
Abstract
Background:
The association between prolonged postoperative opioid use on outcomes after hip preservation surgery is not known.
Purpose:
To compare minimum 2-year patient-reported outcomes (PROs) between patients who required ≥1 postoperative opioid refill after undergoing hip arthroscopy for femoroacetabular impingement syndrome (FAIS) versus patients who did not require a refill and to identify preoperative predictors for patients requiring ≥1 postoperative opioid refill.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Data from consecutive patients who underwent arthroscopic surgery for FAIS between January 2012 and January 2017 were analyzed. Multivariate regression analysis was performed to classify patient and radiographic variables as predictive of requiring ≥1 opioid prescription refill after surgery. Patients completed the following PROs preoperatively and at 2-year follow-up: Hip Outcome Score— Activities of Daily Living subscale (HOS-ADL), HOS–Sports Subscale (HOS-SS), modified Harris Hip Score (mHHS), International Hip Outcome Tool (iHOT-12), and 100-point visual analog scale (VAS) for pain and satisfaction. Scores were compared between patients needing additional prescription opioids and those who did not.
Results:
A total of 775 patients, of whom 141 (18.2%) required ≥1 opioid prescription refill, were included in the analysis. Patients requiring opioid refills had significantly lower 2-year postoperative PRO scores compared with patients not requiring refills: HOS-ADL (79.9 ± 20.3 vs 88.7 ± 14.9), HOS-SS (64.6 ± 29.5 vs 78.2 ± 23.7), mHHS (74.2 ± 21.1 vs 83.6 ± 15.9), iHOT-12 (63.6 ± 27.9 vs 74.9 ± 24.8), and VAS satisfaction (73.4 ± 30.3 vs 82.2 ± 24.9), as well as significantly more pain (26.8 ± 23.4 vs 17.9 ± 21.8) (P ≤ .001 for all). Predictors of requiring a postoperative opioid refill included patients with active preoperative opioid use (odds ratio, 3.12 [95% confidence interval, 1.06-9.21]; P = .039) and larger preoperative alpha angles (odds ratio, 1.04 [95% confidence interval, 1.01-1.07]; P = .03).
Conclusion:
Patients requiring ≥1 opioid prescription refill after hip arthroscopy for FAIS had lower preoperative and 2-year PRO scores when compared with patients not requiring refills. Additionally, active opioid use at the time of surgery was found to be predictive of requiring additional opioids for pain management.
Keywords
The United States is currently battling an opioid epidemic, where the overuse and misuse of opioid medication has become an increasingly significant cause of death. 22,29,30 Since the late 1990s, the growing number of physician prescriptions of opioids for pain control has contributed directly to the current crisis. 38 As of 2015, orthopaedic surgeons were found to be among the top prescribers of opioid analgesics within the medical specialties. 25 Consequently, health policy officials and the medical community have emphasized the need for reform in how patient pain is managed. 32
Recently, there has been an increase in studies evaluating the prevalence of opioid use and its effect in orthopaedic surgery. In a review of 1208 patients who underwent hip arthroscopy, Westermann et al 41 found that 24.9% filled a prescription for opioid medication within 1 to 3 months prior to surgical intervention. Use of opioids preoperatively is associated with prolonged postoperative opioid use, greater postoperative pain, lower physical function, and increased mortality rates after undergoing orthopaedic surgical procedures. 1,15,19,24,26,43 Although prior studies have investigated the risk factors for prolonged opioid use, there is a paucity of literature on the association between extended opioid use on patient-reported outcome (PRO) measures, particularly in patients undergoing arthroscopic hip preservation surgery. Recognizing and understanding the risk factors for extended opioid use in patients with femoroacetabular impingement syndrome (FAIS) may allow providers to identify at-risk patients.
The purpose of this study was to (1) compare preoperative and minimum 2-year reported outcomes in patients undergoing hip arthroscopy for femoroacetabular impingement who required ≥1 postoperative opioid refill versus patients who did not and (2) identify preoperative predictors for patients requiring ≥1 postoperative opioid refill. We hypothesized that patients requiring additional use of opioids would have lower mean preoperative and postoperative outcome score and that prior history of opioid use would be predictive of requiring continued opioid prescription use for postoperative pain control.
Methods
Patient Enrollment
After the study received approval by our institutional review board, data collected prospectively from patients who underwent primary hip arthroscopy for FAIS by 1 fellowship-trained hip arthroscopist (S.J.N.) between January 2012 and January 2017 were extracted retrospectively for analysis. Study inclusion criteria consisted of patients diagnosed with FAIS based on previously established criteria, 10 whose nonoperative treatment had failed (eg, lifestyle modification, physical therapy sessions, nonsteroidal anti-inflammatory drugs, intra-articular injections), who underwent elective hip arthroscopy, and who had a record in their electronic medical record (EMR) of filling the opioid medication prescribed routinely by the senior author (S.J.N.) for pain control after surgery. Exclusion criteria consisted of patients with follow-up of <2 years from the date of surgery, with a history of contralateral or ipsilateral hip surgery, undergoing concomitant procedures for extra-articular pathology (eg, gluteal tendon tear repair, psoas release, iliotibial band lengthening, trochanteric bursectomy, subspine impingement), and with a history of pediatric hip conditions (eg, avascular necrosis, developmental hip dysplasia, slipped capital femoral epiphysis). General exclusions for the senior author’s performing surgery to treat FAIS included Tönnis grade ≥2 and hip dysplasia (lateral center-edge angle [LCEA] ≥20°).
Radiographic Analysis
Patients in the study group all received preoperative radiographic films, as well as postoperative radiographs at 1-month follow-up. 39 Each series consisted of a standing anteroposterior (AP) pelvis, a false-profile hip, and a 45° Dunn lateral hip radiograph. 6 Measurements of interest included alpha angle, Tönnis angle, Tönnis grade, LCEA of Wiberg, and anterior center-edge angle (ACEA). 17,28,36 All radiographic measurements were made by the senior author (S.J.N.) and confirmed by an orthopaedic fellow.
Surgical Technique
All surgical procedures were performed by a surgeon (S.J.N.) trained in hip preservation surgery using a similar technique that has been well described previously. 11,33 Briefly, after anterolateral and midanterior portals were established, an interportal capsulotomy was performed to address central compartment pathology, including acetabular rim trim and labral tear repair. Once completed, traction was released, and the interportal capsulotomy was extended inferiorly to create a T-capsulotomy for peripheral compartment access. If cam morphology was present, it was resected until adequate femoral head-neck offset was completed. A dynamic examination of the treated leg was performed to confirm resolution of bony impingement. Both limbs of the capsulotomy were closed, with vertical limb plication performed depending on the degree of capsular laxity. Of note, all patients underwent general anesthesia with no regional or local anesthesia.
Postoperative Care and Physical Rehabilitation
All patients began rehabilitation on postoperative day 1 using a protocol similar to those described previously. 20,21 Standard postoperative pain management for patients undergoing hip arthroscopy included prescribing 30 hydrocodone-acetaminophen tablets (5-325 mg) for postoperative use with instructions to take 1 or 2 tablets orally every 4 to 6 hours for pain as needed. If this medication was not tolerated, patients were prescribed 30 tramadol tablets (50 mg) with instructions to take 1 tablet every 6 hours for pain relief as needed. No additional medications for postoperative pain management (eg, nonsteroidal anti-inflammatory drugs) were prescribed. The same pain management regimen was used for both opioid-naïve patients and patients with a past history of opioid prescription use. Refills for the opioid medication were not provided on the initial prescription, and additional opioid prescriptions were made on a case-by-case basis if requested by the patient. As a general rule in the senior author’s practice: no patient request for refill was denied; however, patients were counseled on the risk of opioid dependence and the number of tablets provided. Furthermore, the same prescription was generally refilled. As the standard of care for providing narcotic prescriptions in hip arthroscopy had not been established, the protocol utilized by the senior surgeon was based on his clinical experience with the intention of providing the least amount of narcotic needed for pain relief. In addition, all patients were prescribed a 10-day course of indomethacin (75 mg) for heterotopic ossification prophylaxis. 37 Last, prolonged postoperative opioid use was defined as requiring ≥1 prescription opioid refill after surgery in addition to what was routinely prescribed after hip arthroscopy. Of note, all study participants were confirmed by chart review to have been prescribed the routine postoperative pain management medication during the retrospective data analysis.
Patient Variables and Functional Outcomes
All the variables included in the analysis were extracted from the senior author’s patient database and confirmed via EMR review. Past opioid use was defined as taking prescription opioids at any point for the hip pain. Other variables, including history of past smoking, were marked as “yes” if there was evidence of it at any point in the EMR or it was self-reported.
Patients included in the analysis had completed preoperative hip-specific PRO instruments both preoperatively and at 2-year follow-up. The PROs included the Hip Outcome Score— Activities of Daily Living subscale (HOS-ADL), 23 HOS–Sports Subscale (HOS-SS), the modified Harris Hip Score (mHHS), and the International Hip Outcome Tool (iHOT-12) questionnaires. In addition, patients reported their level of pain and satisfaction using a visual analog scale (VAS) ranging from 0 to 100. 5,12 Preoperative and 2-year postoperative scores were collected via online-based surveys using an encrypted and secure data collection system (Oberd).
Statistical Analysis
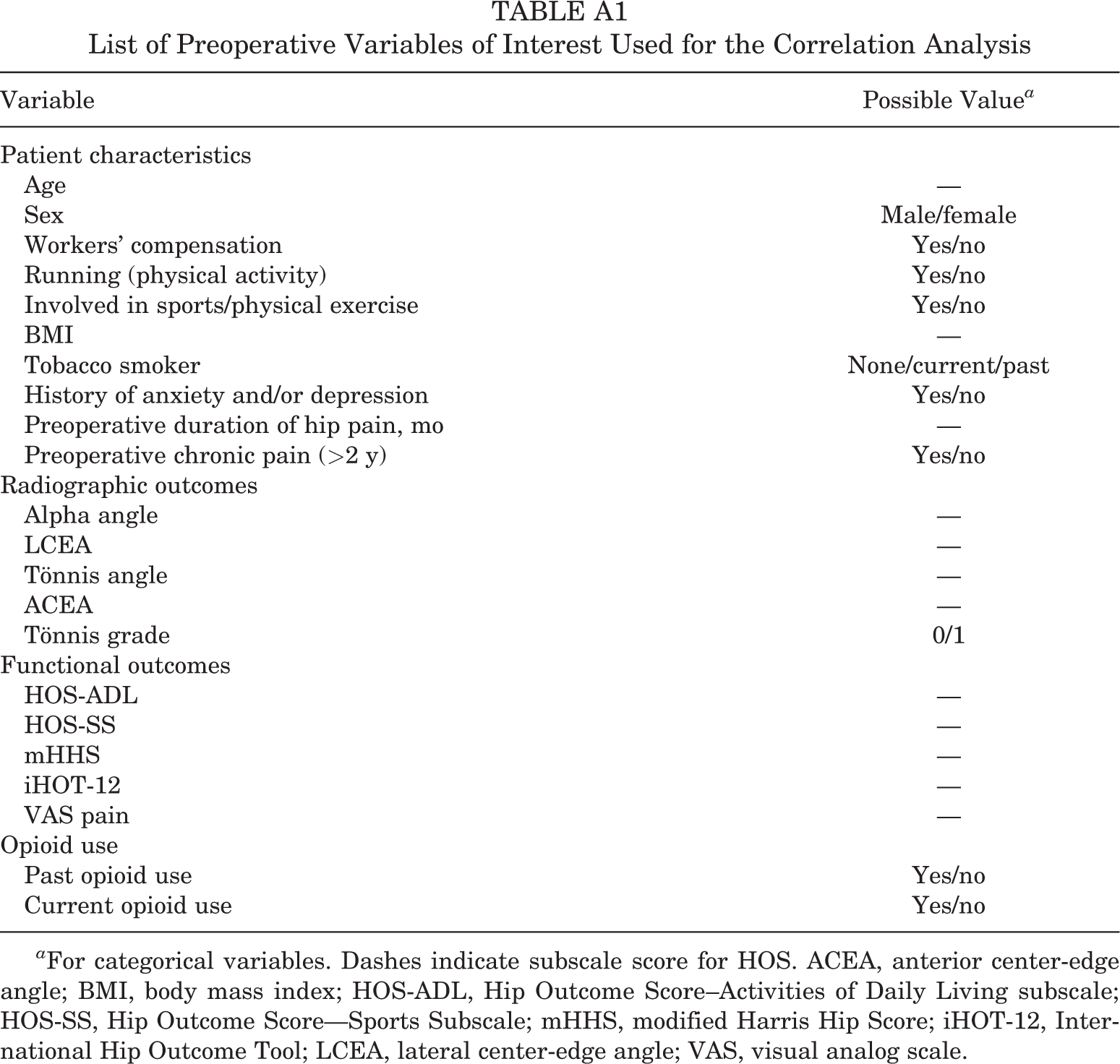
Data were confirmed to have met parametric statistical assumptions prior to analysis. Independent-samples t test was performed to assess for differences in PROs between patients with and without postoperative narcotic refills. A multivariate logistic regression model was performed to identify preoperative variables predictive of requiring additional prescription opioid pain management. Preoperative variables are listed in Appendix Table A1 and include demographic, radiographic, and preoperative functional outcomes, as well as history of preoperative prescription opioid use. To avoid multicollinearity in the logistic regression analysis, we performed a Pearson coefficient and Spearman coefficient analysis to determine correlations between continuous and categorical variables, respectively. Any variable that had a statistically significant correlation (P < .05) with postoperative opioid use was tested in the final regression model. Any preoperative variables that demonstrated statistical correlation with each other (P < .05) were placed separately into different models, with the best-fit model used as the final regression model. In addition, a subanalysis was performed to determine whether active opioid use at the time of surgery or a history of opioid prescription use prior to surgery was a stronger predictor of requiring additional pain control after surgery. Receiver operating characteristic (ROC) curve analysis was used to determine the appropriate fitness of the predictive models in the study population, with an area under the curve (AUC) >0.700 indicating good accuracy of the model. 14 All statistical tests were 2-tailed, and the statistical difference was established at a 2-sided α level of .05 (P < .05). All statistical analysis was performed using SPSS Version 25 (IBM Corp).
Results
Of the 934 patients who met inclusion criteria, 775 (83.0%) had 2-year minimum follow-up and were included in the final analysis (Figure 1). Of the total study group, 141 (18.2%) patients required ≥1 opioid prescription refill after surgery in addition to the routine opioid prescribed postoperatively to every patient after hip arthroscopy. The mean age and body mass index (BMI) of the study group was 33.9 ± 12.3 years and 25.5 ± 8.6, respectively. Comparison of characteristics between the refill and no refill groups demonstrated a statistical difference between age (35.9 ± 11.6 vs 33.5 ± 12.4 years; P = .03), and BMI (27.2 ± 6.1 vs 25.1 ± 9.0; P = .001) (Table 1).
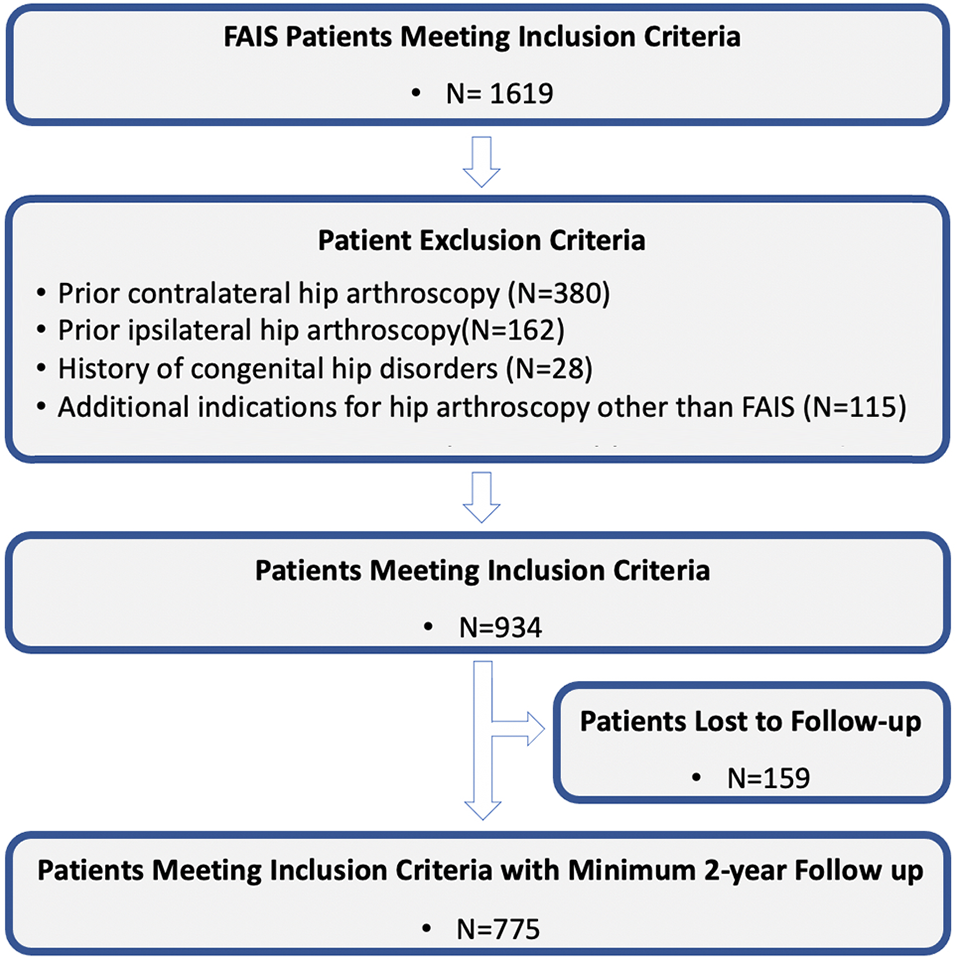
Flowchart of patient selection. FAIS, femoroacetabular impingement syndrome
Combined Cohort Patient Characteristics a

a Data are reported as mean ± SD or n (%). Bold P values indicate statistically significant difference between groups (P < .05).
Radiographic Findings
The analysis comparing radiographic findings of the 2 groups is detailed in Table 2. There was a statistically significant difference between groups in the alpha angle measurement on AP radiographs (78.8 ± 13.1 vs 75.2 ± 12.2; P = .019). There was no statistically significant difference between any of the other pre- or postoperative radiographic parameters. Tönnis grade, Tönnis angle, and the ACEA approached, but did not reach, significance.
Comparison of Radiographic Findings Between Opioid Refill Status Groups a
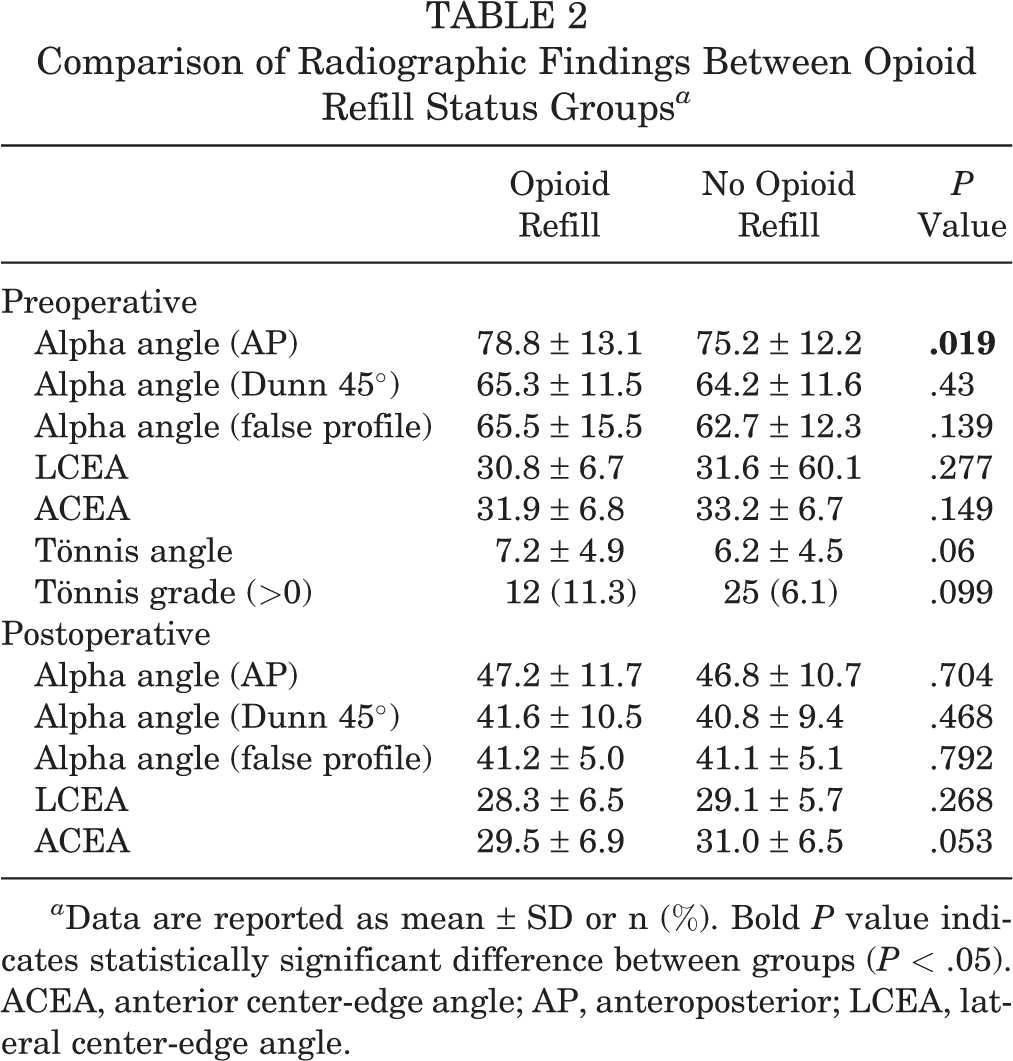
a Data are reported as mean ± SD or n (%). Bold P value indicates statistically significant difference between groups (P < .05). ACEA, anterior center-edge angle; AP, anteroposterior; LCEA, lateral center-edge angle.
Analysis of Pre- and Postoperative Functional Scores
The results of the independent-samples t test analysis comparing PRO score averages between the 2 groups are summarized in Table 3. Analysis of baseline scores demonstrated that patients requiring opioid refills had significantly lower preoperative HOS-ADL (54.8 ± 20.5 vs 66.3 ± 17.5; P < .001), HOS-SS (32.7 ± 23.2 vs 42.5 ± 22.1; P < .001), mHHS (50.6 ± 15.4 vs 59.6 ± 14.3; P < .001), and iHOT-12 (28.4 ± 18.6 vs 36.8 ± 16.8; P < .002) score averages when compared with patients with no opioid refills. However, there was no statistically significant difference in baseline VAS pain between the 2 groups (P = .590). Analysis of postoperative scores demonstrated patients requiring refills had significantly lower postoperative HOS-ADL (79.9 ± 20.3 vs 88.7 ± 14.9; P < .001), HOS-SS (64.6 ± 29.5 vs 78.2 ± 23.7; P < .001), mHHS (74.2 ± 21.1 vs 83.6 ± 15.9; P < .001), iHOT-12 (63.6 ± 27.9 vs 74.9 ± 24.8; P = .001), and satisfaction (73.4 ± 30.3 vs 82.2 ± 24.9; P = .001) averages, as well as greater pain (26.8 ± 23.4 vs 17.9 ± 21.8; P < .001) when compared with the no-refill group.
Assessment of Functional Score Changes Over Time Between Opioid Refill Status Groups a
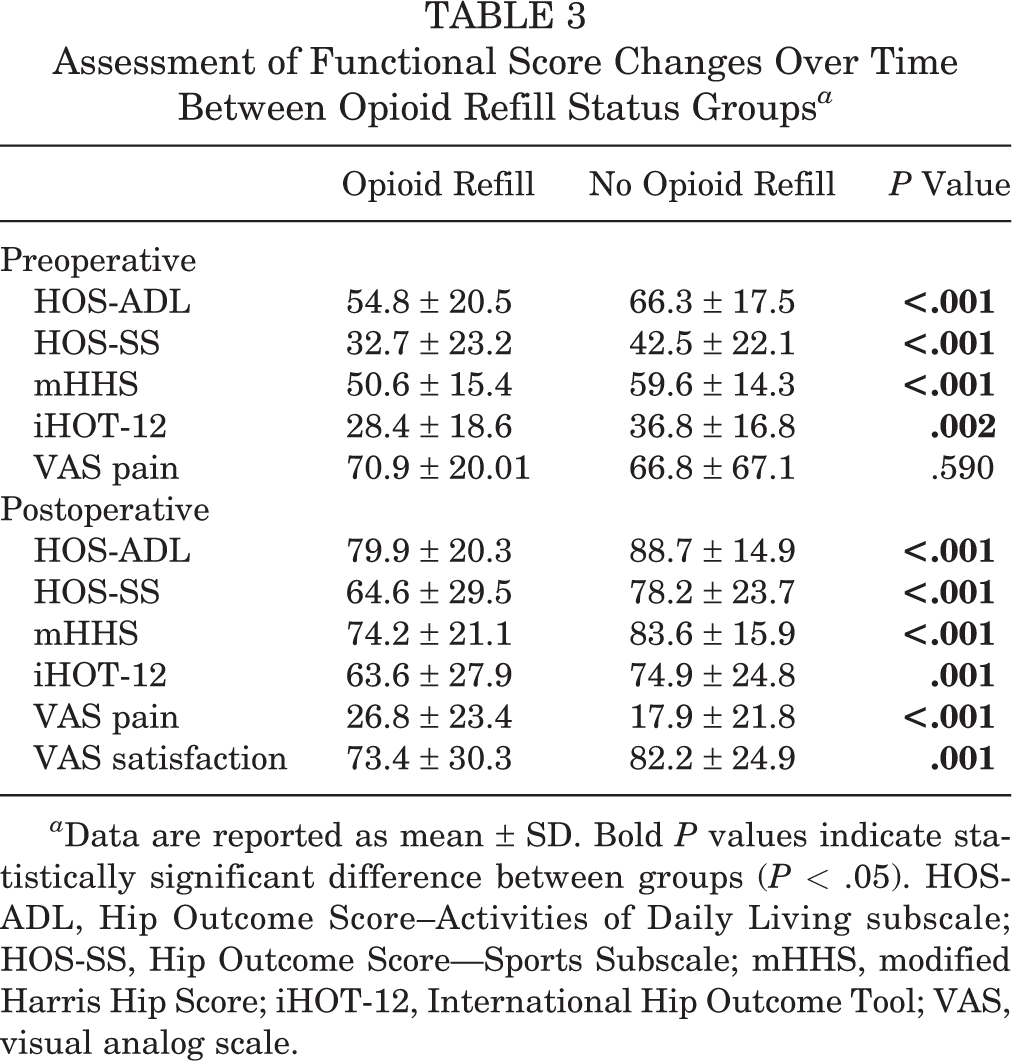
a Data are reported as mean ± SD. Bold P values indicate statistically significant difference between groups (P < .05). HOS-ADL, Hip Outcome Score--Activities of Daily Living subscale; HOS-SS, Hip Outcome Score— Sports Subscale; mHHS, modified Harris Hip Score; iHOT-12, International Hip Outcome Tool; VAS, visual analog scale.
Predictors of Requiring Additional Opioid Prescription Refills for Pain Management
Logistic regression analysis demonstrated that preoperative predictors of requiring additional postoperative opioids included patients with a history of opioid use prior to surgery (odds ratio [OR], 4.04; 95% CI, 1.99-8.19; P < .001) and larger preoperative AP alpha angles (OR, 1.04; 95% CI, 1.01-1.07; P = .03) (Table 4). ROC curve analysis demonstrated that the model had good accuracy of prediction among the study population (AUC = 0.718) (Appendix Figure A1). Subanalysis of patients with a history of and those with active prescription opioid use at the time of surgery demonstrated that active use was predictive (OR, 3.12; 95% CI, 1.06-9.21; P = .039), whereas past opioid use was not. ROC curve analysis demonstrated that this model had good accuracy of prediction among the study population as well (AUC = 0.710) (Appendix Figure A2).
Logistic Regression Models for Predictors of Prolonged Postoperative Opioid Use and Subanalysis of Preoperative Opioid Use a
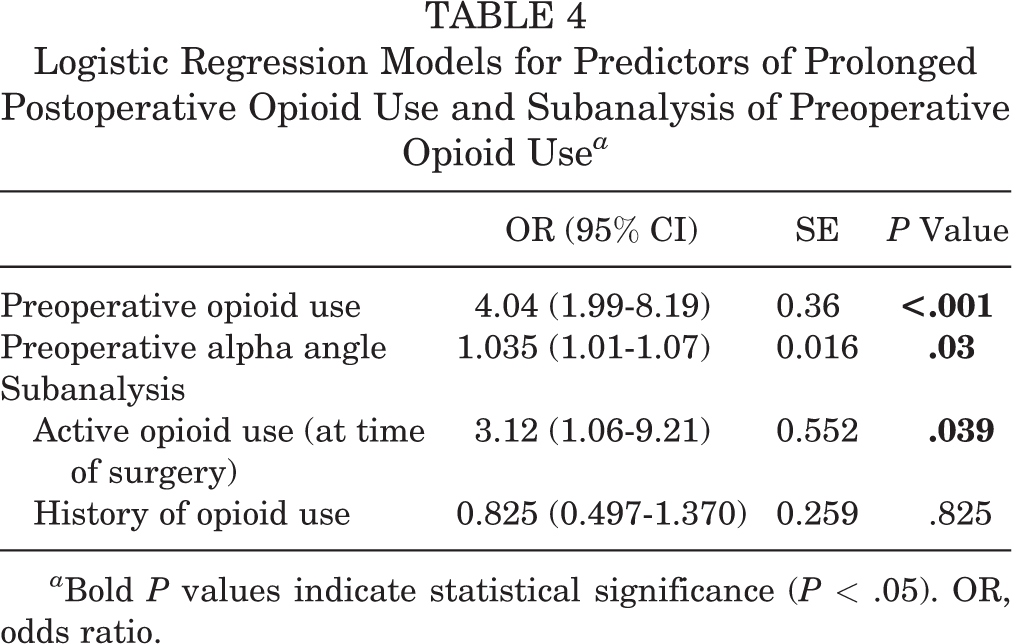
a Bold P values indicate statistical significance (P < .05). OR, odds ratio.
Discussion
In this study, we found that patients requiring ≥1 opioid prescription refill after hip arthroscopy for FAIS demonstrated lower baseline and postoperative 2-year reported outcome scores in comparison with patients not requiring additional opioid medications. Active opioid use at the time of surgery was found to be a strong predictor of requiring ≥1 additional opioid refill above a standardized postoperative course. As such, our hypothesis was partially confirmed. Although we found that prior opioid use was predictive of needing additional postoperative opioid prescriptions for pain management, this was the case only in the subset of patients actively taking opioids.
Several prior studies have shown that opioid consumption prior to hip arthroscopic surgery strongly predicts prolonged postoperative use. Anciano Granadillo et al 2 found that preoperative opioid use was the most significant risk factor for prolonged postoperative opioid use after hip arthroscopy at an OR of 3.61. Similarly, Westermann et al 41 demonstrated an OR of 18.6 for opioid prescription filling 3 months postoperatively in patients who took opioids within 3 months of hip arthroscopy compared with opioid-naïve patients. In both studies, rates of opioid refills between 3 and 6 months postoperatively were reported as 17.4% and 24.7%, respectively. Both studies were performed using large insurance databases, which have intrinsic limitations from a data collection aspect. The strength of our study lies in its single-surgeon cohort of a larger number of patients with FAIS only, treated using comprehensive capsular management techniques. All patients received the same standardized postoperative pain protocol, and thus, any patient requiring a refill represented a deviation from this. Our findings are corroborated by an increasing number of studies linking preoperative opioid use to prolonged opioid utilization following total knee arthroplasty, 26 spine surgery, 16 shoulder arthroplasty, 31 anterior cruciate ligament reconstruction 4 , and knee and shoulder arthroscopy. 9,34
In addition to preoperative opioid consumption, previous studies in the orthopaedic literature have identified other risk factors for prolonged opioid use for postoperative pain management. Wu et al 42 performed a meta-analysis that included 416,321 patients undergoing total joint arthroplasty and observed a 12% prevalence of prolonged opioid use after surgery. These authors also demonstrated that preoperative opioid use had the highest relative risk for extended use of opioid prescriptions, followed by posttraumatic stress disorder, benzodiazepine use, tobacco use, and additional sources of pain. 42 In another study, Anderson and colleagues 3 used a large health care database to identify risk factors of prolonged opioid dependence after anterior cruciate ligament reconstruction among military patients. As in the previous study, the authors identified preoperative opioid pain control as a major risk factor, as well as gender, age, and a history of substance abuse. In the current study, cam lesions with larger preoperative alpha angles were predictive of requiring ≥1 opioid prescription refills after surgery. These findings coincide with those observed in previous studies that patients with larger femoral cam lesions tend to have poorer postoperative outcomes and to achieve clinically significant outcomes at lower rates. 8,35 However, with an OR close to 1.0, the effect of an increased alpha angle on opioid dependence is likely minimal.
Through a subanalysis, we demonstrated that active opioid use at the time of surgery was more accurate for predicting additional postoperative prescription opioid use than was prior history of opioid use without an active prescription. Patients actively using opioids at the time of hip arthroscopy have been shown to exhibit lower outcome scores as measured using subjective hip joint pain, function, and general health compared with opioid-naïve patients. 40 Westermann et al 40 showed respective 15- and 13-point differences in the Hip disability and Osteoarthritis Outcome Score pain and physical function in these 2 patient populations. However, patients with previous opioid use, but not within 3 months prior to surgery, did not exhibit lower outcome scores compared with opioid naïve patients. Our findings, along with those of Westermann et al, 40 indicate an important distinction in predicting at-risk patients for prolonged postoperative opioid use: that opioid use at the time of surgical intervention is the strongest risk factor.
To our knowledge, this is the first study that has reported on 2-year postoperative PROs in patients needing ≥1 postoperative opioid prescription refill after FAIS surgery. In each of our hip-specific PROs, including HOS-ADL, HOS-SS, mHHS, and iHOT-12, we saw a statistically significant decrease in score at a minimum 2 years postoperatively in the opioid refill group compared with those not refilling. The same group also demonstrated lower preoperative scores. This finding gives surgeons objective data when counseling patients on expected outcomes. Preoperatively, patients actively using opioids may be counseled that there is increased risk for a limited improvement in PRO. In addition, in the early postoperative period, patients with extended analgesic demands should be counseled on an increased risk for limited outcome improvement. Interestingly, the preoperative VAS pain scores were not different in the 2 groups. A potential explanation for the observed worse outcomes could be a higher incidence of chronic hip pain seen in patients requiring additional opioid use rather than a higher intensity of pain. This is supported by a recent analysis of >1000 patients undergoing hip arthroscopy for FAIS that demonstrated that chronic preoperative pain is associated with clinical failure (revision arthroscopy or conversion to total hip arthroplasty). 27 It is possible, however, that the association between the need for prolonged opioid pain management and lower outcome scores is multifactorial and includes causal relationships with other factors including psychological and social demographics.
Current practices of prescribing opioid medication for postoperative pain management are limited because of the lack of standardized protocols. Recent studies have evaluated the effect of modifying postoperative pain management modalities to decrease postoperative narcotic medication use or eliminating their use altogether. In a randomized controlled trial, Hartwell et al 13 compared the number of opioid pills consumed among a group of patients undergoing partial meniscectomy that was provided postoperative multimodal pain control with aspirin, acetaminophen, naproxen, and oxycodone versus a group that received the multimodal pain control medications without oxycodone but given the opportunity to fill an oxycodone prescription if needed. While the study indicated that there was no significant reduction in the number of tables utilized and days that opioids were required between both groups, more importantly, they demonstrated that 37% of patients did not require opioids postoperatively, and 86% used ≤8 of the 20 prescribed oxycodone tablets. 13 The findings of their study underscore the need for evaluating whether a multimodal approach of oral analgesics does in fact allow for reducing prescribing of opioids for postoperative pain management. Other multimodal pain strategies, such as intraoperative intra-articular injections, for reducing opioid prescription have been investigated previously. Cogan and colleagues 7 demonstrated in a retrospective study that patients who received an intra-articular injection of 10 mg of morphine and 100 µg of clonidine intraoperatively at the end of surgery required less treatment with narcotics for pain management during postsurgical recovery prior to discharge. Although the results of this study are promising, there is a need to determine whether intra-articular injections continue to provide appropriate analgesic effects over a longer period of time after patients are discharged from the recovery unit.
Limitations
There are a number of limitations in the current study that are worth noting. First, we did not include the time of onset of symptoms prior to intervention within our analysis. Patients whose diagnosis was delayed or whose presentation to a surgeon specialized in hip arthroscopy was delayed, may have had more prolonged symptoms and worse pathology. Delayed time to surgical intervention has been shown to result in worse midterm surgical outcomes. 18 Therefore, patients using preoperative opioids or requiring prolonged postoperative opioid use may have represented a sizable portion of patients with chronic hip pain from relatively delayed treatment, leading to the observed worse pre- and postsurgical reported outcome scores. Despite this potential mechanism, identifying patients with potential for prolonged opioid use merits appropriate counseling and closer follow-up. Second, we were not able to track opioid prescriptions provided by other physicians outside of our institution; however, this is likely to be a small number given that we were interested primarily only in patients requiring 1 additional narcotic prescription postsurgery. We are unable to comment on the incidence and outcome in patients requiring more than the initial refill. Last, the findings based on our statistical modeling may be limited to this particular data set, and these results should be confirmed in larger or different datasets in future research.
Conclusion
Patients requiring ≥1 opioid prescription refill after hip arthroscopy for FAIS had lower preoperative and 2-year patient reported functional scores when compared with patients not requiring refills. In addition, active opioid use at the time of surgery was predictive of requiring additional opioids for pain management.
Footnotes
Final revision submitted April 11, 2021; accepted May 4, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.U.N. has received grant support from Arthrex; education payments from Arthrex and Smith & Nephew; and hospitality payments from Stryker, Wright Medical, and Zimmer. J.D. has received grant support from Arthrex and Acumed, education payments from Smith & Nephew and Elite Orthopedics, and hospitality payments from Stryker. S.J.N. has received research support from Allosource, Arthrex, Athletico, DJO, Linvatec, Miomed, Smith & Nephew, and Stryker; education payments from Arthrex; consulting fees from Ossur and Stryker; and royalties from Ossur, Springer, and Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Rush University Medical Center (ORA No: 12022108-IRB01-CR07).
Appendix
List of Preoperative Variables of Interest Used for the Correlation Analysis
| Variable | Possible Value a |
|---|---|
| Patient characteristics | |
| Age | — |
| Sex | Male/female |
| Workers’ compensation | Yes/no |
| Running (physical activity) | Yes/no |
| Involved in sports/physical exercise | Yes/no |
| BMI | — |
| Tobacco smoker | None/current/past |
| History of anxiety and/or depression | Yes/no |
| Preoperative duration of hip pain, mo | — |
| Preoperative chronic pain ( |
Yes/no |
| Radiographic outcomes | |
| Alpha angle | — |
| LCEA | — |
| Tönnis angle | — |
| ACEA | — |
| Tönnis grade | 0/1 |
| Functional outcomes | |
| HOS-ADL | — |
| HOS-SS | — |
| mHHS | — |
| iHOT-12 | — |
| VAS pain | — |
| Opioid use | |
| Past opioid use | Yes/no |
| Current opioid use | Yes/no |
a For categorical variables. Dashes indicate subscale score for HOS. ACEA, anterior center-edge angle; BMI, body mass index; HOS-ADL, Hip Outcome Score–Activities of Daily Living subscale; HOS-SS, Hip Outcome Score— Sports Subscale; mHHS, modified Harris Hip Score; iHOT-12, International Hip Outcome Tool; LCEA, lateral center-edge angle; VAS, visual analog scale.