
Abstract
Background:
Trochlear dysplasia (TD) is a recognized condition that can become a risk factor for patellofemoral instability. A modified Albee osteotomy procedure using a trapezoidal-shaped wedge to elevate the lateral wall of the trochlea can be used with the goal of preventing further dislocation. However, outcomes studies are lacking, and scores on patient-reported outcome measures (PROMs) are largely unknown.
Purpose/Hypothesis:
The purpose of this study was to identify PROM scores for the Kujala Anterior Knee Pain Scale (AKPS), International Knee Documentation Committee (IKDC), Activity Rating System (ARS), and 100-point pain visual analog scale (VAS) for patients having undergone the modified Albee osteotomy. The hypothesis was that patients will have acceptable pain and function at mid- to long-term follow-up.
Study Design:
Case series; Level of evidence, 4.
Methods:
From 1999 to 2017, a total of 46 consecutive patients (49 knees) underwent a modified Albee procedure by a single surgeon at a single health care system. These 46 patients were contacted and asked to complete the AKPS, IKDC, ARS, and pain VAS. Additional demographic information was obtained via chart review. Frequencies and rates for categorical variables and means and standard deviations for continuous variables of the demographics and PROM scores were calculated.
Results:
PROM scores were obtained in 28 (30 knees; 61%) of the 46 patients. At minimum follow-up of 82 months, the mean scores were 78.5 ± 18.2 for AKPS, 61.2 ± 11.4 for IKDC, 5.2 ± 5.3 for ARS, and 24.4 ± 28.7 for VAS pain. Notably, only 1 of the 28 patients reported a patellofemoral dislocation since surgery, and this was an isolated incident without further instability.
Conclusion:
A modified Albee trochlear osteotomy can be a successful adjunctive procedure to prevent recurrent patellar dislocations in patients with mild TD. However, owing to the loss of one-third of patient follow-up scores and the absence of baseline function scores in this study, the procedure deserves further investigation as a way to address a particularly difficult dilemma for a select subset of patients with patellofemoral instability.
Keywords
Acute dislocation of the patella is a relatively common knee injury, comprising 2% to 3% of all knee injuries in children and adults. 6,8,14,20 In addition to patella alta and skeletal immaturity, trochlear dysplasia (TD) is recognized as a significant risk factor for the development of recurrent patellar dislocation. 2,3,13,19,21 Femoral TD is characterized as the abnormal depth and shape of the trochlear groove. 18 The condition affects less than 2% of the general population; however, some studies have shown that 85% of individuals with a history of recurrent patellofemoral dislocations have TD. 5,16 Several radiographic findings exist for TD, with perhaps the most prominent being the crossing sign. The crossing sign, first described by Dejour et al, 5 is viewed on a true lateral radiograph and is seen as the line representing the floor of the trochlear groove crossing the anterior femoral condyles. Dejour et al found this sign in only 3% of patients without a history of dislocation but in 96% of patients with a history of dislocation. Dejour et al have classified TD. 15 Initially, it was developed from the lateral plain radiograph and based on the crossing sign and the presence or absence of a supratrochlear spur. Subsequently, Dejour et al developed a system with 4 subtypes based on axial computed tomography images.
In 1915, Albee 1 described a trochlear osteotomy to be used for the treatment for habitual patellar dislocations. His osteotomy elevated the lateral wall of the femoral trochlea by inserting a 1-cm cortical-cancellous bone graft. In so doing, there was an obligatory fracture of the articular surface of the lateral femoral condyle. Furthermore, Kuroda et al 12 demonstrated that elevations of this magnitude significantly increased patellofemoral contact pressures.
These developments, combined with the knowledge that the normal depth of the trochlear groove is 6 mm, led to one aspect of our modification of the Albee procedure. The height of our bone wedge is only 6 to 8 mm, as shown in Figure 1A. Second, in an effort to avoid the articular surface fracture, we designed a trapezoidal wedge with a proximal height of 6 to 8 mm and 2 mm distally (Figure 1, B and C). This would create an adequate lateral buttress at entry and recreate the slope of the lateral wall of the trochlea. As Farahmand et al 7 demonstrated, once the patella has engaged within the trochlea, the slope of the lateral wall of the trochlea becomes the primary restraint to lateral translation of the patella.
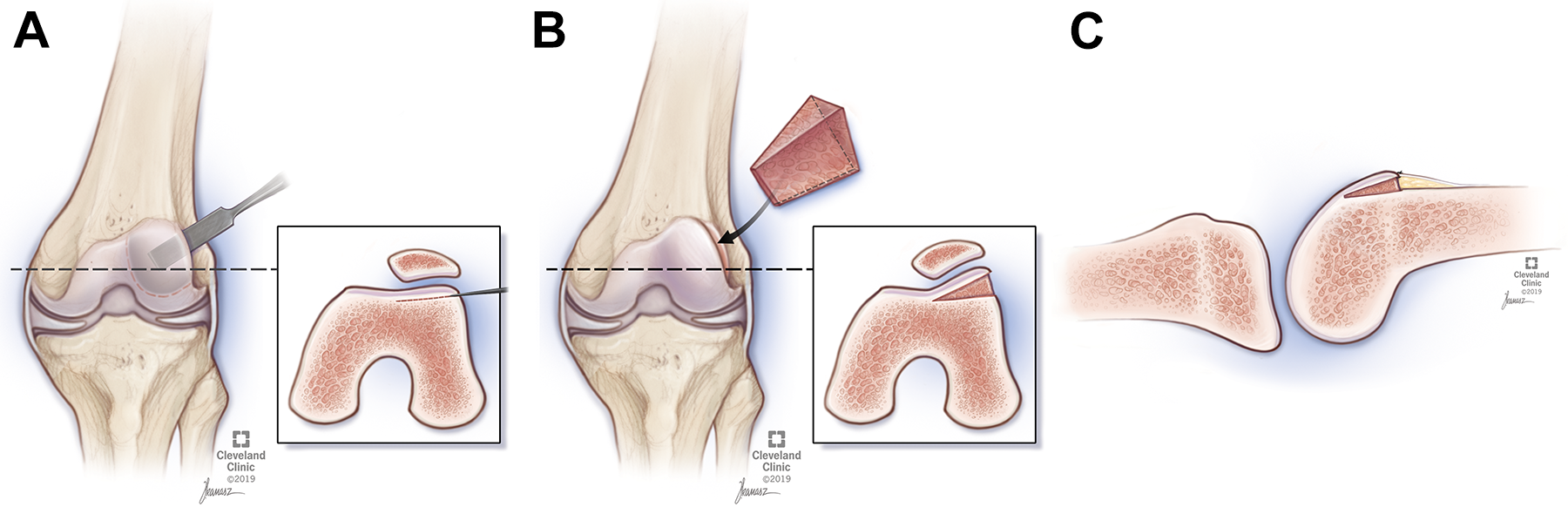
(A) The Albee osteotomy is performed from just posterior to the articular cartilage at the entry of the trochlea and angled to a point just anterior to the weightbearing surface of the lateral femoral condyle when the knee is in full extension. (B) The lateral trochlear facet is then elevated and a bone graft wedge (either cortical cancellous autograft from the distal femur or allograft) is inserted. (C) This modification to the original Albee osteotomy uses a trapezoidal instead of rectangular wedge, whereby the proximal portion of the wedge is 6 to 8 mm in width and tapered distally to a width of 2 mm. No fixation is required. (Figure courtesy of Cleveland Clinic Art and Photography.)
Although the topic of TD has been described thoroughly in the literature, and with more recent descriptions on trochleoplasty techniques, there is little information on the Albee procedure. Furthermore, although small case series reporting functional outcomes in the Albee osteotomy exist, an updated larger series with longer follow-up is indicated to further understand the functional outcomes of this procedure. The purpose of this study was to identify functional outcomes, as evaluated by patient-reported outcome measure (PROM) scores, for patients undergoing the modified Albee osteotomy. We hypothesized that patients will have acceptable pain and function at mid- to long-term follow-up.
Methods
Study Design
This study was approved by our institutional review board as a minimal-risk study. Patients were included from a single surgeon’s modified Albee osteotomy registry (J.T.A.); in total, 46 patients undergoing a total of 49 procedures were identified from 1999 to 2017. Notably, all patients underwent at least 1 additional procedure at the time of surgery. No exclusion criteria were applied owing to the small sample size and greater than 5-year follow-up in every patient.
Patients were contacted from May 2019 to September 2019 up to 11 times and were asked to complete 4 PROMs either by telephone or through an electronic survey based on their preference. In an attempt to minimize bias, the individuals contacting the patients were authors (P.J.B., J.W., P.O.H., E.K.) who played no role in the care of the patient. For the patients who participated, their demographics (age at surgery, race, laterality, date of surgery, sex, and concurrent procedures) and postoperative complications were collected via direct chart review.
Of the 46 patients (49 procedures), 32 patients (36 procedures) were contacted successfully, 13 patients could not be contacted, and 1 had passed away. Of the 32 patients (36 knees) contacted successfully, 1 declined to participate (2 procedures) and 3 did not fill out the electronic survey, leaving 28 patients (30 procedures) with PROM scores.
Measured Outcomes
The 4 PROMs used were the Kujala Anterior Knee Pain Scale (AKPS), International Knee Documentation Committee (IKDC), Activity Rating System (ARS), and pain visual analog scale (VAS); in addition, dislocations since Albee osteotomy surgery and postoperative complications were investigated. The AKPS is a questionnaire with a 0- to 100-point scale used to evaluate symptoms related to the patellofemoral joint. A score of 100 signifies no symptoms. 11 The IKDC 2000 version is a knee-specific questionnaire with a 0- to 100-point scale that evaluates symptoms, function, and sports-related activity. 9 No objective scoring was used. A score of 100 represents no knee-specific limitations in the activities of daily living and recreation, as well as no symptoms related to the knee. The ARS is a questionnaire with a scale from 0 to 16 that evaluates the patient’s activity levels based on activities such as cutting or acceleration that are not specific to an individual sport. 18 A score of 16 indicates participation in running-, cutting-, pivoting-, and declaration-type activities at least 4 times a week over the past 4 years. The VAS is a 0- to 100-point scale that measures pain, with 100 defined as the most pain possible. The occurrence of a dislocation was recorded in 2 ways: through direct chart review from the date of surgery through the last follow-up visit, and by using the AKPS, which documents painful patellar dislocations and subluxations. When a discrepancy in the 2 modes of collection existed, the patient was assumed to have had a dislocation event. Last, postoperative complications were collected through direct chart review of all postoperative visits.
Data Analysis
Frequencies for the demographics of sex, race, laterality, and concurrent procedures; dislocations; and complications were tabulated. Means and standard deviations, as well as medians and interquartile ranges (IQRs), were calculated for age and the PROMs. Mean follow-up time from the day of surgery to the last follow-up visit and the date on which the PROMs were completed were also obtained.
Results
Patient Demographics
Table 1 contains demographic data, including concurrent and past procedures performed.
Demographic Data of Patients Who Underwent the Modified Albee Procedure (n = 28) a

a Data are reported as n (%) unless otherwise indicated. LPFL, lateral patellofemoral ligament; MPFL, medial patellofemoral ligament; MUA, manipulation under anesthesia; ORIF, open reduction internal fixation; VMO, vastus medialis oblique.
Measured Outcomes
The follow-up for PROMs occurred at a mean of 162 months (minimum, 82 months), whereas the median was 156 months (IQR, 119-213.5). The mean and median scores for the 4 PROMs are listed in Table 2.
Patient-Reported Outcome Measure Scores After the Modified Albee Procedure a
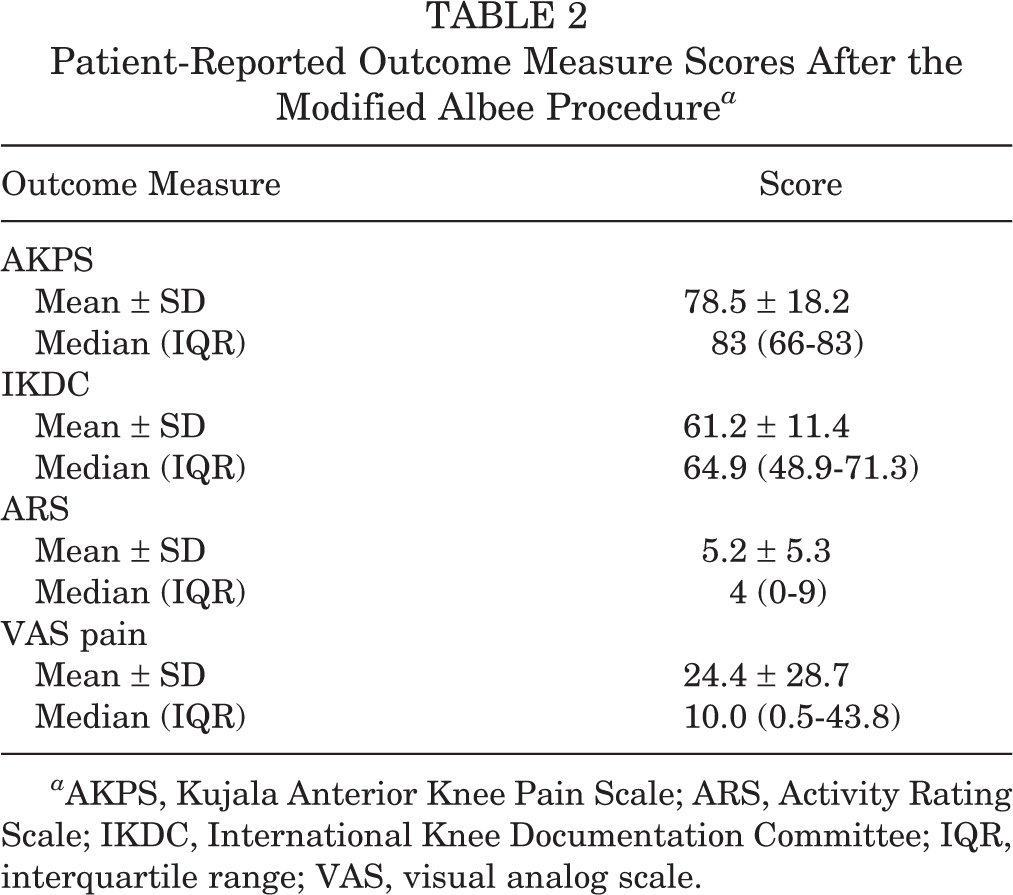
a AKPS, Kujala Anterior Knee Pain Scale; ARS, Activity Rating Scale; IKDC, International Knee Documentation Committee; IQR, interquartile range; VAS, visual analog scale.
The mean time for the in-person follow-up was 57 months. Complications occurred in 3 patients. Two (6.7%) patients required manipulations under anesthesia (MUAs). Two (6.7%) patients dislocated, 1 of which was a patient with MUA that subsequently dislocated and required a revision surgery for a lateral lengthening and medial patellofemoral ligament reconstruction. Notably, the patient who had a dislocation reported no further dislocations during PROM questioning.
Discussion
Femoral TD is a relatively infrequent condition but is highly correlated with patellofemoral dislocation. 5,16 A modified Albee osteotomy can be used to elevate the lateral femoral condyle in an effort to prevent future dislocations. 20 Our “modification” of the osteotomy refers to the trapezoidal design of the bone wedge, which replaces the rectangular shape described by Weiker and Black 22 or the distally based wedge described by Albee 1 in order to avoid cracking through the articular cartilage distally. The literature describing outcomes of the Albee procedure is limited, with no study in existence with greater than 19 patients. 4,10,22 A systematic review of 392 knees from 14 articles found that the Bereiter technique was the technique performed most commonly, whereas the Dejour technique had the best postoperative Kujala score of 79.3 (SD, ±8.4) points. 17 Although their literature review included “Albee Trochleoplasty” in its search terms, no articles on the topic that fit their inclusion criteria were found. Several case series have been performed, with sample sizes ranging from 4 to 19 patients with minimum follow-up times of 2 years to 65 months. 4,10,22 All of these studies reported low rates of further dislocation.
Our study found that that the mean PROMs were 78.5 ± 18.2 for the AKPS, 61.2 ± 11.4 for the IKDC, 5.2 ± 5.3 for the ARS, and 24.4 ± 28.7 for the VAS following a modified Albee procedure. These scores indicate that patients had mild pain and symptoms but were not able to return to sporting activities. Only 2 of our patients had a dislocation, 1 of which occurred after an MUA and necessitated reconstruction, after surgery, with a total of 3 having postoperative complications.
Badhe and Forster 4 presented a case series of 4 patients. All patients subsequently had a stable patellofemoral joint, but also residual patellofemoral pain after undergoing an Albee osteotomy combined with a modified Fulkerson Elmslie-Trillat osteotomy, a patellar osteotomy, a lateral release, and a medial plication. 2 None of these patients were able to return to sporting activities owing to pain; however, all were able to perform activities of daily living without bracing. Notably, all patients had a 10° to 20° loss of flexion. The case series by Badhe and Forster differs from ours because of the inclusion of a patellar osteotomy, which was not implemented in any of the patients in our series.
A larger case series of 19 trochleoplasties indicated for patellofemoral instability with TD treated exclusively with the Albee osteotomy procedure found that only 2 of the knees had suffered a subluxation event after 2 years of follow-up, with no frank dislocations. 10 All the patients in this latter study reported improvement in pain and function using Lysholm, functional knee score for patellofemoral pain, and Western Ontario and McMaster Universities Osteoarthritis Index PROMs. For 16 of the 19 procedures, the patient reported a willingness to undergo the same surgery, whereas 3 reported that they would not.
A 1997 review by Weiker and Black 22 described 5 patients with patellofemoral instability refractory to both prior surgical and nonsurgical interventions. They were treated exclusively with an Albee osteotomy procedure and found that, after a minimum of 65 months follow-up, only 1 patient had a subsequent dislocation. However, all 5 patients had complications and required subsequent surgical interventions. One patient had an MUA, whereas 2 others required an open lysis of adhesions; these patients regained their motion after these interventions. One patient who had degenerative changes required a patellectomy 15 months after her osteotomy. The final patient had a traumatic dislocation 4.5 years from the procedure and had a repeat medial capsular imbrication. In addition, 3 of the 5 patients had symptoms during athletics, 1 during activities of daily living and 1 who had functional status that was considered poor. It should be noted that this study differs from ours in that a rectangular wedge of 8 to 10 mm was used as opposed to a trapezoidal shape of 6 mm.
Our study does have limitations. Owing to the retrospective nature of this study, no baseline preoperative PROMs were collected. Similarly, there was no postoperative imaging or physical examination data available at follow-up. The results of our study might also be confounded by the multiple associated procedures included with each of our trochleoplasty surgeries (see Table 1). In addition, this study lacks controls and a comparison group, making it difficult to ascertain whether the procedure affected the natural course of the patient’s condition that would have resulted otherwise from the associated procedures alone. Selection bias may have been introduced into our study, as nearly one-third of patients were lost to follow-up. Although contact with each patient was attempted numerous times (up to 12 times in some cases), 13 patients could not be reached. Some of these patients might have opted not to contact us back owing to suboptimal outcomes. With regard to the lack of return to sporting activity after the operation, there was no clear established documentation describing a baseline level of sporting activity for these patients. This work may not be generalizable to all Albee osteotomy patients, as the procedure was conducted by a single experienced surgeon (J.T.A.) involved with the aforementioned modification of the procedure. Despite these limitations, this is still the largest case series to date assessing the mid- to long-term outcomes of a modified Albee osteotomy procedure.
Conclusion
This study indicates that the modified Albee procedure in conjunction with other procedures can be considered a success when its goal is the prevention of further patellofemoral dislocations. With only mild symptoms and functional activity limitations, these data can be used to counsel patients with TD who are indicated for use of a modified Albee procedure and other concomitant procedures.
Footnotes
Final revision submitted February 26, 2021; accepted March 4, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: L.D.F. has received consulting fees from Zimmer Biomet. P.O.H. has received education payments from Arthrex and Smith & Nephew and hospitality payments from Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Cleveland Clinic (ID No. 19-406).