
Abstract
Background:
A large volume of systematic reviews and meta-analyses has been published on the effectiveness of sports injury prevention programs.
Purpose:
To provide a qualitative summary of published systematic reviews and meta-analyses that have examined the effectiveness of sports injury prevention programs on reducing musculoskeletal injuries.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
We searched the PubMed, CINAHL, EMBASE, and the Cochrane databases for systematic reviews and meta-analyses that evaluated the effectiveness of sports injury prevention programs. We excluded published abstracts, narrative reviews, articles not published in English, commentaries, studies that described sports injury prevention strategies but did not assess their effectiveness, studies that did not assess musculoskeletal injuries, and studies that did not assess sports-related injuries. The most relevant results were extracted and summarized. Levels of evidence were determined per the Oxford Centre for Evidence-Based Medicine, and methodological quality was assessed using the AMSTAR-2 (A MeaSurement Tool to Assess systematic Reviews, revised version).
Results:
A total of 507 articles were retrieved, and 129 were included. Articles pertaining to all injuries were divided into 9 topics: sports and exercise in general (n = 20), soccer (n = 13), ice hockey (n = 1), dance (n = 1), volleyball (n = 1), basketball (n = 1), tackle collision sports (n = 1), climbing (n = 1), and youth athletes (n = 4). Articles on injuries by anatomic site were divided into 11 topics: general knee (n = 8), anterior cruciate ligament (n = 34), ankle (n = 14), hamstring (n = 11), lower extremity (n = 10), foot (n = 6), groin (n = 2), shoulder (n = 1), wrist (n = 2), and elbow (n = 1). Of the 129 studies, 45.7% were ranked as evidence level 1, and 55.0% were evidence level 2. Based on the AMSTAR-2, 58.9% of the reviews reported a priori review methods, 96.1% performed a comprehensive literature search, 47.3% thoroughly described excluded articles, 79.1% assessed risk of bias for individual studies, 48.8% reported a valid method for statistical combination of data (ie, meta-analysis), 45.0% examined the effect of risk of bias on pooled study results, and 19.4% examined the risk for publication bias.
Conclusion:
This comprehensive review provides sports medicine providers with a single source of the most up-to-date publications in the literature on sports injury prevention.
In the United States, approximately 4.3 million nonfatal sports or recreation-related injuries are seen annually in the emergency department. 81 The highest rates of sports injuries for both boys and girls occur in adolescents aged 10 to 14 years, which is likely due to increased participation in sports among this age group. 81 The lower extremity is most commonly injured during sports participation; however, the incidence of injury to specific body parts varies by sport. 81,185,257 Owing to the influx of participants in sports and the subsequent injuries they sustain, research on sports injury prevention strategies is rapidly growing. 129 Injury prevention is important for reducing long-term health consequences, such as disability, and minimizing the economic burden of treatment. 2
Injury prevention strategies typically focus on modifiable risk factors, such as rules, equipment, and physical fitness, and prevention strategies may be tailored to a specific sport or injury. 2 Exercise training involves learning proper exercise techniques, such as understanding the limits of range of motion of each joint and avoiding joint positions that place the anatomic structures of the joint at risk for injury. 40 Exercise training usually involves some combination of strength, proprioceptive, balance, and neuromuscular training that is important for improving athletic performance and preventing injuries. 30,107,127
The purpose of this comprehensive review was to quantify the number of systematic reviews and meta-analyses that have examined the effectiveness of sports injury prevention programs on reducing musculoskeletal injuries, evaluate the quality of each systematic review, identify the primary studies included in each review, and provide a succinct summary of this vast body of literature for easy reference. We hypothesized that the largest number of articles would (1) pertain to sports injury prevention in general (as opposed to prevention strategies for specific sports) and (2) focus on preventing knee injuries that are common in sports.
Methods
We performed a literature search in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 151 using PubMed, CINAHL, EMBASE, and the Cochrane databases to identify articles published in English between inception of these databases and August 31, 2020. Additional articles were found by hand searching the reference lists of included articles. The search terms were (“prevention” or “prevention programs”) AND (“sports injury” OR “musculoskeletal injury”) AND (“systematic review” or “meta-analysis”). We included systematic reviews and meta-analyses that evaluated the effectiveness of sports injury prevention programs on reducing musculoskeletal injuries. We excluded published abstracts, narrative reviews, articles not published in English, commentaries, studies that described sports injury prevention strategies but did not assess the effectiveness of these strategies, studies that did not assess musculoskeletal injuries, and studies that did not assess sports-related injuries.
The results of the entire literature search were entered into a single database, and duplicates were removed via electronic search and double-checked manually. Two of the authors (S.D.S. and M.A.K.) independently screened the results of the literature search, and 3 authors (S.D.S., J.W.K., and A.V.V.) reviewed studies that met inclusion in more detail and summarized the germane results. The articles that met inclusion criteria were summarized by 2 major topics: (1) all injuries and (2) injuries by anatomic site. Articles pertaining to all injuries were further subdivided into 9 topics: sports and exercise in general, soccer, ice hockey, dance, volleyball, basketball, tackle collision sports, climbing, and youth athletes. Articles pertaining to injuries by anatomic site were subdivided into 11 topics: general knee, anterior cruciate ligament (ACL), ankle, hamstring, lower extremity, foot, groin, shoulder, wrist, shin, and elbow. We determined the level of evidence for each systematic review according to the definitions set forth by the Oxford Centre for Evidence-Based Medicine. 88 Methodological quality was assessed using the AMSTAR-2 (A MeaSurement Tool to Assess systematic Reviews, revised version). 205 The list of 129 articles was divided in half among 4 authors (S.D.S., M.A.K., J.W.K., and A.V.V.) for AMSTAR-2 assessment, and thus each study was assessed independently by 2 authors (S.D.S. and M.A.K.). Last, we tallied the number of overlapping primary studies between systematic reviews within a particular topic.
Results
Figure 1 presents the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart illustrating the literature search process. The literature search identified 507 unique articles, and of these, 129 met the inclusion criteria. Table 1 illustrates the number of included articles by topic. The majority of “all injury” articles pertained to sports and exercise in general (15.5%) and soccer (10.1%). Most of the “injuries by anatomic site” articles pertained to ACL (26.4%), ankle (10.9%), and hamstring (8.5%) injuries. Three of the 129 included articles covered >1 anatomic site. The level of evidence and the AMSTAR-2 results are shown in Table S1 (available as Supplemental Material). A total of 59 (45.7%) of the included systematic reviews were ranked as evidence level 1, and 71 (55.0%) were level 2. Based on the AMSTAR-2, 76 (58.9%) reviews reported a priori review methods, 124 (96.1%) performed a comprehensive literature search, 61 (47.3%) thoroughly described excluded articles, 102 (79.1%) assessed risk of bias for individual studies, 63 (48.8%) reported a valid method for statistical combination of data (ie, meta-analysis), 58 (45.0%) examined the effect of risk of bias on pooled study results, and 25 (19.4%) examined the risk for publication bias.
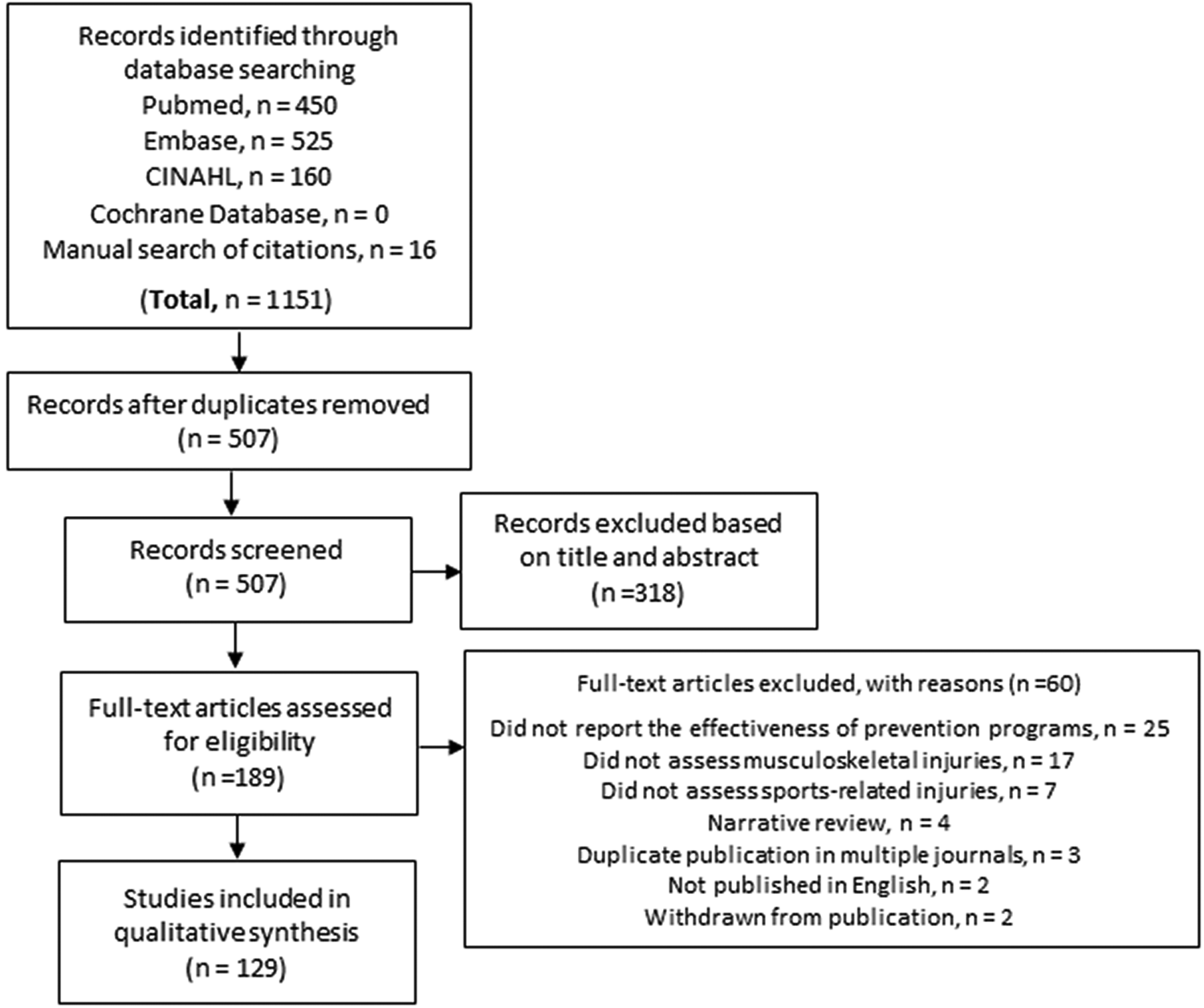
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart.
Number of Included Articles by Topic
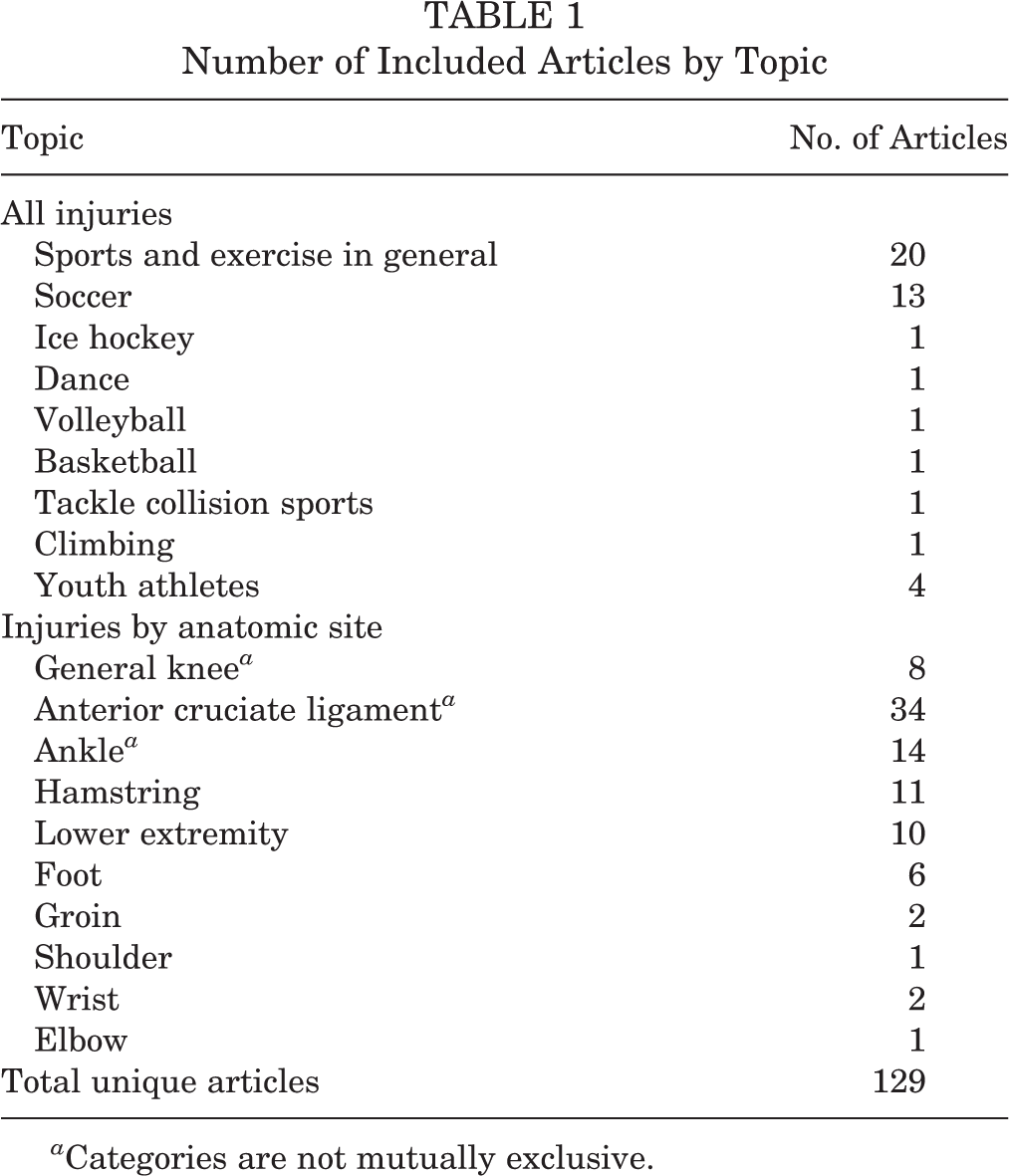
a Categories are not mutually exclusive.
All Injuries
A total of 43 studies pertaining to prevention of all injuries were identified and are summarized by topic here. Tables S2 to S4 and Figures S1 to S3 (available as Supplemental Material) illustrate the overlapping primary studies between included systematic reviews.
Sports and Exercise in General
A number of overlapping systematic reviews ‡ have examined the effectiveness of various injury prevention strategies for sports and exercise in general. Salam et al 194 pooled data from 24 studies and found that sports injury prevention interventions were effective in that interventions decreased the incidence of (1) injuries in general (relative risk [RR], 0.66; 95% confidence interval [CI], 0.53-0.82), (2) injuries per hour of exposure (RR, 0.63; 95% CI, 0.47-0.86), and (3) injuries per number of exposures (RR, 0.79; 95% CI, 0.70-0.88); however, the results of their study were not stratified by type of intervention. Two meta-analyses by Lauersen et al 127,128 found that strength training was effective for reducing the risk of sports injuries, and 1 of these studies 128 also found that proprioception training (RR, 0.55; 95% CI, 0.35-0.87) and a combination of exercises (RR, 0.66; 95% CI, 0.52-0.83) were effective at reducing sports injuries. Smyth et al 214 found moderate evidence demonstrating the effectiveness of exercise and psychological interventions for reducing injuries in pre-elite athletes competing in the Olympics or professional sports, but evidence was lacking with respect to the effectiveness of equipment and nutrition-related interventions. Two systematic reviews 1,129 found that the use of insoles, external joint supports, and multi-intervention or sport-specific training programs were effective for injury prevention. Of note, several overlapping systematic reviews have found no or minimal evidence regarding the effectiveness of stretching, § warm-up exercises, 1,69 or prevention videos 1,129 for injury prevention. Two systematic reviews 30,107 demonstrated that balance training was favorable for reducing overall injuries (RR, 0.49; 95% CI, 0.13-1.80) and defined the optimal balance training program for injury prevention as lasting for 8 weeks and including two 45-minute training sessions per week. Three overlapping systematic reviews 77,131,239 found that psychological interventions, including cognitive behavioral therapy and stress management—based interventions, were effective at reducing sports injuries. Ernst and Posadzki 60 found conflicting results regarding the effectiveness of chiropractic interventions for preventing sports injuries in their review of 6 studies. To summarize, there are multiple systematic reviews and meta-analyses demonstrating that injury prevention programs are effective, with strength, proprioception, balance, and psychological programs being specifically beneficial.
Soccer
Four overlapping systematic reviews 43,64,182,243 found mixed results for exercise-based prevention programs in soccer players, and all of these reviews were poor quality and at high risk for bias. Based on their review of 18 studies, Kirkendall et al 123 concluded that a structured warm-up program can be effective at reducing soccer injuries by one-third. Based on their review of 13 studies, Slimani et al 211 found that psychological-based interventions were effective at reducing injury rates in soccer players. Seven overlapping systematic reviews and meta-analyses 4,6,21,79,119,192,238 examined the effectiveness of 2 soccer injury prevention programs developed by the Federation Internationale de Football Association (FIFA). The FIFA 11 and FIFA 11+ programs combine training in both technique and balance along with neuromuscular training exercises including strengthening and plyometrics with the goal of eliminating injuries. Al Attar et al 4 examined the combined effects of FIFA 11 and FIFA 11+ and found that overall injuries were reduced by 34% (RR, 0.66; 95% CI, 0.60 to 0.73) and lower limb injuries were reduced by 29% (RR, 0.71; 95% CI, 0.63 to 0.81). Gomes Neto et al 79 observed that FIFA 11 was associated with reduced injury risk (RR, 0.69; 95% CI, 0.49 to 0.98) and improvement in both dynamic balance (weighted mean difference, 2.68; 95% CI, 0.44 to 4.92) and agility (standardized mean difference, –0.36; 95% CI, –0.70 to 0.02) compared with controls. Two systematic reviews 21,192 demonstrated that FIFA 11+ resulted in (1) 30% to 70% fewer injuries and (2) significant improvement in many features of motor and neuromuscular performance. Two systematic reviews 6,238 directly compared FIFA 11 and FIFA 11+ and found that FIFA 11+ was associated with a greater reduction in injuries. In their review of 33 articles, Kilic et al 119 concluded that the FIFA 11+ program and the Nordic Hamstring Exercise (NHE) program were most effective for reducing musculoskeletal injuries in adult soccer players, while FIFA 11, balance board, the Prevent Injury and Enhance Performance program, a groin program, and balance board training were not effective injury prevention programs. To summarize, the FIFA 11+ program has been shown to reduce injuries and improve neuromuscular performance in soccer.
Ice Hockey
Cusimano et al 45 identified 13 studies that examined rule changes intended to minimize aggression (eg, restriction of body-checking) during ice hockey, of which 9 studies demonstrated a decrease in penalties ranging from 1.2 to 5.9 per game and in injury rates by 3- to 12-fold.
Dance
Hincapie et al 103 reviewed 2 cohort studies and concluded that there was weak evidence for the effectiveness of injury prevention programs in dancers.
Volleyball
Kilic et al 120 found evidence from 3 studies that (1) a resistance training program, (2) a program aimed at reducing anterior knee pain, and (3) balance board training were effective at reducing musculoskeletal injuries in volleyball players.
Basketball
Based on their systematic review of 4 studies, Kilic et al 121 concluded that each of the following programs was successful at reducing musculoskeletal injuries in basketball players: (1) a jump-landing technique intervention during warm-up, (2) a multistation proprioceptive exercise program, (3) a wobble board and sport-specific balance training program during warm-up, and (4) the FIFA 11+ program.
Tackle Collision Sports
Sewry et al 202 identified 7 studies that demonstrated that exercise-based intervention programs were successful at reducing injuries in tackle collision sports (ie, rugby union or league and American, Australian, and Gaelic football).
Climbing
Based on their systematic review of 19 studies, Woollings et al 260 found that both taping and weight training reduced injury rates in sport climbing and bouldering. However, the authors did not find any support for stretching, yoga, using instructors, regulating equipment usage, taking supplements, heating hands before climbing, and corticosteroid injections as injury prevention measures for sport climbing.
Youth Athletes
Several overlapping systematic reviews 2,37,189,217 have examined the effectiveness of various sports injury prevention strategies in youth (ie, adolescents or teenagers aged <20 years). Soomro et al 217 pooled data from 10 studies and found a 40% reduction (injury rate ratio, 0.60; 95% CI, 0.48-0.75) in injuries for multifaceted injury prevention programs (ie, a combination of warm-up, neuromuscular strength, and proprioception training) in adolescent team sports. Abernethy and Bleakley 2 reviewed 12 studies and found preseason conditioning, functional training, education, balance, and sport-specific skills to be moderately effective at preventing adolescent sports injuries. However, the effectiveness of protective equipment (eg, knee pads and knee braces) was inconclusive and requires further research. Rossler et al 189 conducted a meta-analysis of 21 randomized controlled trials (RCTs) and found that prevention programs geared toward both specific injuries and all injuries in children and adolescents were effective. Furthermore, the authors concluded that prevention programs including jumping or plyometric exercises were more effective than programs that did not include these types of exercises. Carder et al 37 systematically reviewed 6 studies and found that 43% of youth athletes specialized in a single sport and these athletes were at greater risk for injury compared with youth athletes that sampled a variety of sports (RR, 1.37; 95% CI, 1.19-1.57).
Injuries by Anatomic Site
A total of 86 studies pertaining to prevention of injuries by anatomic site were identified and are summarized by topic here. Tables S5 to S10 and Figures S4 to S9 (available as Supplemental Material) illustrate the overlapping primary studies between included systematic reviews.
General Knee Injuries
Grimm et al 85 found insufficient evidence regarding the effectiveness of knee injury prevention programs in athletes based on their review of 10 RCTs; however, the authors did not distinguish among different types of injury prevention programs. Thacker et al 236 found limited evidence supporting the effectiveness of neuromuscular training and conditioning programs for reducing knee injuries. On the other hand, 3 overlapping systematic reviews 51,84,99 have demonstrated that neuromuscular training programs reduced knee injuries by 27%. Ter Stege et al 233 systematically reviewed 35 studies and found that neuromuscular injury prevention programs were effective at reducing several risk factors (ie, knee valgus moments, knee flexion angles, hamstring activation profiles, and vertical ground-reaction forces) that are associated with knee injuries in team ball sports. Three overlapping systematic reviews 179,195,236 have found that wearing a knee brace is not effective at reducing knee injuries in athletes.
ACL Injuries
All Athletes. Two systematic reviews 7,163 concluded that the available evidence was too weak to make any conclusions about the effectiveness of ACL injury prevention programs in general; however, several more recent systematic reviews 85,152,232 have found ACL injury prevention programs to be effective. Grindstaff et al 86 conducted a meta-analysis of 5 studies and estimated that 89 individuals (95% CI, 66-136) would need to participate in an injury prevention program to prevent 1 ACL injury per season. Furthermore, these authors concluded that the most important components of an ACL injury prevention program were plyometrics, strengthening, flexibility, agility, and feedback. Padua and Marshall 168 found moderate evidence to support the use of ACL injury prevention programs, which incorporate proprioception/balance or plyometric/agility training in athletes; however, no studies directly compared the effectiveness of multifaceted versus single exercise programs. Arundale et al 15 found substantial evidence supporting the use of exercise-based prevention programs for reducing knee and ACL injuries in athletes. Several overlapping systematic reviews ∥ have found that neuromuscular training programs were effective at reducing ACL injuries by 51% to 62%, and 1 meta-analysis 193 found that neuromuscular training was more effective at reducing ACL injuries in male versus female patients. Sugimoto et al 224 found that participant age (ie, training was more effective for younger athletes compared with adults), dosage of training, exercise variations, and verbal feedback were the most effective components of a neuromuscular training program. Inclusion of at least 1 of these 4 components in a training program reduced the risk of ACL injury by 18%, and if all 4 components were incorporated into the program, the risk was reduced by as much as 73%.
Benjaminse et al 26 concluded that when teaching motor learning, giving athletes an external focus of attention (eg, soft landing) was more effective for increasing performance and decreasing the risk of ACL injuries compared with an internal locus of attention (eg, knee flexion). Furthermore, Armitano et al 12 found that motor learning programs using augmented information improved risk factors that were associated with ACL injuries. Neilson et al 157 concluded that using augmented feedback with jump landing training was an effective way to reduce 2 of the major risk factors for ACL injury: maximum knee flexion angle and vertical ground-reaction force.
Female Athletes
Several overlapping systematic reviews ¶ have focused on ACL injury prevention in female athletes. Two systematic reviews 161,223 have demonstrated the effectiveness of ACL injury prevention programs in female athletes; however, there were insufficient data to determine which specific program was most effective for reducing ACL injuries. On the other hand, 3 overlapping systematic reviews concluded that plyometrics, 38,254 strengthening, 227,254 and neuromuscular exercises 254 were the most effective components for injury prevention in female athletes. Moreover, Noyes and Barber Westin 160 found that both the Sportsmetrics and the Prevent Injury and Enhance Performance programs successfully reduced ACL injuries in female athletes; however, the Sportsmetrics program is very time-intensive (ie, 1-2 hours of training for 3 d/wk) and may compromise compliance. Based on their meta-analysis of 14 studies, Sugimoto et al 226 found that the most effective ACL injury prevention programs in female athletes were those (1) of longer duration (>20 minutes vs <20 minutes), (2) done more frequently (multiple times versus once per week), and (3) with a higher training volume. Myer et al 155 found that neuromuscular training was most effective at reducing ACL injuries in female athletes aged ≤18 years compared with >18 years (odds ratio [OR], 0.28; 95% CI, 0.18-0.42). Based on their meta-analysis of 18 studies, Petushek et al 176 found that interventions that targeted female athletes in middle school and high school (OR, 0.38; 95% CI, 0.24-0.60) reduced the odds of ACL injury more so than interventions targeting college or professional female athletes (OR, 0.65; 95% CI, 0.48-0.89). Only 1 meta-analysis 225 examined compliance with neuromuscular training in female athletes and found that high compliance was associated with a greater reduction in ACL injuries compared with low compliance (risk reduction ratio, 0.27; 95% CI, 0.07-0.80). Pfile and Curioz 178 concluded that both mixed leadership (RR reduction, 48.2%; 95% CI, 22%-65%) and coach-led (RR reduction, 58.4%; 95% CI, 40%-71%) injury prevention programs were successful at reducing ACL injuries in female athletes; however, the available evidence was low to moderate quality.
Ankle Injuries
Eight overlapping systematic reviews # have found the use of external supports, such as ankle bracing and taping, to be effective at reducing ankle injuries. Barelds et al 20 conducted a meta-analysis of 6 studies and found that ankle bracing was effective for both primary (RR, 0.53; 95% CI, 0.32-0.88) and secondary (RR, 0.37; 95% CI, 0.24-0.58) prevention of acute ankle injuries; however, the available evidence was low quality. Two systematic reviews 25,50 found that external supports reduced ankle injuries by 62% to 64%; however, another review 49 found that external supports were only effective in athletes with a history of ankle injuries.
Several overlapping systematic reviews have found evidence supporting the effectiveness of neuromuscular training, 34,35,250 proprioception and balance training, 25,34,48,143,197 and exercise interventions 50,83 for preventing ankle injuries. Four overlapping systematic reviews 25,48,116,197 found that proprioception or balance training reduced ankle injuries by 31% to 46%, and these training programs primarily consisted of single-leg stance challenges, wobble/balance board exercises, and sport-specific agility drills. Furthermore, Schiftan et al 197 found that proprioceptive training (ie, balance exercise with or without balance/wobble board or ankle disc for at least 8 weeks) was effective at reducing ankle sprains in athletes with (RR, 0.64; 95% CI, 0.51-0.81) and without (RR, 0.57; 95% CI, 0.34-0.97) a history of ankle sprain. Doherty et al 50 conducted a meta-analysis of 23 studies and found that exercise interventions reduced recurrent ankle sprains by 41% (pooled OR, 0.59; 95% CI, 0.51-0.68), and the most effective intervention was ankle disc or balance/wobble-board training for a minimum of 4 to 6 weeks. Grimm et al 83 conducted a meta-analysis of 10 RCTs and found that an exercise protocol focused on stretching, strength training, balance, and coordination reduced the risk of ankle injuries by 40% (RR, 0.60; 95% CI, 0.40-0.92). In summary, several systematic reviews and meta-analyses have found external supports and balance and proprioceptive training to be effective in preventing ankle injuries.
Hamstring Injuries
Hibbert et al 101 systematically reviewed 7 studies in 2008 and concluded that hamstring lowers, isokinetic strengthening, and other strengthening were effective at reducing hamstring strains; however, the included studies were deemed low quality and none of the studies examined eccentric strengthening in isolation. Two systematic reviews, 1 by Prior et al 183 in 2009 and the other by Monajati et al 152 in 2016, found low-level evidence suggesting that hamstring injury prevention programs in general may be effective at reducing hamstring injuries. Goldman and Jones 78 systematically reviewed 7 RCTs in 2010 and concluded that there was insufficient evidence regarding the effectiveness of strengthening, manual therapy, proprioception, and warm-ups/cool-downs for preventing hamstring injuries. Based on 2 systematic reviews 145,186 published in 2016 and 2013, respectively, there is inconclusive evidence regarding the effectiveness of stretching on reducing hamstring injuries. The NHE was designed to increase eccentric hamstring strength in soccer players, and 4 overlapping systematic reviews 5,80,203,245 conducted between 2015 and 2019 found that the NHE (used in isolation or combined with other interventions) reduced hamstring injuries by 49% to 65%. Two overlapping systematic reviews 80,203 published in 2015 and 2017, respectively, found that using a YoYo flywheel ergometer for eccentric hamstring strengthening was effective at reducing hamstring injuries in soccer players. In 2019, Vatovec et al 247 conducted a meta-analysis of 17 studies and found that hamstring injuries were reduced by 51% after exercise interventions and by 50% after neuromuscular interventions.
Lower Extremity Injuries
Several overlapping systematic reviews have demonstrated that exercise programs 33,261 and neuromuscular training programs 58,95,221,231 were effective at reducing lower extremity injuries. Emery et al 58 found that neuromuscular training reduced lower extremity injuries by 36% in youth athletes (injury risk reduction, 0.64; 95% CI, 0.49-0.84). Based on their meta-analysis of 10 RCTs, Taylor et al 231 found that neuromuscular training with or without lace-up ankle braces reduced the odds of lower extremity injuries in basketball players by 31% (OR, 0.69; 95% CI, 0.57-0.85). Steib et al 221 concluded that neuromuscular training was effective at reducing lower extremity injury risk in youth athletes, and the optimal regimen was 10- to 15-minute sessions 2 to 3 times a week. Herman et al 95 reviewed 9 studies and concluded that to be effective at reducing lower limb injuries, neuromuscular warm-up strategies should be completed for at least 3 months and should incorporate stretching, strengthening and balance exercises, sports-specific agility drills, and landing techniques. Yeung and Yeung 261 concluded that there was strong evidence suggesting that the incidence of lower extremity soft tissue running injuries can be reduced by decreasing running frequency, duration, and distance; however, the optimum training load could not be determined. There is weak or insufficient evidence regarding the effectiveness of (1) eccentric exercise, proprioception, and balance exercise for reducing lower extremity injuries in soccer players 137 ; (2) exercise programs for prevention of lower limb injuries in Australian football players 10 ; and (3) lower limb injury prevention programs in high school athletes. 138 Thacker et al 234 systematically reviewed 9 studies and found that using shock-absorbent orthotic inserts and a preseason conditioning regimen focused on lower extremity strength, agility, and flexibility may reduce the occurrence of shin splints in young male athletes.
Foot Injuries
Several overlapping systematic reviews found low to moderate evidence that shock-absorbing insoles may be effective at preventing stress fractures in an active military population; however, no other types of interventions (eg, reducing training volume and intensity) have been effective at reducing stress fractures, and no studies have been done in the general population. 29,76,114,187,204 A meta-analysis of 11 studies found that foot orthoses reduced the risk of stress fractures by 41% (RR, 0.59; 95% CI, 0.45-0.76). 29 Peters et al 173 found limited evidence supporting the use of balance training, shoe adaptations, and hormone replacement therapy in active postmenopausal women for reducing Achilles tendinopathy, and there was no evidence to support stretching for reducing Achilles tendinopathy.
Groin Injuries
Two nonoverlapping systematic reviews 39,62 found limited evidence to support the use of hip adductor and abdominal strengthening exercises for groin injury prevention.
Shoulder Injuries
Asker et al 16 identified only 1 study 9 that examined prevention of shoulder injuries in overhead sports and found no statistically significant effects of a strength and conditioning regimen on shoulder injuries in Norwegian handball players.
Wrist Injuries
Two overlapping systematic reviews 122,191 found that the risk for wrist injury, wrist fracture, and wrist sprain was reduced by 54% to 83% in snowboarders with the use of wrist guards.
Elbow Injuries
Deal et al 47 found that injury prevention programs were effective at reducing elbow injuries in baseball players.
Discussion
This comprehensive review provides a thorough and concise summary of all systematic reviews and meta-analyses on the topic of sports injury prevention in general and for specific sports and injury types. The majority of “all injury” articles pertained to sports and exercise in general (15.5%) and soccer (10.2%). Most of the “injuries by anatomic site” articles pertained to ACL (26.4%), ankle (10.9%), and hamstring (8.5%) injuries. In line with our hypothesis, we found that most injury prevention systematic reviews pertained to sports injuries in general (as opposed to specific sports) and focused on prevention of knee injuries (both in general and specifically on the ACL). To our knowledge, this is the first comprehensive review of the systematic reviews and meta-analyses published on sports injury prevention.
Injury prevention programs are effective and can reduce injuries by at least 40% in both youth and adults. 194,217 Strength training, proprioception, balance, and psychological programs have all been shown to be beneficial, while stretching has not. Much of the research on preventing sport-related injuries in general has focused on specific sports, 45,103,120,121,202,260 primarily soccer. ** †† There is substantial evidence supporting the FIFA 11+ program for preventing soccer-related injuries; however, the systematic reviews on this topic include many overlapping studies. 4,6,21,79,119,192,238 There is limited low-quality research demonstrating that other exercise and psychological-based interventions are effective at reducing soccer-related injuries. 43,64,123,182,211,243 Several systematic reviews have found injury prevention programs tailored toward hockey, 45 volleyball, 120 basketball, 121 tackle collision sports, 202 and sport climbing and bouldering 260 to be effective at reducing musculoskeletal injuries in general.
Evidence regarding the effectiveness of neuromuscular training for preventing knee injuries in general has been contradictory, 51,84,99,236 and there is currently no systematic review evidence to support wearing a knee brace for injury prevention. 7,179,236 However, there is moderate evidence to support exercise and neuromuscular training programs for ACL injury prevention, 7,85,152,163,232 and the most effective components of these programs included plyometrics, strengthening, flexibility, agility, and feedback. 86 A number of systematic reviews have focused on ACL injury prevention in female athletes†† and found that plyometrics, 38,254 strengthening, 227,254 and neuromuscular training 254 were most effective in this cohort. ACL injury prevention programs were most effective in female athletes aged <18 years 155 and among those who were highly compliant with the programs. 225 The most effective ACL injury prevention programs in female athletes were those lasting at least 20 minutes per session, with multiple sessions per week and at a high training volume. 226 It should be noted that the ACL injury prevention literature may be skewed toward female athletes since most of the studies evaluated female athletes only or included more female athletes than male athletes. There is substantial evidence supporting the use of ankle bracing and taping, which can reduce ankle injuries by at least 60%. ‡‡ Neuromuscular, 34,35,250 balance, 25,34,48,143,197 and exercise training 50,83 have also been shown to be effective for reducing ankle injuries. Exercise and neuromuscular training have been demonstrated to be effective at reducing hamstring injuries by 50% 247 ; however, the effectiveness of strengthening remains uncertain, 78,80,101,203 and there is no evidence to support stretching 145,186 for hamstring injury prevention. Lower extremity injuries can be reduced by exercise 33,261 and neuromuscular training 58,95,221,231 programs, and the risk for stress fractures may be reduced by foot orthoses. 29,76,114,187,204 Wrist guards have been shown to reduce wrist injuries by 54% to 83% in snow boarders. 122,191 There is limited evidence available to be able to make any conclusions regarding groin, 39,62 shoulder, 16 and elbow 47 injuries and shin splints. 234
There are several limitations of this study. There were a number of overlapping studies between systematic reviews and meta-analyses, which may have resulted in more weight being placed on the strength of evidence for certain topics than was truly warranted. Only 19.4% of the included reviews assessed publication bias, and 47.3% thoroughly described exclusion criteria. Thus, selection and/or publication biases may have affected the results of individual reviews. Also, only 48.8% of systematic reviews pooled their data for analysis. The remaining 50.2% did not pool data mainly because of considerable heterogeneity among included studies. Finally, this review was limited to a qualitative summary of the literature since there was too much heterogeneity between studies to warrant any pooled data analyses. However, strengths of this study include performing a thorough literature search in accordance with PRISMA and performing a thorough review of study quality and risk for bias using the AMSTAR-2.
Conclusion
This comprehensive review provides sports medicine providers and other interested parties with a single source of the most up-to-date published literature focused on the effectiveness of sports injury prevention and organizes the literature by anatomic site and general injury patterns.
Supplemental Material for this article is available at http://journals.sagepub.com/doi/suppl/10.1177/23259671211035776.
Supplemental Material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671211035776 - A Comprehensive Summary of Systematic Reviews on Sports Injury Prevention Strategies
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671211035776 for A Comprehensive Summary of Systematic Reviews on Sports Injury Prevention Strategies by Samuel D. Stephenson, Joseph W. Kocan, Amrit V. Vinod, Melissa A. Kluczynski and Leslie J. Bisson in Orthopaedic Journal of Sports Medicine
Footnotes
Notes
Final revision submitted April 5, 2021; accepted May 3, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: Departmental research funding was received from the Ralph C. Wilson Jr Foundation. L.J.B. has received research support from Arthrex, royalties from Zimmer Biomet, and hospitality payments from Prodigy Surgical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.