
Abstract
Background:
The optimal treatment for complete avulsions of the proximal adductor longus (AL) is still debatable, and different operative and nonoperative treatment options have been suggested.
Purpose:
To report surgical techniques and functional outcomes of a series of athletes who were treated operatively for proximal AL tears.
Study Design:
Case series; Level of evidence, 4.
Methods:
A retrospective evaluation of patients who underwent surgical repair of complete proximal AL tear with concomitant distal fascial release with or without lesions of the neighboring soft tissue structures was performed. This included preinjury Tegner score, age, number of tendons involved, time interval from injury to surgery, and postoperative complications. Self-reported outcomes were defined based on the ability to regain sports activities (excellent, good, moderate, fair, or poor). Between-group comparisons were performed to identify factors associated with improved outcomes. The Mann-Whitney nonparametric test was used for comparing continuous variables, and the Fisher exact test was used for comparing nominal variables.
Results:
A total of 40 male athletes were included in the evaluation, with an average follow-up of 11 months (range, 6 months-8 years). Self-reported outcome was excellent in 23 (57.5%), good in 13 (32.5%), and moderate in 4 (10%) patients. Comparisons between patients with excellent versus good/moderate outcomes revealed nonsignificant differences regarding age at injury and preinjury Tegner score. Athletes with excellent outcomes received surgery sooner after the injury compared with athletes with good/moderate outcomes (2.4 ± 1.8 vs 11.4 ± 11.0 weeks, respectively; P < .01).
Conclusion:
Surgical repair for complete proximal AL tears with a concomitant distal fascial release resulted in outcomes rated as good or excellent in 90% of the cases. This treatment should be considered particularly in high-level athletes with a clear tendon retraction and within the first month after the injury. Further research is nevertheless needed to compare these outcomes with other treatment alternatives to better define criteria advocating surgery.
A tear of the adductor longus (AL) tendon is an uncommonly reported injury. 14 It usually affects athletes involved in cutting-pivoting sports. A recent investigation exploring the mechanism of injury to the AL in male football (soccer) players through video analysis demonstrated 4 major situations that led to AL tears. 16 These included open-chain movements such as kicking and jumping and closed-chain movements such as change of direction and reaching. The common denominator in these various situations was rapid, high-muscle activation during rapid muscle lengthening occurring throughout the hip adductors, with the hip extended and externally rotated. The investigators thus supported the promotion of eccentric training of the groin adductors in prevention programs. 16
Until recently, a treatment of choice had not been determined once an injury occurred. Nonoperative management with relative rest and physical therapy can be suggested as a first-line option but at the potential cost of developing chronic groin discomfort during sporting activities. 4,10,15 Moreover, the confluency of the aponeurotic layer overlying the adductor insertion with the lower abdominal layers involving the rectus abdominis and pyramidalis muscles and the conjoint tendon with the external oblique fascia may subject athletes sustaining proximal adductor tendon tears to the development of chronic adductor-related groin pain and athletic pubalgia. 4,5 Furthermore, a recent study that investigated magnetic resonance imaging (MRI) scans of injured athletes showed that the proximal AL was rarely injured in isolation and more frequently comprised only 1 injured structure among other lesions that involved an interconnected complex. This also includes the pyramidalis muscle, the anterior pubic ligament, the AL fibrocartilage, and, sometimes, the pectineus muscle. 13 Thus, a violation of this anatomic confluency and the possible resultant asynchronous dysfunction among these structures following eccentric groin overload through tear of the AL and adjacent structures may be responsible for the development of chronic symptoms if not addressed with early repair. This might disable the athlete and require further surgical interventions such as adductor tenotomy 1,12 or may require repair of pubic aponeurotic plate lesions. 5
Considering surgical options to treat adductor tendon tears, 3 it was shown in a limited number of patients that early repair of adductor tears with reinsertion to the pubic origin can lead to excellent outcomes, thus providing some support to suggest early surgery instead of conservative management. 11,19 Others were able to support objective improvement in adductor strength following surgical release in a case report of a chronic lesion. 6 However, there has not been a study in a large series of patients treated with operative repair and a distal fascial release that could have the potential to provide a more thorough understanding of the outcomes of such an approach and help in elaborating a treatment rationale for these injuries in athletes.
The purpose of this study was to report functional outcomes in a series of athletes treated operatively for proximal AL tendon tears. It was hypothesized that anatomic repair of AL ruptures with concomitant distal fascial release would result in return to sports in the majority of cases, without substantial postoperative morbidity.
Methods
A retrospective evaluation of patients undergoing surgical repair of complete proximal AL tendon tear between 2010 and 2018 was performed. Preoperative diagnoses were made based on history, physical examination, and MRI (Figure 1). Inclusion criteria were (1) sports-related proximal tear of the AL and (2) operative repair of the AL and neighboring soft tissue with or without adjacent tendon repair, alongside distal AL fascial layer release. Patients excluded from the series were those undergoing surgical treatment for chronic (>2 months) groin pain that involved superficial AL release without AL tendon repair. The study was performed in accordance with written rules of the local hospital ethics committee.

(A) T2-weighted short tau inversion recovery MRI coronal view of the pelvis demonstrating complete left proximal AL avulsion tear with more than a 2-cm retraction (arrows) and (B) MRI T2-weighted coronal view of the pelvis showing chronic tear of left AL after nonoperative management demonstrating partial continuity (arrows). AL, adductor longus; MRI, magnetic resonance imaging.
Clinical data were retrieved from office charts and operative reports and included sex, age at injury, type of sports, level of activity according to Tegner scale, 18 mechanism of injury, interval between injury and surgery (weeks), extent of the injury (number of adjacent tendons involved as identified during surgery), postoperative complications, and follow-up time. Self-reported outcomes were classified as excellent (patient was able to return to preinjury activity level, free of any symptoms during any activity); good (patient was able to return to preinjury activity level, with mild pain or discomfort during sports, and without symptoms during activities of daily living); moderate (patient was able to return to sports at a lower level with minor symptoms during sports such as reduced strength or deficient groin flexibility but no symptoms during activities of daily living); fair (patient did not resume sports activities because of significant pain and discomfort during such activities, alongside minor symptoms during activities of daily living); or poor (patient was unable to resume sports activities, alongside substantial difficulties in activities of daily living).
The patients in this study had surgical repair of the proximal AL tendon with a concomitant distal fascial release within 4 weeks postinjury. Tendon retraction advocating repair was defined as more than 2 cm, and the athletes also reported in these cases feeling weakness of the hip adductors, which was also noted on the physical examination. When retraction was less than 2 cm, failure of nonoperative treatment was defined as failure to return to sports, based on previously suggested guidelines after hamstring injuries, 2 and in these circumstances, proximal AL repair with a distal fascial release was suggested as well. Symptoms indicating failure of nonoperative treatment involved local dull pain with tenderness of the involved area during direct contact at sports activities, painful limitation, and excessive tightness during stretching of the groin adductors during forced contraction, or friction against the surrounding tissue with tethering sensation during sports activities. Symptoms resulted in the athlete's inability to perform sports-specific tasks and resume sports at the level desired.
Surgical Technique
Patients were positioned supine with the hip at 45° of abduction and external rotation and the knee at 90° of flexion. In acute repairs, a 3- to 5-cm transverse incision was used at the medial proximal thigh 3 cm distal to the palpable pubic tubercle, overlying the adductor mass. The common adductor fascia, when intact, was opened with a curved incision. This tissue was subsequently used as a fascia flap to reinforce the reinsertion site. The adductor rupture was identified, often with concomitant lesions of the neighboring fibrocartilage, pyramidalis muscle, and anterior pubic ligament. The torn structures were released from any adhesions, and excessive scar tissue was resected. Reinsertion of the ruptured AL tendon was performed by using 1 or 2 single- or double-loaded suture anchors (Figure 2). Initially, we used GII titanium suture anchors (DePuy Mitek), but over the years, with newly designed anchors, suture-only anchors were used regularly (ie, Iconix 2.3 mm [Stryker] or JuggerKnot [Zimmer Biomet]).
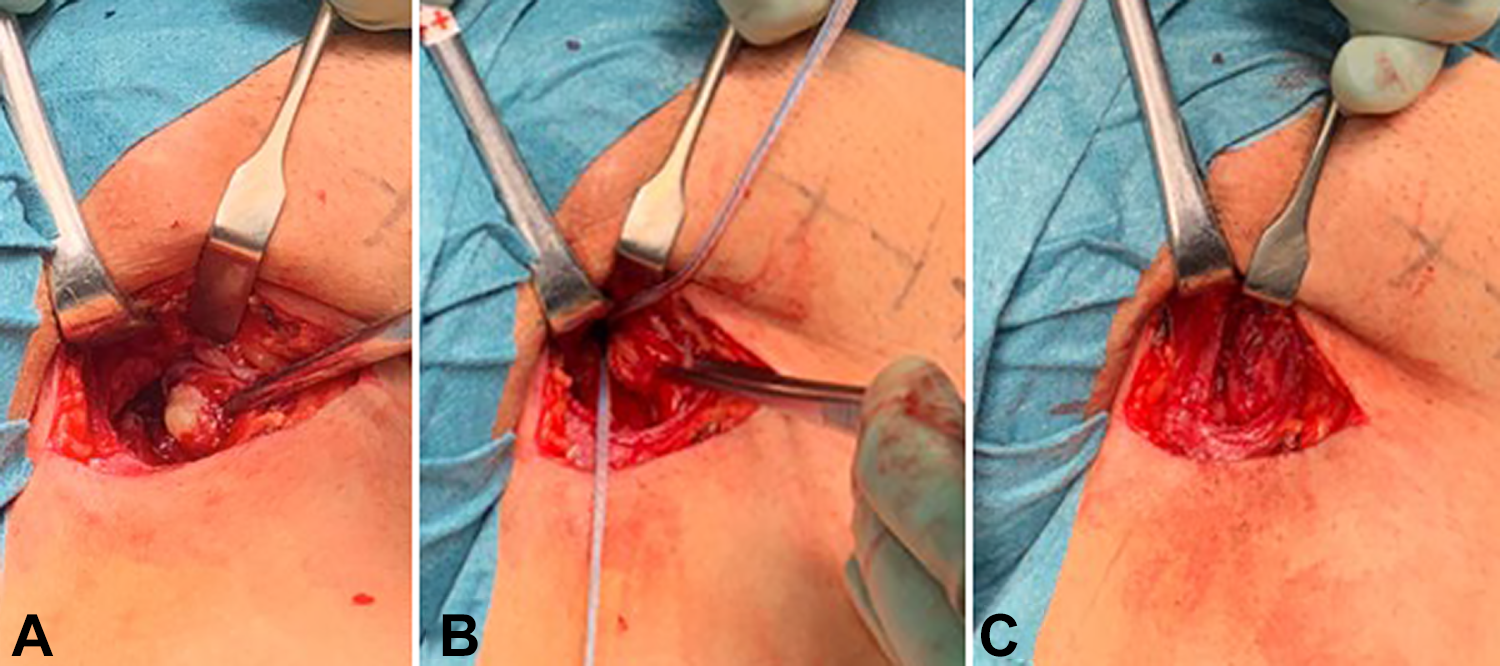
Operative images of left AL repair. (A) Acute AL tendon with a retraction. (B) Two anchors are inserted into the anatomic origin site on the pubic bone. (C) The AL tendon is reinserted and fixed to the pubic bone, and the attachment area is reinforced by a fascia flap. AL, adductor longus.
After the direct repair of the ruptured tissue, a Bovey cautery device was used to perform transverse release of the superficial fascial layer of the AL at 4 to 5 cm distal to the pubic bone insertion in accordance with previous descriptions. 6,12 This partial release, which was performed on the superficial fibers of the AL, addressed the layer that is under relatively greater tensile loads during AL activation. The rationale to add this partial release to the procedure was to decrease the risk of postoperative AL tightness, which could by itself become a source of disabling symptoms and reduce strength in athletes. 12 In cases that involved additional distal muscle-tendon area ruptures, a longitudinal skin incision was preferred, overlying the AL course to enable a larger exposure. The lesioned tissue was directly repaired side-to-side using absorbable Vicryl or PDS 3-0 sutures, utilizing the gliding Z-plasty technique described earlier to avoid excessive adductor tightness. 7 Some cases involved concomitant tendon tears such as the adductor magnus, adductor brevis, gracilis, pectineus, and oblique abdominal fascia as seen on the preoperative MRI (Figure 3). In these cases, another incision was made transversally just proximal to the inguinal ligament to allow exposure and repair of the torn oblique abdominal muscle fascia (conjoined tendon) to the pubic bone using sutures. In these cases, it is important to be aware of the obturator nerve, which descends between the AL and the adductor brevis muscles. The distal fascial release was performed in these cases as described. Subcutaneous tissue was closed with absorbable sutures, and the skin closure was made with nonabsorbable sutures. No drain was used.
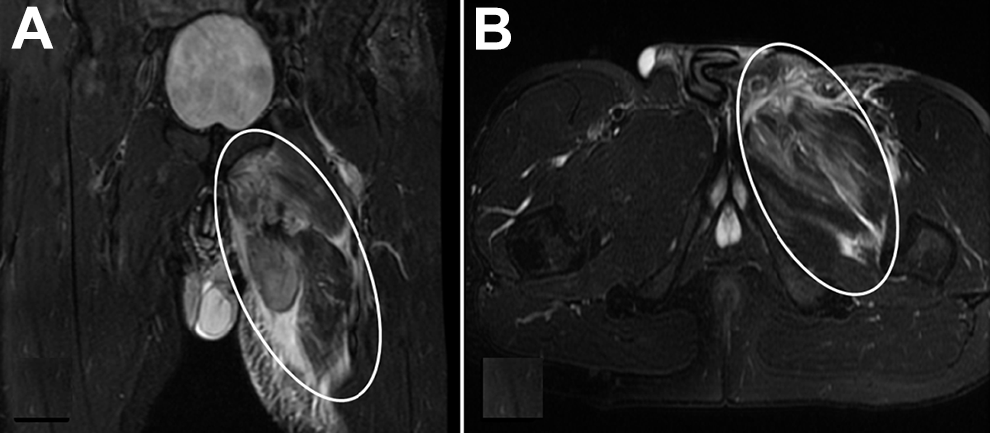
T2-weighted short tau inversion recovery magnetic resonance imaging (A) coronal view and (B) sagittal view of the pelvis demonstrating a case of complete left adductor group avulsion tears (circled).
Postoperative Rehabilitation Protocol
During the first postoperative week, walking with the use of crutches as needed and cold packing were recommended. During the second postoperative week, range-of-motion exercises as well as lower extremity muscle activations commenced. After removal of skin sutures at 2 weeks after surgery, aquatic training was allowed. At the third week, stationary bicycling and cross-training were allowed, together with light gym and rubber-band training. At the fourth postoperative week, more walking was encouraged with light jogging; additional stretching; strength training; and coordination, balance, and muscle activation. At the fifth week, running was allowed, and after 6 weeks, sprinting and kicking were permitted. Return to full training was allowed at 2 to 3 months postsurgically. Heterotopic ossification (HO) prophylaxis was not prescribed. Outpatient visits were scheduled at 2 weeks and then 1, 3, and 6 months after surgery. Additional visits were performed as needed to maintain adequate follow-up records regarding functioning of these patients. Postoperative ultrasound or MRI studies were not routinely performed.
Statistical Analysis
The desired sample size for this study was not based on power analysis calculations but was planned to be consistent with previous outcome studies that demonstrated the clinical benefit of surgical treatment in patients undergoing direct repair of tendinous-pelvic avulsions or repair of other muscle lesions of the thigh. 9,17 These consisted of between 30 and 40 athletes. 9,17 Descriptive statistics consisted of numbers with percentages for nonmetric variables, and medians with ranges or means with standard deviations for continuous variables. Continuous variables were checked for normality using the Shapiro-Wilk test. The Mann-Whitney nonparametric test was used for comparing continuous variables, and the Fisher exact test was used for comparing nominal variables. The following potential associated factors for inferior outcomes were compared between patients with self-reported outcomes of excellent versus those outcomes rated as good or moderate: (1) age at injury (years); (2) preinjury Tegner score; (3) interval between injury and surgery (weeks); and (4) number of adductor tendons involved (ie, isolated AL tear cases as opposed to AL tear with concomitant tendons involved). In addition, outcomes and time from injury to surgery were compared between the subgroup of patients that had AL repair with concomitant tendons repair (ie, gracilis, adductor brevis, adductor magnus, oblique abdominal fascia, and pectineus) and the other patients who had repair of the AL only. The P value to reject the null hypothesis was set at .05. Statistical analyses were performed using IBM SPSS-22 software (SPSS).
Results
A total of 40 male athletes were included in the evaluation. Of these, 36 had AL repair, whereas 4 patients had AL with concomitant tendon repair. Median age at surgery was 25 years (range, 18-48 years) (Table 1). Follow-up was an average 11 months (range, 6 months-8 years).
Patient Demographics, Injury, and Surgery Characteristics and Outcomes a

a AL, adductor longus.
In total, 25 cases (63%) occurred while playing soccer. Regarding the mechanism of injury, most cases were low-energy tears because of eccentric overload while playing soccer (36 cases involved the AL and 1 case involved the AL and gracilis tendons). Four cases involved higher-energy falls during downhill skiing, of which 3 had repair within 10 days of the injury of concomitant lesions in addition to the AL tear, also involving the gracilis, the adductor brevis, the adductor magnus, the oblique abdominal fascia, and the pectineus. In 3 cases, a small bony fragment avulsion of the pubic bone was excised to enable direct reattachment of the tendon without excessive tissue bulk at the repair site.
The preinjury Tegner level was median 9 (range, 5-10). Twenty-six (65%) of the cases involved high-level competitive sports corresponding to Tegner levels 8-10, and from these 26, 23 cases were soccer players (88%). The interval between injury and surgery was 1-35 weeks (mean 6 weeks) whereas 30 cases (75%) were operated in the acute or subacute phase (within 4 weeks from injury). Self-reported outcome at follow-up was excellent in 23 (58%), good in 13 (33%), and moderate in 4 (10%) patients. There were no outcomes graded as fair or poor. Comparisons between patients with excellent (23 patients) versus good/moderate (17 patients) outcomes revealed no significant differences regarding age at injury (27 ± 8 vs 29 ± 6; P = .2), preinjury Tegner score (8.3 ± 2 vs 8.3 ± 1; P = .5), or number of injured tendons (2 cases of 23 patients vs 2 cases of 17 patients; P ≥ .999).
The time interval between the injury and surgical repair was found to be a significantly influential factor with regard to outcomes. Athletes with outcomes classified as excellent were operated within a shorter time interval from the injury compared with athletes with good/moderate outcomes (2.4 ± 1.8 vs 11.4 ± 11.0 weeks; P < .01). Outcomes in the subgroup of patients who had AL with concomitant tendons repair (n = 4; excellent in 50% and good/moderate in 50%) were not significantly different compared with patients who had only AL tendon repair (n = 36; excellent in 58% and good/moderate in 42%) (odds ratio = 1.4 [95% CI, 0.18-11.1]; P ≥ .99; Fisher exact test). Time interval between injury and surgery was significantly shorter in the subgroup of patients that had AL with concomitant tendon repair compared with the subgroup that had only AL tendon repair (ie, 2 ± 1.3 vs 6.7 ± 8.5 weeks; P < .01).
There were 3 cases (7.5%) that presented postoperative complications and required reoperation. This involved partial adductor releases and suture material removal due to hypertrophic scar formation. Wound infections were noted in 3 cases, of which 2 resolved with oral antibiotics and the third was treated with scar removal and partial adductor release. There were no neurological compromises. None of the cases developed heterotopic bone.
Discussion
There are 2 major findings in this study. (1) Proximal AL repair with concomitant distal fascial release for athletes who had complete AL tears resulted in excellent or good outcomes in 90% of cases. This accounted for the athletes’ ability to return to preinjury sports activities without or with only minor symptoms. (2) Athletes with excellent outcomes were found to undergo proximal AL repair within a shorter time interval from the injury compared with athletes with good/moderate outcomes (2.4 ± 1.8 vs 11.4 ± 11.0 weeks; P < .01). In other words, operative treatment within the first month after the injury was associated with improved outcomes compared with surgical repair at later stages following a trial of nonoperative management. These findings are in concordance with previous case reports that advocated direct repair of complete AL tendon tears in athletes. 11,19 The small subset of patients in this series who had concomitant tendon repair in addition to the AL had almost similar rates of excellent outcomes to isolated AL cases despite the extensiveness of the injury, possibly because these more extensive lesions were associated with earlier intervention, which seemed by itself a favorable prognostic factor in this series. It should be remembered, nevertheless, that despite these apparently compelling findings, the decision on whom to operate early and who should be managed nonoperatively may not always be straightforward depending on the extent of the tear and amount of tendon retraction. However, based on the current findings, there are 2 scenarios where surgery should be strongly considered in athletes. One is when the tendon is retracted to more than 2 cm and a clear gap can be felt at the ruptured area. This ruptured tendon should be viewed as unstable, and surgery is therefore suggested. A second scenario is following nonoperative management, which results in a tightly scarred tendon causing continued groin pain that may prevent the athlete from returning to play.
The surgical approach that was used in this series promotes the re-creation of adductor anatomy and at the same time decreases the risk of developing adductor tightness. This may decrease the risk of developing chronic groin pain and athletic pubalgia, which can be a challenging problem in athletes and difficult to resolve, 4,5 particularly in high-level professional athletes involved in pivoting sports. Of note, despite performing direct repair of the lesioned tissue with concomitant partial release to potentially ease future groin discomfort, 12 40% of athletes in this series still reported some groin discomfort during activities at follow-up, reflecting how challenging the adductor musculature is to treat. This may be consistent with a recent description of MRI scans of injured athletes showing that the proximal AL was rarely lesioned in isolation and more frequently comprised only 1 lesioned structure among other lesions within the interconnected complex that included also the pyramidalis, the anterior pubic ligament, the AL fibrocartilage, and the pectineus. 13 This suggests that some of the lesions in this complex area may have been missed, even in the current series, despite identifying and treating in some of the cases not only the AL tendon but also concomitant lesions that included the pyramidalis muscle, oblique fascia, the adductor magnus and brevis, and the gracilis tendons. This also emphasizes the need of the surgeon to be familiar with anatomic interconnections between the lower abdominal muscles and fascial layers and the groin fascia and tendons 5 to be able to repair the lesioned structures without improperly overtightening soft tissues or overlooking some of the injuries.
None of the patients in this series were female. In previous series of severe muscle and tendinous lesions around the hip and thigh areas, such as hamstring tears and thigh muscle tears, a similar male predominance was reported. 8,9 Although the reasons for this clear sex predominance are unclear, the findings do support these injuries’ being extremely unlikely to occur in women.
In this series, HO prophylaxis was not prescribed, and HO did not develop. Although HO can lead to substantial disability in high-level athletes, who may require surgical intervention in some cases, 8,9 the current series does not support routinely prescribing postoperative HO prophylaxis following AL repair.
Limitations of this series include the retrospective design and lack of a control group. Because of this design and the fact that these lesions do not always lead to severe swelling or ecchymosis, it is possible that other athletes with acute groin injuries and possibly with AL tears have healed without even undergoing diagnostic MRI, so that their injuries may have not been fully documented. In this case, the cohort of this study would have been subjected to a selection bias. Nevertheless, the relative homogeneity of the series in terms of patient characteristics and the surgical approach described may allow for future comparisons of the current series against similar populations treated by other strategies to further refine the preferred treatment approach for these lesions. In addition, adductor peak torque was not objectively measured on isokinetic dynamometer. Thus, while previous reports showed that in chronic adductor-related groin pain, partial adductor tendon release resulted in recovery of adductor strength, 6 despite the high proportion of return to high-level sports in this series, which likely required regaining nearly full if not full adductor strength following the repair, it cannot be determined, based on the data presented, whether muscle torque fully recovered.
Conclusion
Surgical repair for complete proximal AL tears with a concomitant distal fascial release results in good or excellent outcomes in 90% of cases. This treatment should be considered particularly in high-level athletes with a clear tendon retraction and within the first month following the injury. Further research is nevertheless needed to compare these outcomes with other treatment alternatives to better define criteria advocating surgery.
Footnotes
Final revision submitted April 13, 2021; accepted June 8, 2021
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Mehiläinen NEO.