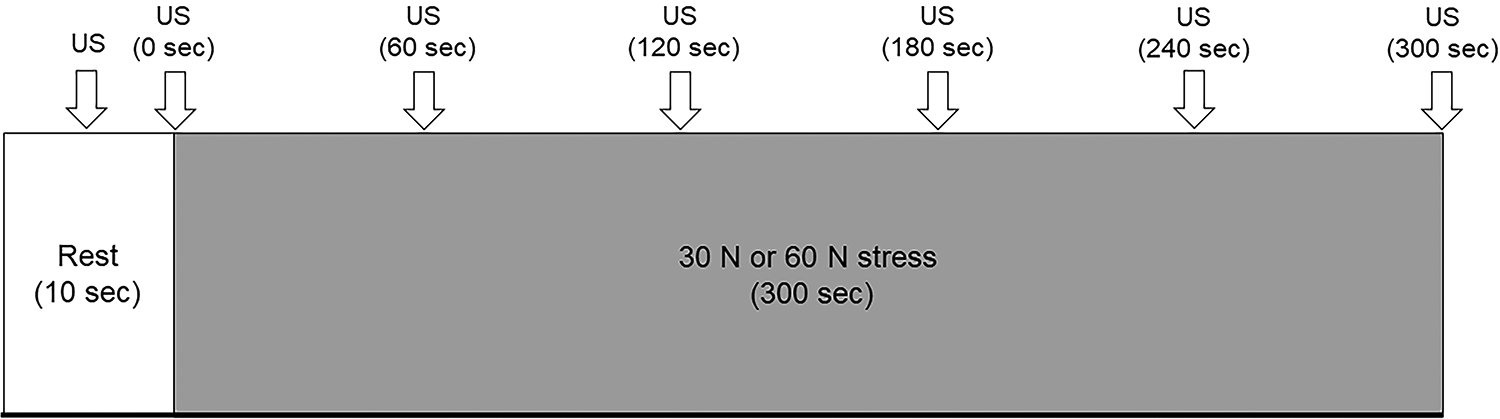
The measurement protocol. US, ultrasound.
To verify the reliability of the JS measurements, 1 month before the study experiment, nondominant elbows from 8 of the participants (age, 21.9 ± 0.8 years; height, 170.8 ± 4.2 cm; weight, 63.8 ± 4.0 kg) were examined at the starting limb position and with loads under 30 and 60 N by the same examiner using the same measurement protocol. These measurements were compared with values from the same 8 participants taken during the experiment.
Measurement of Defensive Muscle Contractions and Pain
At the same time, we measured whether valgus stress caused defensive muscle contractions or pain. Contractions were measured using an electromyogram (EMG) (DPA2078; DiaMedical System). The distance between electrodes was set to 1.0 cm, and after skin treatment with alcohol, the surface electrode (Blue Sensor; Mets) was attached to the pronator teres. The pronator teres muscle is located in the superficial layer and was adopted due to being a clearly identifiable muscle under the skin. The sampling frequency was 1000 Hz, and the derived EMG data were converted from analog to digital using Power Lab software (AD Instruments) and imported into a computer. Bandpass filtering (20-1000 Hz) was then performed using EMG analysis software (Chart7 for Windows), and full-wave rectification was performed.
Muscle contraction values were normalized as the percentage of the maximum voluntary contraction (%MVC) in the middle of the forearm during isometric forearm pronation with the elbow flexed 90°. First, maximum isometric forearm pronation was performed by manual resistance and the MVC was measured. For each load, the maximum value of full-wave rectification for 300 seconds was divided by the MVC to obtain the %MVC. With reference to a previous study by Aagaard et al, 1 ≥2.5% MVC was set as representing defensive contraction. During each measurement, the intensity of pain in the medial elbow joint was reported by the participant on a numerical rating scale (NRS) (range, 0-10 [10 set as maximum pain]). If the NRS score reached 10, the measurement was discontinued.
Statistical Analysis
Intrarater reliability was calculated with the intraclass correlation coefficient (ICC). The ICC values were interpreted according to the criteria of Landis and Koch 12 : <0.00, poor; 0.00 to 0.20, slight; 0.21 to 0.40, fair; 0.41 to 0.60, moderate; 0.61 to 0.80, substantial; and 0.81 to 1.00, almost perfect. Repeated-measures analysis of variance was used to compare the JS between 0 N and 30 or 60 N of continuous elbow valgus at the different stress times (0, 60, 120, 180, 240, and 300 seconds) using the Bonferroni method for post hoc testing. The level of significance was set at 5%. All statistical analyses were performed using SPSS (version 26.0; SPSS Japan).
Results
The ICC(1,1) values of the JS measurements were 0.973 at the start limb position, 0.965 at 30 N, and 0.946 at 60 N, indicating near perfect reliability. No participant showed defensive contractions (muscle contraction, ≥2.5% MVC) of the pronator teres at any time point.
Table 1 shows the JS for each load at each valgus stress time. At both 30 and 60 N, the JS was significantly larger at all loaded times compared with the start limb position (0 N). In addition, at both loads, the JS was significantly larger at 60, 120, 180, 240, and 300 seconds compared with immediately after loading of valgus stress (0 seconds). The JS continued to increase significantly with longer elbow valgus stress times after 60 seconds at 30 N and after 120 seconds at 60 N.
Medial Elbow Joint Space at Each Valgus Stress Load and Time (N = 20 Elbows). a

a Data are presented as mean ± SD. s, seconds.
Statistically significant differences at 30 N:
bP < .001 versus start limb position (0 N).
cP = .007 versus 0 seconds.
dP = .011 versus 60 seconds.
eP = .001 versus 60 seconds.
fP = .042 versus 120 seconds.
gP = .001 versus 120 seconds.
hP = .003 versus 180 seconds.
Statistically significant differences at 60 N:
iP < .001 versus start limb position (0 N).
jP = .002 versus 0 seconds.
kP = .001 versus 60 seconds.
lP = .003 versus 120 seconds.
mP = .033 versus 180 seconds.
nP < .001 versus 180 seconds.
oP = .044 versus 240 seconds.
Discussion
In this study, the JS was significantly larger than immediately after loading of valgus stress, with an increase in continuous elbow valgus stress after 60 seconds at 30 N and after 120 seconds at 60 N. In addition, no participants showed defensive contractions during any measurement.
The UCL and forearm flexor muscles are examples of soft tissues located on the medial side of the elbow and involved in elbow valgus braking. ‡ As the UCL is considered to be the main stabilizer under 30° of elbow flexion, 15 we measured the JS at 30° of elbow flexion. The UCL was thus considered to be particularly loaded among the soft tissues inside the elbow. In addition, the ligament shows a creep phenomenon of stretch under constant load. It has been established that continuous creep is caused by continuous load and periodic creep is caused by repetitive load. 5 In this study, defensive contractions did not occur and JS increased because of continuous elbow valgus stress, suggesting that continuous creep may have increased JS.
We applied elbow valgus stress continuously at 2 different loads. However, UCL injury is thought to be caused by repeated elbow valgus stress. 11 Therefore, changes in JS with repetitive elbow valgus stress need to be examined in the future. In addition, previous studies have reported that contraction of the forearm flexor muscles reduces JS. 18,20 Future studies will need to investigate whether contraction of the forearm flexor muscle group can suppress increases in JS caused by continuous elbow valgus stress, as well as clarify the effects of fatigue tasks on the forearm flexor muscle group.
This study has some limitations. First, the JS measurement was not performed at times shorter than 60 seconds. At 30 N, creep may have occurred before 60 seconds. Second, we could not continue measurements for more than 300 seconds. The creep phenomenon after a long period of time is unknown. In the future, the time may need to be divided into smaller intervals for consideration. Third, this study targeted the elbow joint on the nondominant side among healthy male university students. Last, the JS was measured instead of the length of the ligament. In the future, investigations of the pitching side and in elbows with UCL injury should be conducted.
Conclusion
This study examined the effect of continuous elbow valgus stress on JS in healthy male college students. The JS was significantly larger immediately after the loading of valgus stress, with an increase in continuous elbow valgus stress after 60 seconds at 30 N and after 120 seconds at 60 N. These results suggest that a creep phenomenon may develop in the soft tissues around the elbow when loaded by a continuous valgus stress.
Footnotes
Final revision submitted April 14, 2021; accepted June 8, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by a Grant-in-Aid for Scientific Research (19K11358) from the Japanese Society for the Promotion of Science (JSPS) and was commissioned by the Japan Sports Agency (Female Athletes Development and Support Projects 2020). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Niigata University of Health and Welfare (study No. 18430).