
Abstract
Background:
A “double-pulley” dual-row technique had been applied for arthroscopic fixation of large bony Bankart lesion in which the fragment has a wide base.
Purpose:
To investigate clinical outcomes and glenoid healing after arthroscopic fixation of bony Bankart lesion using the double-pulley dual-row technique.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 25 patients were included in this retrospective study. The American Shoulder and Elbow Surgeons (ASES) score, pain visual analog scale (VAS) score, and range of motion of the affected shoulder were assessed. Radiographs and computed tomography (CT) scans (preoperatively, immediately after surgery, and at 1 year postoperatively) were performed to evaluate arthritic changes (Samilson-Prieto classification) and glenoid size. The intraobserver reliability of the CT measurements was analyzed.
Results:
At a mean follow-up of 3.4 years, the mean ASES and VAS scores were 94.87 ± 5.02 and 0.48 ± 0.59, respectively. Active forward elevation, external rotation with the arm at the side, and internal rotation were 165.80° ± 11.70°, 33.20° ± 8.02°, and T9 (range, T6-S1), respectively. No patient reported a history of redislocation or instability. The intraobserver reliability of the CT measurements was moderate to excellent. The mean preoperative size of the bony fragment was measured as 23.4% ± 7.8% of the glenoid articular surface. The quality of the reduction was judged to be excellent in 13 (52%) cases, good in 8 (32%), and fair in 4 (16%). The mean immediate postoperative glenoid size was 96.8% ± 4.3%, and bone union was found in all cases. There were no significant differences between reconstructed and immediate postoperative glenoid size or between preoperative and final Samilson-Prieto grades.
Conclusion:
The arthroscopic double-pulley method was a reliable technique for the fixation of large bony Bankart lesions with a wide base. Satisfactory results can be expected regarding the restoration of the glenoid morphology and stability of the shoulder. High healing rate and good shoulder function can be achieved. No radiological evidence of cartilage damage caused by suture abrasion was found at 2- to 5-year follow-up.
Bony Bankart lesions are commonly observed in patients with anterior shoulder dislocation and are defined as a detachment of the anteroinferior labrum associated with a glenoid rim fracture. 2,4,5 The incidence of bony Bankart lesion ranges from 4% to 70%. 11 The arthroscopic management of acute and chronic bony Bankart lesions has been proven to be effective over the past 20 years. 6,7,10,11 However, the stability of fixation and the healing of the bony fragment is still a concern.
A “double-pulley” dual-row technique has been described for the arthroscopic fixation of bony Bankart lesion in which the fragment has a wide base. 15 This technique distributes the stress evenly over a large surface area to achieve better healing and biomechanical stability. The purpose of this study was to investigate clinical outcomes and glenoid healing after arthroscopic fixation of bony Bankart lesions using this double-pulley technique. We hypothesized that this technique would provide good clinical outcomes and a high healing rate.
Methods
Patient Selection
Institutional review board approval was received for this retrospective study. The indications for the double-pulley technique were (1) chronic (surgery performed more than 3 weeks after injury) bony Bankart lesion with recurrent anterior dislocation or acute (surgery within 3 weeks after injury) case with bony fragment displacement >5 mm; and (2) a bulky bony Bankart fragment with a maximum mediolateral width of the base of >5 mm.
The inclusion criteria were patients who (1) were diagnosed with traumatic anterior shoulder dislocation or instability with a bony Bankart lesion; (2) had undergone arthroscopic treatment using the double-pulley technique; (3) were in possession of complete sets of preoperative, immediate postoperative, and postoperative 1-year computed tomography (CT) scans with 3-dimensional (3D) reconstruction; and (4) were available for clinical follow-up for at least 2 years. The exclusion criteria were as follows: (1) multidirectional shoulder instability; (2) previous surgery on the affected shoulder; or (3) fixation in addition to the suture anchors (screw, button, etc).
Surgical Technique
All surgeries were performed by a single senior surgeon (C.J.) using the technique described by Zhang and Jiang. 15 The patient was placed in the standard lateral decubitus position. After a diagnostic arthroscopy through a standard posterior portal, a high anterosuperior portal was established. The attachment of the inferior glenohumeral ligament (IGHL) complex to the fragment was preserved.
A thorough release and debridement was performed if the fragment was healed medially on the glenoid neck in chronic cases. Two 3.5-mm double-loaded suture anchors (M1: distal anchor, M2: proximal anchor [Twinfix, Smith & Nephew] in Figure 1) with 2 high-performance nonabsorbable sutures were placed through the normal glenoid cortex just medial to the glenoid fracture line (Figure 1A). All 8 limbs of the suture strands were passed through the soft tissues medial to the bony fragment. The sutures were evenly distributed through the IGHL complex. Three 2.8-mm single-loaded suture anchors (L1: distal anchor, L2: middle anchor, and L3: proximal anchor [Twinfix, Smith & Nephew] in Figure 1) were placed at the anterior articular margin of the native glenoid. Fixation was finished after all suture loops were tied together (Figure 1, B and C; Figure 2). There were 6 loops running across the bony fragment horizontally (2 M1-L1, 2 M2-L3, M1-L2, and M2-L2) and 1 loop running over the medial base of the fragment vertically (M1-M2). Concomitant rotator cuff tears (RCTs) were repaired with suture anchors. When the fracture fragment was comminuted, the fragments were held together with the labral tissue, and the fragments could still be reduced and fixed with this technique.

The double-pulley dual-row technique for arthroscopic fixation of bony Bankart lesion. (A) The dual-row anchors. (B) One suture strand from the lateral anchor (L1) was tied extracorporeally to a strand from the medial anchor (M1) with a static surgeon’s knot. The other 2 suture strands were pulled (arrows), thereby delivering this extracorporeal knot into the joint over the bony fragment. (C) Reduction and fixation of the bony Bankart fragment. Image reproduced from Zhang and Jiang. 15 M2 = medial proximal anchor; L2 = lateral middle anchor; L3 = lateral proximal anchor.

Intra-articular view of a left shoulder from an anterosuperior viewing portal. (A) The bony Bankart fragment. (B) Reduction and fixation of the fragment. Image reproduced from Zhang and Jiang. 15
Postoperative Rehabilitation
A sling was used for 6 weeks after surgery. Passive range of motion (ROM) exercises were started at postoperative 4 weeks under the supervision of a physical therapist. Terminal stretching exercises were allowed at 3 months postoperatively. Overhead or contact sports activities were not allowed until 1 year after surgery, when full ROM was restored and no apprehension was detected.
Follow-up
The patients were evaluated at 6 weeks, 3 months, 6 months, 1 year, and every year thereafter until the final follow-up. The American Shoulder and Elbow Surgeons (ASES) score, and pain visual analog scale (VAS) score, and ROM of the affected shoulder were assessed by the same independent surgeon who performed the preoperative evaluation. Preoperative ASES and VAS scores were not available.
Radiographic Evaluations
All radiographic evaluations were performed by a single author (S.G.) who was not involved in the surgical procedures. Radiographs and CT scans were performed preoperatively, immediately after surgery, and at 1 year postoperatively. Additional radiographs were taken every year thereafter until the final follow-up, and possible arthritic changes were evaluated according to the Samilson-Prieto classification. 12
Using the method described by Sugaya et al, 13 an en face view of the glenoid was obtained with the humeral head eliminated on the preoperative and postoperative CT scans. On the preoperative CT scan, 3 parameters (the sizes of the residual glenoid, bony fragment, and bony defect of the glenoid) were measured using a graphics program (Photoshop CS; Adobe). The sizes of the residual glenoid and the bony fragment were calculated as the percentage of the surface area of a projected outer-fitting circle based on the inferior portion of each glenoid (Figure 3). The size of the bony defect was calculated using the following equation: Bony defect size = 1 – Residual glenoid size.

The size of the residual glenoid was calculated as the percentage of the glenoid fossa in the en face view using the following equation: G/A × 100%, where A = the area of the outer-fitting circle based on the inferior part of the glenoid contour from the 3-o’clock to 9-o’clock position, and G = the area of the residual glenoid. The size of the bony fragment was calculated as F/A × 100%, where F = the area of the displayed osseous fragment.
On the immediate postoperative CT scan, the reduction quality was graded using the method described by Sugaya et al 14 : (1) excellent, sufficient superior and lateral repositioning without a step-off between the fragment and the glenoid face; (2) good, sufficient superior repositioning but insufficient lateral repositioning, with a step-off apparent between the fragment and the glenoid face; (3) fair, insufficient superior and lateral repositioning with an apparent step-off; or (4) poor, the fragment was not repositioned and remained in the original preoperative location (Figure 4). The postoperative glenoid size was calculated as the percentage of the surface area of the postoperative glenoid to the area of the outer-fitting circle (Figure 5).

Three-dimensional computed tomography (left) and axial magnetic resonance imaging scans (right) showing reduction quality according to the Sugaya classification 14 : (A) excellent, (B) good, and (C) fair.

The size of the postoperative reconstructed glenoid was calculated as the percentage of the glenoid fossa in the en face view using the following equation: G*/A × 100%, where A = the area of the outer-fitting circle based on the inferior part of the glenoid contour from the 3-o’clock to 9-o’clock position, and G* = the area of the postoperative glenoid.
On the postoperative 1-year follow-up CT scan, healing of the bony fragment was checked in the axial view and in 3D. Bone healing was defined as no gap or prominent demarcation line identified between the graft and the native glenoid on consecutive axial CT scans. The size of the reconstructed glenoid was calculated as the percentage of the surface area of the reconstructed glenoid to the area of the outer fitting circle.
The sizes of the fragment and the glenoid were measured by a single observer (S.G.) 3 times at 2-month intervals. The data were recorded as the mean value of the 3 measurements.
Statistical Analysis
All the data were analyzed using SPSS 16.0 software (IBM). Continuous variables were reported as means ± SDs. Intraobserver reliability was analyzed by calculating the intraclass correlation coefficient, in which >0.75 indicated excellent reliability, 0.40 to 0.75 moderate reliability, and <0.40 poor reliability. A paired t test was used to compare the glenoid size at different time points. For all analyses, P < .05 was considered significant.
Results
Characteristics
From February 2015 to February 2018, a total of 121 patients with a bony Bankart lesion were treated surgically in our department; of these, the arthroscopic double-pulley technique had been performed in 34 patients. The majority of the other cases with bony Bankart lesions had small bone fragments and were treated with an arthroscopic Bankart repair. Nine patients were excluded from this study because of loss to follow-up (n = 1) or incomplete CT imaging (n = 8). None of the 8 patients with incomplete imaging data reported a history of recurrent instability or dislocation. Thus, 25 patients (n = 7 women; n = 18 men) were eligible for this study. The mean age was 44 years (range, 14-74 years). Four (16%) patients had RCTs. In 19 (76%) patients, the arthroscopic repair was performed within 3 weeks after injury. The other 6 patients underwent surgery at times ranging from 2 to 11 months after the initial trauma.
Clinical Outcomes
The mean follow-up period was 3.4 years (range, 2-5 years). At the final evaluation, the mean ASES score was 94.87 ± 5.02, and the mean VAS pain score was 0.48 ± 0.59. The mean active forward elevation, external rotation beside the body, and internal rotation were 165.80° ± 11.70°, 33.20° ± 8.02°, and T9 (range, T6-S1), respectively. The results had no significant differences compared with the contralateral side: forward elevation, 169.6° ± 7.9° (P = .077); external rotation, 36° ± 8° (P = .143); and internal rotation, T9 (range, T6-L3) (P = .059). No patient reported a history of redislocation or instability after surgery. The apprehension and relocation test was negative in all cases. There were no complications.
Radiographic Evaluations
The detailed patient and CT imaging data are listed in Table 1. The intraobserver reliability of the CT measurements is described in Table 2, with results suggesting moderate to excellent reliability.
Demographic Data and Results of CT Scan a

a Dashes indicate calculating the mean was not applicable. ASES, American Shoulder and Elbow Surgeons; CT, computed tomography; F, female; M, male; N, no; Preop, preoperative; Postop, postoperative; Y, yes.
Intraobserver Reliability of CT Measurements a
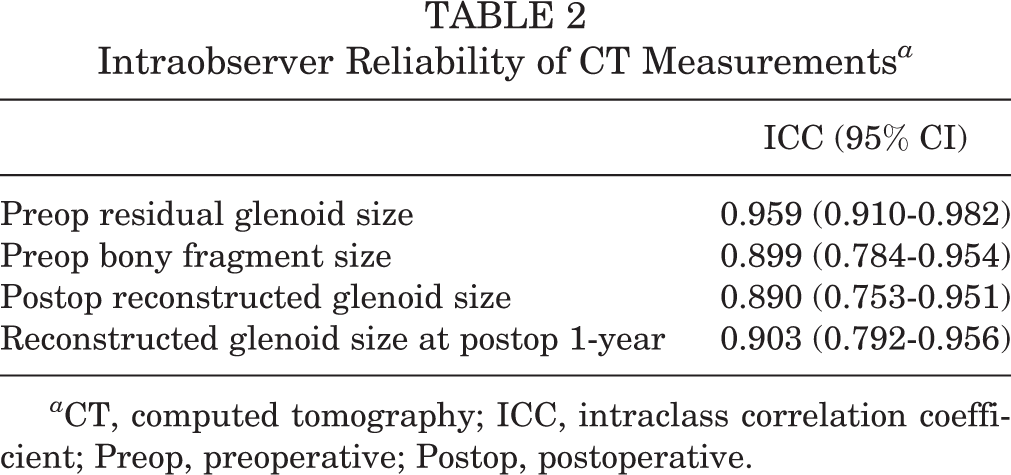
a CT, computed tomography; ICC, intraclass correlation coefficient; Preop, preoperative; Postop, postoperative.
Preoperatively, the mean surface area of the residual glenoid and the bony fragment was 72.5% ± 9.3% and 23.4% ± 7.8%, respectively. The defect size was 27.5% ± 9.3%. On the CT scan immediately after surgery, the quality of the reduction was graded as excellent in 13 (52%) cases, good in 8 (32%), and fair in 4 (16%). The mean immediate postoperative glenoid size was 96.8% ± 4.3%.
Bone union of the fragment was found in all cases on the 1-year postoperative CT scan. The mean reconstructed glenoid size was 96.3% ± 5.2%, which was not significantly different compared with the immediate postoperative glenoid size (P = .584).
Glenohumeral arthrosis grades according to Samilson-Prieto classification are presented in Table 3. Only 1 patient showed progression of arthrosis. There were no significant differences in results between preoperative assessment and final follow-up (P = .317).
Samilson-Prieto Classification Preoperatively and at Last Follow-up a

a Data are presented as n (%).
Discussion
The most important finding of the present study support was that the “double-pulley” technique was able to achieve satisfactory reduction and restore the glenoid morphology, leading to good postoperative shoulder function and glenoid healing.
According to previous studies, 2,3 glenoid bone loss is associated with a higher risk of surgical failure after arthroscopic soft tissue repair. Therefore, a bony reconstruction procedure is recommended, especially in cases with bone loss >20% to 25% of the inferior glenoid diameter. Although many arthroscopic techniques have been reported, the presence of a bulky fragment is still a big challenge for an all-arthroscopic approach. The single-row suture anchor technique might not provide sufficient contact area and compression between the fracture fragment and the glenoid bone bed. A dual-row fixation can effectively avoid this disadvantage. The double-pulley suture-tying technique was originally reported by Arrigoni et al 1 and Koo et al. 9 This technique creates double-mattress sutures that compress the fragment against its bone bed without overtensioning and restores better bony anatomy of the anterior glenoid rim with stable and nontilting fixation, which may improve healing. 15 Although the present study included cases with larger fragment size (23.4%) compared with that of previous studies (Sugaya et al 14 : 9.2%; Kitayama et al 8 : 4.7%) using the single-row technique, all cases obtained osseous union with a nearly normal or slightly hypertrophic glenoid as well.
In the present study, the included cases had bulky bony fragments with a mean size of 23.4% of the inferior glenoid surface area. In 84% (21/25) of the cases, the reduction quality was graded as “good” or “excellent,” and in 16% (4/25) it was graded as “fair.” The whole system is a horizontally paralleled double-loop system strengthened by a vertical loop. The stress of each loop is equally distributed between the 2 strands overlying the fragment. Because the sutures are free to slide through the eyelets, an incidental tension increase (or decrease) at one point can easily be adjusted by changing the tension on the secondly tied 2 suture strands before knot tying. The secondly tied 2 suture strands of an established loop are tied together as a static knot to finalize the fixation of the fragment, thus avoiding the risk of overtensioning the fragment (Figure 6). In most patients, the CT scan at 1-year follow-up showed little displacement of the fragment compared with the immediate postoperative CT scan. The bone union of fragments was confirmed in all cases. These promising results indicate that the double-pulley technique can provide stable fixation and restore glenoid morphology.

Reduction of fragments in a right shoulder. Images from: (A) preoperative and (B) immediately postoperative. (a) Axial view. (b) En face view of the glenoid. (c) Lateral view of the glenoid.
Unlike coracoid transfer surgery (Bristow-Latarjet), marked resorption of the reconstructed glenoid was not found in cases in this study. There was no significant difference between the mean immediate postoperative glenoid size and the mean reconstructed glenoid size at 1 year postoperatively. Also, the morphology of the reconstructed glenoid had little alteration during that period in most of the cases. In some of the nonanatomically reconstructed cases, remodeling rather than resorption was identified at the final follow-up. Eight of the 25 patients had a larger glenoid size at the final follow-up compared with immediately postoperative. Kitayama et al 8 also reported this phenomenon.
Although all knots were tied outside the edge of the glenoid rim to avoid abrasion and potential cartilage damage, sutures on top of the fragment articular surface can still be a potential risk for cartilage abrasion, which may lead to arthritis. In our case series, there was no significant difference in Samilson-Prieto grade from preoperatively to final follow-up (P = .317). Progression according to Samilson-Prieto grade was confirmed in just one 63-year-old female patient who had undergone concomitant rotator cuff repair, with a 2-year follow-up time. Considering the same issue also exists in arthroscopic soft tissue Bankart repair, there was no evidence that the double-pulley technique adds more risks from this perspective, despite the fact that the sutures overlay a much greater length of the articular cartilage.
There are some limitations to this study. First, the number of patients included was relatively small, and the rate of loss to follow-up was considerable (9/34). However, all included cases had complete clinical follow-up and 3 complete sets of CT images, and no recurrent instability was seen in the patients who were excluded because of missing CT scans. Second, although the glenoid and the fragment size was recorded as the mean value of 3 measurements to avoid bias, the unavoidable error in measurement cannot be totally eradicated. Third, for the evaluation of cartilage damage and arthritis thereafter, 2 to 5 years of follow-up time was relatively short and might not be reliable. Thus, further long-term follow-up evaluations are warranted. Finally, this was a level 4 case review study, and comparisons with other techniques were not performed.
Conclusion
The arthroscopic double-pulley technique was found to be a reliable technique for the fixation of large bony Bankart lesions with a wide base. Satisfactory results can be expected regarding the restoration of the glenoid morphology and stability of the shoulder. High healing rate and good shoulder function can be achieved. No radiographic evidence of the cartilage damage caused by the suture abrasion was found in this case series at 2- to 5-year follow-up.
Footnotes
Final revision submitted February 13, 2021; accepted March 2, 2021.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Beijing Jishuitan Hospital (IRB 201706-07).