
Abstract
Background:
During notchplasty in anterior cruciate ligament (ACL) reconstruction, bone is excised from the lateral and roof area of the notch to widen the intercondylar space and avoid notch-graft impingement in extension. There are concerns that bone regrowth of the area will cause narrowing and increase the risk of complications.
Purpose:
To determine the possibility of late narrowing of the notch after notchplasty using computed tomography (CT) analysis.
Study Design:
Case series; Level of evidence, 4.
Methods:
Measurements were performed on CT scans (axial and sagittal planes with knee in extension) in patients who had undergone single-bundle anatomic ACL reconstruction using hamstring graft. Two axial image levels were used: at the anterior outlet and the anterior one-eighth level of the notch. The maximum notch height and width, the notch width at one-third and two-thirds of the preoperative notch midwidth height, the maximum condylar width, and the surface area of the lateral half of the notch were measured preoperatively and at 1 week and 2 years postoperatively.
Results:
Included were 20 consecutive patients (mean ± standard deviation age, 28 ± 7.3 years; follow-up, 24.2 ± 3.3 months). At the anterior notch outlet, the maximum notch width increased by 1.9 ± 1.7 mm at 1 week postoperatively and narrowed by 0.3 ± 1.1 mm at the final follow-up, while the maximum notch height increased by 1.7 ± 1.9 mm and narrowed by 0.8 ± 1.8 mm, respectively. At one-eighth of the roof length, the maximum notch width increased by 1.1 ± 1.7 mm at 1 week postoperatively and narrowed by 0.1 ± 1.1 mm at the final follow-up, and the maximum notch height increased by 1.2 ± 1.5 mm and narrowed by 0.5 ± 1.5 mm, respectively. All differences were statistically significant when comparing the pre- to the immediate postoperative measurements, and they were nonsignificant when comparing the immediate postoperative to the final follow-up measurements. The same applied for the ratio of maximum notch width to maximum condylar width, indicating no postoperative narrowing of the notch.
Conclusion:
Notch size-shape after a 2-mm notchplasty did not change significantly in stable knees during the first 2 years after anatomic ACL reconstruction. Surgeons should consider performing this adjuvant technique when there is notch-graft impingement during surgery.
Keywords
Notchplasty is an adjuvant surgical procedure to anterior cruciate ligament (ACL) reconstruction consisting of widening and reshaping the intercondylar notch to avoid notch-graft impingement in extension. 3,5,25 It consists of bone/cartilage excision from the lateral and roof area of the intercondylar notch, aiming to widen the intercondylar space. It has been utilized as an adjuvant procedure mostly in the transtibial/isometric ACL reconstruction techniques, but many surgeons still perform notchplasty in the transportal/anatomic techniques. 12,15,18,25,28 Other advantages of notchplasty include better visualization within the notch as well as an increase of the cross-sectional area of the regenerated ACL, providing more space for graft healing and enhancing the healing process. 14,15,19 However, there are concerns related to postoperative blood loss in the early phase, to knee biomechanics distortion, and even more to bone regrowth and narrowing of the notch after notchplasty, although these aspects are still debated. 15,25
Postoperative narrowing after notchplasty could place a previously safe graft at risk for impingement and failure because of the close anatomic relationship of the ACL and the lateral wall of the notch. Little is known about the long-term consequences of this procedure. Furthermore, conflicting reports about regrowth of bone leave surgeons with doubts about decision making. 25 The aim of the current study was to evaluate the regrowth of bone in the intercondylar notch 2 years after primary anatomic ACL reconstruction combined with a 2-mm notchplasty using computed tomography (CT).
Methods
This was a prospective observational study, approved by the institution’s research board. All patients provided informed consent for participation in the study.
Patients
Consecutive patients undergoing ACL reconstruction between January and June 2017 were evaluated in this study. Included patients were aged >18 years, with complete ACL tear confirmed with magnetic resonance imaging (MRI), receiving a single-bundle anatomic reconstruction with autologous quadruple hamstring graft with a diameter ≥8 mm. Exclusion criteria were knee osteoarthritic changes, history of ipsilateral or contralateral fractures or major injuries in weightbearing bones of the lower limbs, and concomitant additional ligament tears.
Surgical Technique
A standard arthroscopic examination was performed to confirm the ACL tear. Then, graft harvesting was performed via an oblique 3-cm incision at the upper border of the pes anserinus. The gracilis and semitendinosus tendons were harvested using a tendon stripper and then looped over a strong suture, creating 4 strands that were sutured together using a whipstitch, and pretensioning was applied for 10 minutes. If the quadruple graft diameter was <8 mm, the patient was excluded from the study. ACL femoral and tibial remnants were debrided, and the posterior edge of the lateral intercondylar wall and tibial footprint were detected. A 2-mm notchplasty of the roof and the lateral femoral wall was performed using either a small osteotome or a motorized bur and a radiofrequency diathermy. The approximate thickness of bone excision was determined by fitting a 2-mm-edge probe, and using the bur, a round, reshaped notch was achieved (Figures 1 and 2).

Layout showing the bone excision (gray area) from the roof and lateral area of the notch, aiming at a round, reshaped notch.

Arthroscopic views of notchplasty from the anterolateral portal. (A) The approximate thickness of 2-mm bone excision was determined by fitting a 3-mm-edge probe and (B) marked using a 4.5-mm tip radiofrequency diathermy in an oblique way. (C) A final view of the 2-mm notchplasty before proceeding with the next steps of the anterior cruciate ligament reconstruction.
The tunnels of the femur and the tibia were drilled and prepared using a dilator, according to the anatomic single-bundle technique, matched with the graft diameter. The graft was fixed using a button system on the femoral side and an interference bioabsorbable screw (Arthrex Inc) on the tibial side. The risk of notch-graft impingement was finally checked arthroscopically by moving the knee periodically from flexion to extension.
Postoperatively, no brace was used. Gradually increasing partial weightbearing and free range of motion was allowed during the first 4 weeks before full weightbearing without crutches was allowed. Closed-chain exercises were emphasized for the first 6 weeks, rowing and biking exercises were permitted after 6 weeks, and running was permitted after 3 months. Contact sports were allowed after the first 6 months.
Methods of Assessment
The dimensions, size, and shape of the intercondylar notch of all patients were measured using CT scan analysis. All knees were evaluated preoperatively, at 1 week postoperatively, and at the 2-year follow-up using a Siemens SOMATOM Definition AS CT scanner at 200 kVp, 110 mAs, and a 14-cm field of view. The patients lay supine, and the knees were examined using 0.6-mm spiral cuts. Thereafter, the measurements were performed using Syngo CT 2010B software (Siemens AG). All dimensions were measured at 2 different image levels in the axial plane: at the anterior axial outlet as well as the level of the anterior one-eighth of the entire notch roof (Blumensaat line) (Figure 3). Those anterior axial levels were selected, as this is the area most likely to cause notch-graft impingement, as previously described. 19
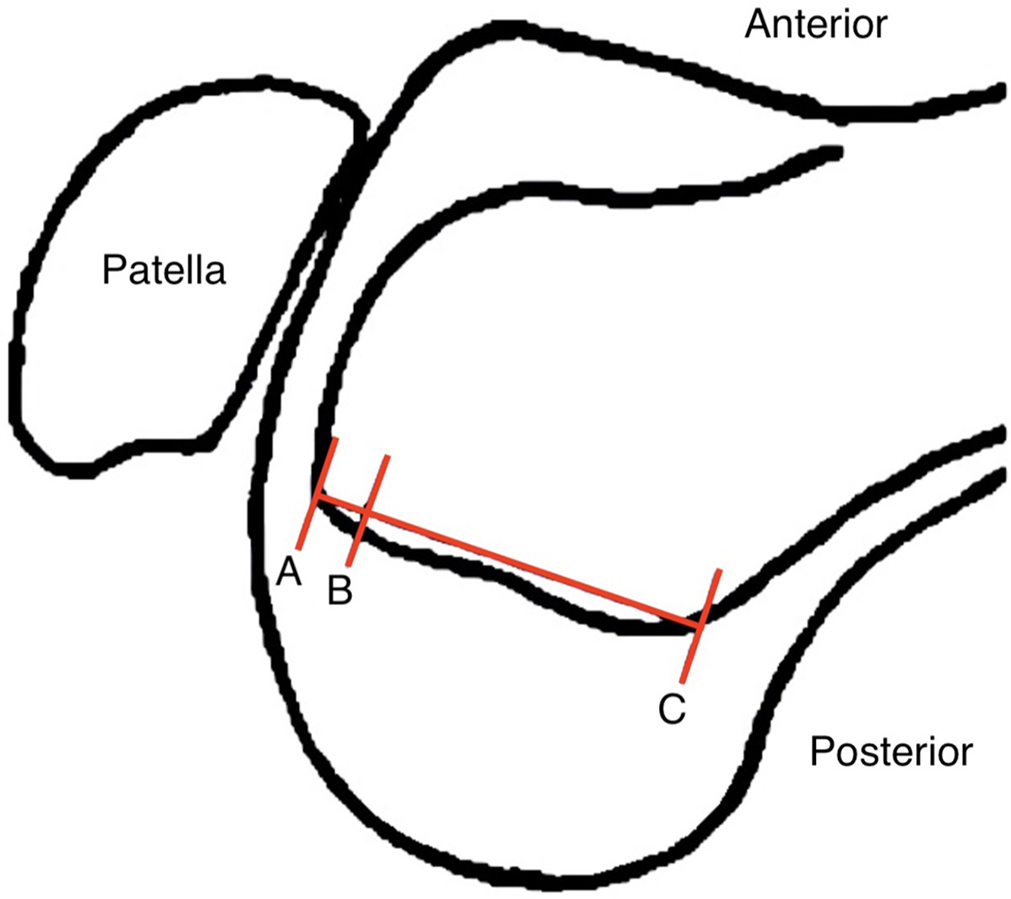
Sagittal layout showing the 2 axial levels at the anterior outlet (A) and anterior one-eighth of the notch (B), determined using the length of the Blumensaat line (AC).
The following measurements in both axial levels were taken:

Layouts showing the (A) maximum notch width and height, (B) notch width at one-third and two-thirds of the preoperative notch midwidth height, and (C) area of the lateral half of the notch (gray area, B) and the maximum condylar width (C). L, lateral; M, medial.
More specifically, the midwidth notch height as measured on the preoperative CT scan was used as a reference to standardize the notch measurements, using a consistent distance from the medial wall, which was not affected by the notchplasty postoperatively. A ratio was calculated of the maximum notch to condylar width, as used in previous studies. 19 The radiologist assessing the CT scans (I.T.) was blinded to the patients’ baseline characteristics.
Statistical Analysis
The preliminary sample size calculation for paired samples suggested that, with a 5% probability of a type 1 error and a power of 80%, a sample size of 20 patients was necessary to detect a difference of an average of 2 mm in the intercondylar notch measurements, which would indicate regrowth of bone after an average 2-mm notchplasty. The calculation was performed using PS: Power and Sample Size Calculation software Version 3 (Vanderbilt University). 6
All comparisons were performed using the paired-samples t test with the Bonferroni correction for multiple group comparisons. The potential correlation between the time period from injury to surgery and the amount of bone regrowth was evaluated using the Pearson correlation coefficient. Statistical Package for Social Sciences (SPSS) software Version 24 (IBM Corp) was used.
Results
A total of 20 patients (18 men and 2 women; 11 right and 9 left knees) were included in the study. The mean ± standard deviation age of the patients was 28 ± 7.3 years, and the mean follow-up was 24.2 ± 3.3 months. The mean time from injury to surgery was 8.6 ± 2 weeks. All ACL reconstructions were uneventful, with no intraoperative concern of notch-graft impingement, and all patients were available for final follow-up without any clinical failures of the grafts. The mean quadruple graft diameter was 8.7 ± 0.5 mm.
At the anterior notch outlet, the maximum notch width increased by 1.9 ± 1.7 mm after surgery and narrowed by 0.3 ± 1.1 mm at final follow-up, while the maximum notch height increased by 1.7 ± 1.9 mm and narrowed by 0.8 ± 1.8 mm, respectively (Figures 5 and 6). All differences were statistically significant when comparing the pre- with the immediate postoperative measurements and nonsignificant when comparing the immediately postoperative with the final follow-up measurements. The same was applied for the maximum notch width to maximum condylar width ratio, which indicated no narrowing of the notch after the operation. The measurements at the anterior outlet of the notch are presented in Table 1.

(A) Preoperative, (B) immediate postoperative, and (C) follow-up computed tomography images showing the increase of the notch maximum width after notchplasty and no bone regrowth with preservation of the width at the final follow-up. L, lateral; M, medial.

(A) Preoperative, (B) immediate postoperative, and (C) follow-up computed tomography images showing the excision of the lateral notch wall osteophyte after notchplasty and no bone regrowth with preservation of the width at the final follow-up. L, lateral; M, medial.
Measurements at the Anterior Outlet of the Notch a
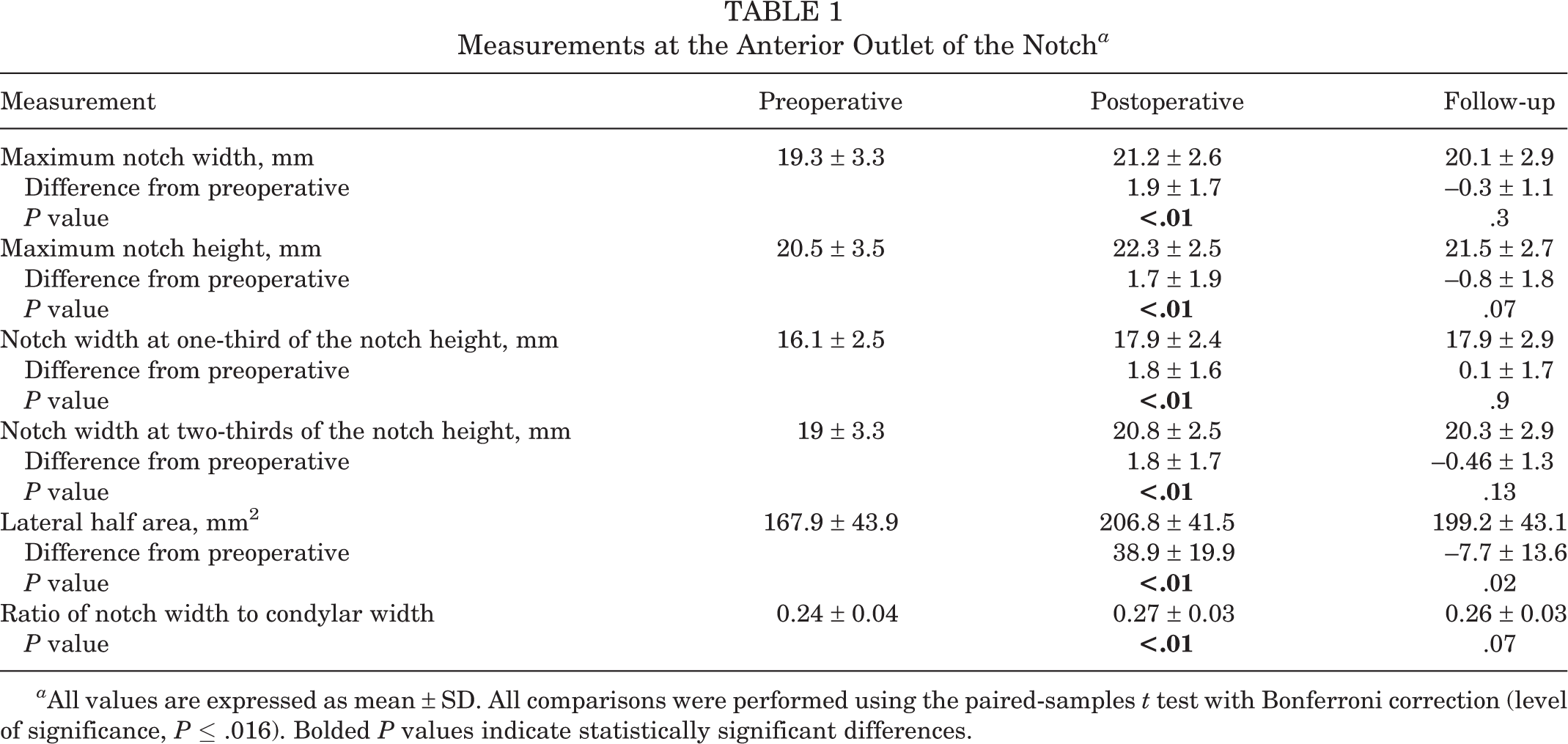
a All values are expressed as mean ± SD. All comparisons were performed using the paired-samples t test with Bonferroni correction (level of significance, P ≤ .016). Bolded P values indicate statistically significant differences.
At one-eighth of the roof length, the maximum notch width increased by 1.1 ± 1.7 mm after surgery and narrowed by 0.1 ± 1.1 mm at the final follow-up, while the maximum notch height increased by 1.2 ± 1.5 mm and narrowed by 0.5 ± 1.5 mm, respectively. Similarly, all differences, including the maximum notch width to maximum condylar width ratio, were statistically significant after the notchplasty and nonsignificant when compared with the final follow-up, indicating no narrowing of the notch. The measurements at one-eighth of the roof length are presented in Table 2.
Measurements at One-Eighth of the Notch Depth From Anterior Outlet to Posterior Notch a

a All values are expressed as mean ± SD. All comparisons were performed using the paired-samples t test with Bonferroni correction (level of significance, P ≤ .016). Bolded P values indicate statistically significant differences.
Of note, the amount of bone regrowth was not significantly correlated with the time period from injury to surgery (P = .2, Pearson correlation).
Discussion
Notchplasty is an adjuvant surgical procedure to ACL reconstruction consisting of widening and reshaping the intercondylar notch to avoid the notch-graft impingement in extension; however, the long-term consequences are still unknown. 20,25 The current study showed that bone regrowth in CT imaging 2 years after notchplasty, measured at both the anterior outlet and the anterior one-eighth of the notch roof length, was not significant. The width and height measurements, as well as the lateral area of the notch, increased significantly when comparing the pre- with the immediate postoperative measurements and did not display significant narrowing when comparing the immediate postoperative measurements with the final 2-year follow-up.
Interpretation in the Context of the Literature
Several radiographic methods have been used to evaluate the intercondylar notch dimensions. The choice of CT imaging in the current study was based on the research of Dahlstedt et al, 5 who showed high accuracy comparing CT and actual intercondylar notch measurements, as well as Anderson et al, 2 who reported low error rates when comparing CT with plain radiography.
The reports about bone regrowth after notchplasty are conflicting. The results of the current study agree with those of Mann et al, 19 who reported no regrowth of the intercondylar notch dimensions on CT scans between 1 week and 1 year postoperatively in 10 patients undergoing ACL reconstruction with notchplasty. However, their study was limited by the small number of patients and a short follow-up period. Dahlstedt et al 5 also observed no bone regrowth 4 years postoperatively on the CT scans of 12 stable knees; however, bone regrowth was noted in failed reconstructions.
May et al 22 evaluated patients after 6 months using MRI and reported a thin layer of cortical bone regrowth. Furthermore, Bents et al 3 observed signs of graft impingement on MRI scans 6 months after ACL reconstruction with notchplasty in 8 of the 36 patients studied, and they hypothesized that this was caused by immature bone growth. Ahn et al 1 evaluated 208 patients arthroscopically after a mean of 21.2 months and reported some degree of notch reformation in 40% of patients, although the clinical results were good and it may be justified by soft tissue coverage. Regarding animal studies, Fitch et al 8 reported bone refilling of the notch after 6 months, and LaPrade et al 16 observed osteophyte formation in dogs. However, they performed a more aggressive notchplasty ranging from 4 to 8 mm. Aggressive intercondylar notchplasty may cause notch regrowth, as well as articular cartilage histopathologic changes, consistent with early degenerative arthrosis. 9,16,19 Therefore, minimal 2-mm notchplasty should be performed only if deemed necessary after having tested the graft clearance intraoperatively.
Several studies in the literature have raised concerns about biomechanical alteration in knee kinematics after notchplasty. 13,20 A large lateral notchplasty may displace the femoral insertion to an abnormally lateral position, which may lead to abnormal knee kinematics and increased graft forces during knee flexion. 9,11 Markolf et al 21 reported that graft forces increased proportionally after 2- and 4-mm notchplasties, respectively, in a biomechanical model. Recently, Mao et al 20 studied small (3-mm) or large (6-mm) notchplasties and concluded that anterior tibial translation increases and graft forces decrease during low knee flexion angles. However, when assessing a 2-mm notchplasty in anatomic double-bundle ACL reconstruction, anterior stability was improved, and there were no harmful effects on patellofemoral joint findings. 15 Therefore, to prevent these potential problems, including the possibility of graft tightening, a limited notchplasty up to 2 mm would still prevent impingement but would not change the origin site of the ACL. In the current study, after a very small notchplasty, the total bone and cartilage loss after excision and a minimal regeneration did not exceed 1.6 mm of the lateral wall and 0.9 mm of the notch roof 2 years postoperatively.
Interpretation of the Results and Clinical Implications
Notchplasty as an adjuvant procedure should not be performed routinely. It should be considered only when the position of the femoral and tibial tunnels, the degree of notch stenosis, and the thickness of the graft may indicate notch-graft impingement. Moreover, notchplasty is most useful in the treatment of arthrofibrosis and in the presence of bone spurs in the context of osteoarthritis in both primary and revision surgery. 7,17,23,25,26 It has been mostly utilized in the transtibial/isometric ACL reconstruction techniques, but many surgeons still perform notchplasty in the transportal/anatomic techniques. 12,15,18,25,28
Surgeons may avoid notchplasty by following principles such as avoiding the double-bundle technique in cases of a narrow notch (<12 mm), 25 choosing the right graft size to avoid notch-graft mismatch and decrease the incidence of cyclops lesions, 10 and placing the tibial tunnel as medially as possible for the anteromedial bundle in the double-bundle technique 27 while respecting the graft-free zone on the tibial footprint. 28 Moreover, if adequate visualization within the notch cannot be achieved, an additional portal can replace notchplasty for better viewing. 24
This study showed that if graft impingement still occurs after all principles were followed, notchplasty with bone excision of an average of 2 mm from the roof and lateral wall of the notch is a safe procedure. Bone regrowth in the notch was minimal (between 0.1 and 0.8 mm) at 2 years postoperatively, and this is in agreement with the results of May et al 22 about a thin layer of cortical bone regrowth. The thin layer of cortical bone probably covers the space that does not come in contact with the graft during the knee motion, and it is highly unlikely to impinge and result in graft failure.
The use of a radiofrequency diathermy after the notchplasty reduces blood loss and decreases the incidence of arthrofibrosis and loss of extension. 25 It may also inhibit osteoblast proliferation and bone refilling in the area. Camillieri et al 4 evaluated the results of notchplasty using a radiofrequency instrument or a motorized shaver in a randomized trial, concluding that postoperative bleeding was significantly higher in patients who received notchplasty using a motorized shaver, although no difference in the range of motion was observed 1 month postoperatively.
Limitations
The present study has several limitations. It represents a patient cohort with a large male to female ratio, and no control group was recruited. Additionally, clinical outcomes were not reported, as this information does not concern the research question of the current study. Although the outcome assessors were blinded to the patients’ characteristics, blinding to the sequence of postoperative CT scans was not possible. Moreover, the results of the current study cannot be adopted in the case of a more aggressive notchplasty because it may cause notch regrowth and biomechanical alterations, as mentioned. Furthermore, although the tibial tunnel was placed at the same location, unavoidable small variations may have affected the regrowth of bone. Late narrowing of the notch may also occur as a result of soft tissue coverage; however, this is unlikely to cause graft failure and was not assessed in the current study. Finally, although not very likely, bone regrowth may occur beyond the 2-year follow-up period of this study.
Conclusion
Notch size-shape, after notchplasty of an average of 2 mm, did not change significantly in stable knees during the first 2 years after anatomic ACL reconstruction. Surgeons should consider performing this adjuvant technique when there is notch-graft impingement intraoperatively.
Footnotes
Final revision submitted March 1, 2021; accepted March 19, 2021.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the 424 Military General Hospital (study No. 190515/424MGH).