
Abstract
Background:
Supervised machine learning models in artificial intelligence (AI) have been increasingly used to predict different types of events. However, their use in orthopaedic surgery has been limited.
Hypothesis:
It was hypothesized that supervised learning techniques could be used to build a mathematical model to predict primary anterior cruciate ligament (ACL) injuries using a set of morphological features of the knee.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Included were 50 adults who had undergone primary ACL reconstruction between 2008 and 2015. All patients were between 18 and 40 years of age at the time of surgery. Patients with a previous ACL injury, multiligament knee injury, previous ACL reconstruction, history of ACL revision surgery, complete meniscectomy, infection, missing data, and associated fracture were excluded. We also identified 50 sex-matched controls who had not sustained an ACL injury. For all participants, we used the preoperative magnetic resonance images to measure the anteroposterior lengths of the medial and lateral tibial plateaus as well as the lateral and medial bone slope (LBS and MBS), lateral and medial meniscal height (LMH and MMH), and lateral and medial meniscal slope (LMS and MMS). The AI predictor was created using Matlab R2019b. A Gaussian naïve Bayes model was selected to create the predictor.
Results:
Patients in the ACL injury group had a significantly increased posterior LBS (7.0° ± 4.7° vs 3.9° ± 5.4°; P = .008) and LMS (–1.7° ± 4.8° vs –4.0° ± 4.2°; P = .002) and a lower MMH (5.5 ± 0.1 vs 6.1 ± 0.1 mm; P = .006) and LMH (6.9 ± 0.1 vs 7.6 ± 0.1 mm; P = .001). The AI model selected LBS and MBS as the best possible predictive combination, achieving 70% validation accuracy and 92% testing accuracy.
Conclusion:
A prediction model for primary ACL injury, created using machine learning techniques, achieved a >90% testing accuracy. Compared with patients who did not sustain an ACL injury, patients with torn ACLs had an increased posterior LBS and LMS and a lower MMH and LMH.
Keywords
Anterior cruciate ligament (ACL) injuries are seen commonly in athletes participating in contact sports. The incidence of these injuries is relatively high, exceeding 200,000 cases per year in the United States. 30 ACL tears can cause knee instability with pivoting and cutting, increasing the risk of developing knee osteoarthritis and eventually necessitating total knee replacement. 10,34
Various anatomic features, such as tibial slope, size of the femoral notch, alignment of the lower extremities, and, more recently, medial and lateral meniscal thickness, have been found to be associated with primary ACL injuries. 2,16,40 Moreover, some reports have also shown that the athlete’s knee biomechanics during jumping and landing could alter the tension forces on the ACL and eventually influence the risk of sustaining an ACL injury. 28 Some authors have postulated that the knee anatomic features of an individual could be used to predict primary ACL injuries. 16,29 However, most of these factors have shown limited sensitivity and specificity in the prediction of primary ACL injuries, 29 and it is often difficult to use these factors as individual tools to predict ACL injuries or manually find a reliable combination of factors to do so.
Supervised machine-learning models in artificial intelligence (AI) have been increasingly used to predict different types of events in multiple fields, such as agriculture, telecommunications, banking, computer networks, and even climate change. 35,44 Supervised learning relies on experience: A set of samples (training set) is collected, including relevant input variables and the associated dependent output. This set is used to build a mathematical model that allows reliable prediction of output data using a proper combination of relevant input variables, even for data not included in the training set. 22 Accordingly, we hypothesized that supervised learning techniques could be used to build a mathematical model to predict primary ACL injuries using a set of morphological features of the knee as input data.
Methods
Study Design and Patient Selection
The study protocol was reviewed and approved by the research ethics board at our institution. We performed a cross-sectional study on 50 young adults who underwent a primary ACL reconstruction between 2008 and 2015. Clinical information was collected from our departmental electronic database. Only individuals who were aged between 18 and 40 years at the time of surgery were included in this study; the upper limit of time from injury to surgery of the included patients was 6 months. Patients with a previous ACL injury (ie, contralateral ACL injury, patients undergoing ACL revision surgery), multiligament knee injury, complete meniscectomy, infection, missing data, and associated fracture were excluded. We also identified 50 sex-matched controls who had a magnetic resonance imaging (MRI) of the knee during the same period and did not sustain an ACL injury. The same exclusion criteria were applied to this group. Figure 1 shows the patient selection flowchart.
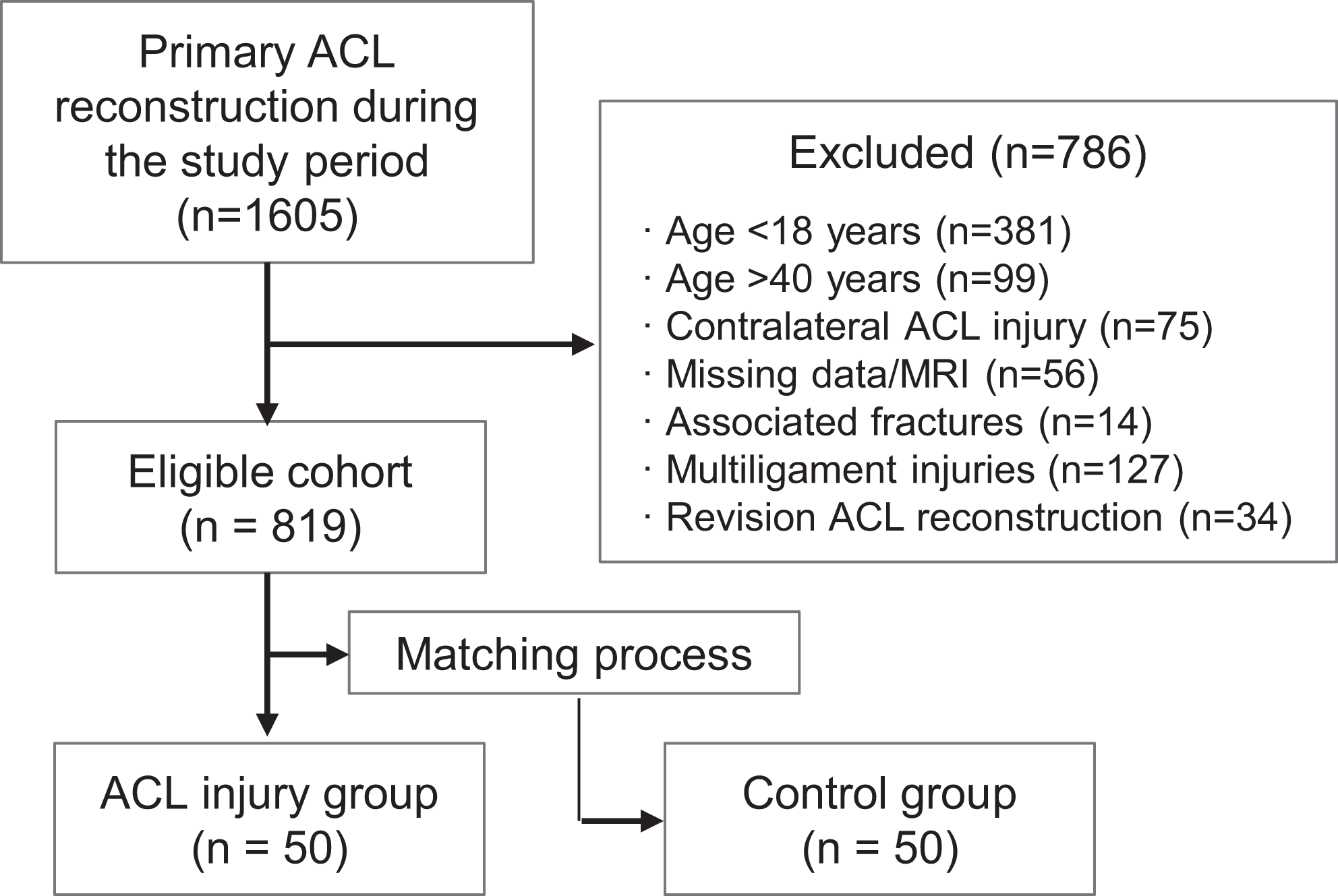
Flowchart illustrating the patient selection process. ACL, anterior cruciate ligament; MRI, magnetic resonance imaging.
MRI Analysis
The MRI studies were performed using a 1.5-T magnetic field (Signa HDxT) with an 8-channel knee coil (HD TR knee array). Images were performed following the standard departmental knee MRI protocol, which included sagittal fat-suppressed fast spin-echo T2-weighted images (repetition time/echo time [TR/TE], 4000/70), sagittal fat-suppressed spin-echo proton density (PD) images (TR/TE, 2000–3000/42), coronal fat-suppressed PD sequence (TR/TE, 2000–3000/42), axial fat-suppressed spin-echo PD images (TR/TE, 2000/42), and sagittal PD sequence (TR/TE, 2000–3000/42). Slices had a thickness of 4 mm, with a 0.4-mm interslice gap. The IntelePACS (Intelerad) system was used to analyze preoperative MRI images.
The MRI analysis was performed independently by an orthopaedic surgeon (I.T.) and an experienced radiologist (A.P.L.). The analysis was performed in 2 steps: image selection and image analysis.
First, a T2 axial image showing the proximal end of the tibial plateau was selected. Then, a transverse line was drawn through the proximal transtibial axis on this image to identify the midpoint of the transtibial axis and the center of the medial and lateral tibial plateaus. These points were used to select 3 sagittal T1-weighted images, including the medial and lateral central sagittal planes (MCSP and LCSP), at the center of the transtibial axis (Figure 2, B-D).

Magnetic resonance images showing (A) the sagittal axis of the tibia; (B) the transtibial axis of the tibia (*anteroposterior length of the medial tibial plateau, ¥anteroposterior length of the lateral tibial plateau); (C) the medial tibial bone slope; and (D) the lateral tibial bone slope.
Second, the readers were blinded and had access only to the 4 MRI images mentioned previously. The central T1 sagittal cut was used to determine the proximal tibial sagittal axis (PTSA) as described by Hudek et al 19 (Figure 2A). The bone slope, meniscal height, and meniscal slope were measured on the MCSP and LCSP (Figure 2, C and D; Figure 3, A and B; and Figure 3, C and D, respectively). 7,15,19 The medial and lateral tibial bone slopes (MBS and LBS) were calculated as the angle between a line joining the highest points of the anterior and posterior tibial plateaus and a line perpendicular to the PTSA 7 (Figure 2, A, C, and D). The medial and lateral meniscal slopes (MMS and LMS) were calculated as the angle between the tangent line to the highest points of the anterior and posterior horns of the menisci and a line perpendicular to the PTSA (Figure 3, C and D). 7 The heights of the menisci were calculated by measuring the perpendicular distance between highest and lowest points of the posterior horn of the menisci on the MCSP and LCSP (Figure 3 A and B). 8

Magnetic resonance images showing (A) medial meniscal height (asterisk); (B) lateral meniscal height (asterisk); (C) medial meniscal slope (angle between solid and dashed lines); (D) lateral meniscal slope (angle between solid and dashed lines).
Statistical Analysis
A normality analysis was performed to continuous variables using the Shapiro-Wilk test. Differences between continuous variables were assessed using the Student t test or Mann-Whitney U test. P values were considered statistically significant if less than .05. The statistical analysis was performed using SPSS Version 22.0 (IBM).
AI Predictor
The AI predictor was created using Matlab R2019b (MathWorks). A Gaussian naïve Bayes model was selected to create the predictor. 21 Naïve Bayes algorithms can work directly with the morphological features, without scaling or normalizing input data, thereby increasing the predictor’s interpretability. Naïve Bayes models also assume independency between input features. In this study, multiple naïve Bayes predictors were trained (ie, 1 per each independent variable). We calculated the sensitivity, specificity, and accuracy (ie, correctly classified patients) of these predictors.
Neighborhood component analysis (NCA) was also performed to obtain a subset of the analyzed anatomic features and remove redundant information. 12 The naïve Bayes predictors per independent variable were calculated as well as the predictors using the combination of features obtained by NCA.
Of the 100 study participants, 76 were used randomly to train and validate the proposed predictor, and 24 to test the model by measuring the specificity and sensitivity in unknown patients.
Results
The average patient age was 20.4 ± 3.88 in the ACL injury group and 23.6 ± 5.63 years in the control group (P = .006); 16 male and 22 female patients were included in each group. Patients in the ACL injury group had an increased posterior LBS (7.0° ± 4.7° vs 3.9° ± 5.4°; P = .008) and LMS (–1.7° ± 4.8° vs –4.0° ± 4.2°; P = .002) compared with individuals in the control group. However, a lower lateral meniscal height (LMH) was observed in the ACL injury group compared with the control group (6.9 ± 0.1 mm vs 7.6 ± 0.1 mm; P = .001) (Table 1). No other lateral compartment differences were observed between the 2 groups. In the medial compartment, patients in the ACL injury group had a lower medial meniscal height (MMH) compared with individuals in the control group (5.5 ± 0.1 vs 6.1 ± 0.1; P = .006). No other medial compartment differences were observed between the 2 groups (Table 1). An interobserver Cohen kappa coefficient of more than 80% was achieved for the MRI measurements.
Anatomic Features of the Validation Group as Measured on MRI a

a Bold P values indicate statistically significant difference between groups (P < .05). ACL, anterior cruciate ligament; MRI, magnetic resonance imaging.
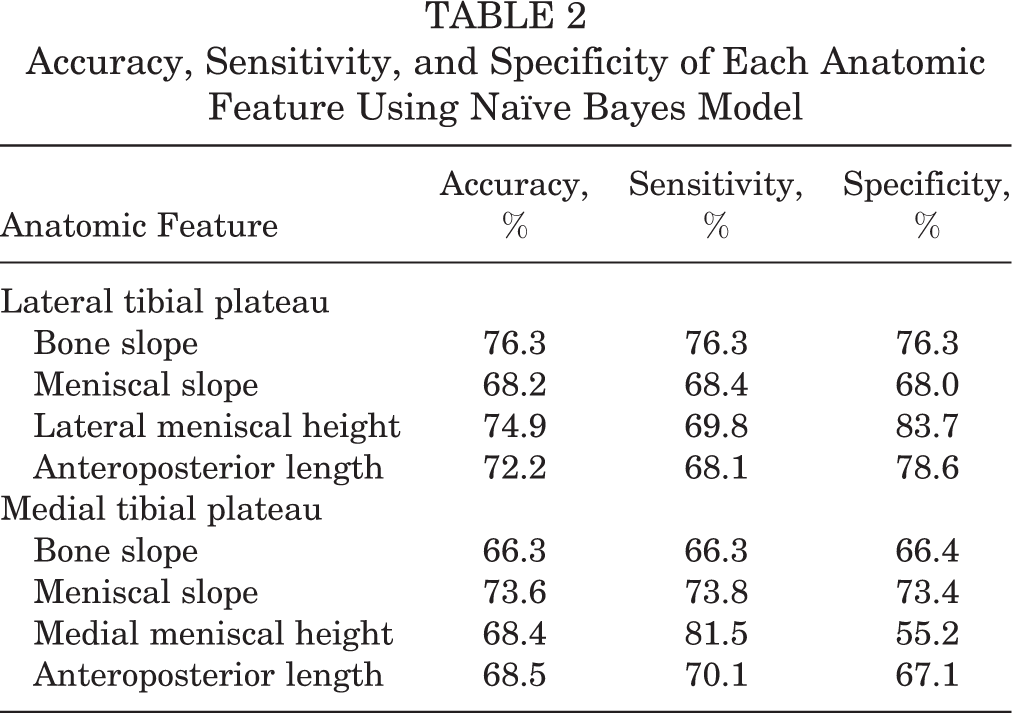
A naïve Bayes predictor can be created with single or multiple features. The accuracy, sensitivity, and specificity of each independent variable using the naïve Bayes algorithms are presented in Table 2. The subset obtained with NCA, including the LBS and MBS, is presented in Table 3. The naïve Bayes model created a parabolic mathematical model based on the LBS and MBS (Figure 4).
Accuracy, Sensitivity, and Specificity of Each Anatomic Feature Using Naïve Bayes Model
Performance of Naïve Bayes Model


Naïve Bayes model. Lateral bone slope (x-axis) and medial bone slope (y-axis) values are clustered into 2 groups: patients with ACL injury and patient controls. (A) The validation group. The white asterisks represent patients with ACL injury; the black plus signs represent the control group. (B) The testing group. The blue asterisks represent patients with ACL injury; the black plus signs represent the control group. ACL, anterior cruciate ligament.
Discussion
In this study, we analyzed multiple knee morphological features to develop an AI model for the prediction of ACL injury. According to MRI, patients in the ACL injury group had an increased LBS and LMS, and a lower MMH and LMH, compared with uninjured controls. We managed to create a prediction model for primary ACL injury using 2 variables (LBS and MBS), achieving a >90% testing accuracy.
Anatomic Features of the Knee
In this study, we observed that the lateral tibial slope was steeper in patients with ACL injuries. These results corroborate the findings of previously published studies. 6,43 Several MRI-based reports have indicated that the lateral tibial slope could play a major role in the biomechanics of ACL injury. 9 Under axial loading, the lateral femoral condyle shifts posteriorly over the lateral tibial plateau, resulting in a relative external rotation of the femur and, to a lesser extent, an internal rotation of the tibia. 27 Therefore, a steeper lateral tibial plateau could facilitate this mechanism. Previous research has also confirmed the relationship between increased tibial slope angle as measured off the medial tibial plateau on radiographic studies and increased risk of ACL tear and increased anterior tibial translation. 3
In this study, we observed that patients with ACL injuries had a lateral and medial tibial slope of 7.0° ± 4.7° and 3.9° ± 5.4°, respectively. The lateral tibial slope in patients with ACL injuries has been previously described to range between 5.7° and 6.0°. The medial slope, however, has been reported to be slightly lower, ranging between 5° and 5.4°. 6,43 A significant degree of variability has been reported between different imaging (ie, plain radiographs, computed tomography scans, and MRI scans) and measurement methods of the tibial slope. 19,33 Accordingly, in our study, the medial tibial slope was relatively lower compared with those of previous reports. Interestingly, again, in our study, the medial tibial slope did not appear as a significant independent risk factor for ACL injury under the standard statistical analysis. However, the AI analysis selected the LBS and MBS as the best possible predictive combination. The model revealed that the risk of a primary ACL injury is higher with increased lateral posterior tibial and decreased medial slopes. As mentioned previously, a steeper lateral tibial plateau could facilitate a relative external rotation of the femur and an internal rotation of the tibia. Our AI analysis suggests that the medial tibial slope could also be involved in this mechanism. Accordingly, a combination of a decreased medial tibial slope and increased lateral slope would offer less resistance to the external rotation of the femur and the internal rotation of the tibia.
On the other hand, we observed that lateral meniscal slope was more horizontal in patients with ACL injury. However, no MMS differences were found between the 2 groups. Research on the relationship between the MMS or LMS and ACL injury is scarce. An increased LMS has been reported to be associated with increased risk of lateral bone contusions in noncontact ACL injury. 25 Moreover, Elmansori et al 7 reported that the LMS and MMS are increased in patients with ACL tears. Hudek et al 18 also analyzed the influence of the meniscal slope on ACL tears, finding an increased LMS in patients with ACL tears. As in our study, research has shown that the meniscal slope is more horizontal than the bony slope in both compartments. 7,26
A lower LMH was observed in the ACL injury group. In a recent study that analyzed the effect of the lateral meniscal wedge angle on the risk of sustaining an ACL injury, the authors reported that a degree decrease in the lateral meniscal wedge angle was associated independently with a 23% increase in the risk of sustaining an ACL injury. 39 These findings suggest that the lateral meniscus could represent a mechanical obstacle during the internal rotation of the tibial plateau, acting as a secondary stabilizer of the knee. In this study, we observed that the LMH was 6.9 ± 0.1 mm in patients with ACL injuries and 7.6 ± 0.1 mm in patients with no ACL tears. These results are within the range of reported measurements in the literature, which have been described to range between 5.4 and 7.7 mm. 1,8,36 We also observed that patients in the ACL injury group had a lower MMH. Research has shown that a decreased MMH could be a risk factor for primary ACL injury and ACL reconstruction failure in female athletes. 24 Moreover, the presence of a concomitant tear in the posterior horn of the medial meniscus has been associated with increased knee instability in ACL-deficient joints. 13
In this study, we did not observe differences between the study groups regarding anteroposterior lengths of the medial and lateral tibial plateaus. Research on the relation between the tibial plateaus lengths and ACL injury is very scarce. Some authors have postulated that a longer anteroposterior distance of the lateral tibial plateau could increase the rotational translation forces of the tibia, 24 which could consequently increase the kinetic energy of the lateral femoral condyle and expose the ACL fibers to higher tensional forces and increase the risk of ACL tear.
Prediction of ACL Injury
The normal biomechanical function of the ACL is influenced by multiple anatomic factors, such as an increased lateral tibial posterior slope, 6,43 smaller ACL diameter, 37 a narrow femoral intercondylar notch, 41 LMH, 39 leg-length discrepancies, 23 and the valgus alignment of the lower extremities. 20 Most of these variables could be measured with a simple radiograph or MRI scan and used to identify high-risk patients. However, the sensitivity and specificity of these isolated measurements is usually limited. The combination of different variables as algorithms could potentially improve the accuracy of these tests. However, identifying the ideal combination of variables with their corresponding cutoff points would be an extremely difficult task without the aid of AI.
Several ACL injury-prediction algorithms have been described in recent years. Myer et al 32 reported a prediction algorithm to identify female patients at high risk of sustaining an ACL tear using sensitive laboratory-based tools to determine predictive mechanisms that underlie increased knee abduction moment during landing. The same authors also published a new method to identify athletes with a high risk of ACL injury based on clinic-based measurements and computer analysis, based on knee abduction moment. 31 However, a recent nested-case control study performed on 1855 female athletes over a 3-year period found that the knee abduction moment was not associated with noncontact ACL injury. 11 Hewett et al 16 recently described a systematic selection of several logistic regression variables for the prediction of secondary ACL injury with a high sensitivity and specificity. This model included the assessment of transverse plane hip net moment impulse, asymmetrical sagittal plane knee moment at initial contact, 2-dimensional frontal plane knee excursion, kinesthesia, and balance and involved limb postural stability deficits. 16 The evaluation of these variables would need an available biomechanical laboratory and well-trained technicians. Therefore, there is a need for the improvement of the current models and the development of new practical, more accurate and reproducible algorithms.
On the other hand, there has been growing interest in recent years on the use of AI in medicine. It has been used in very different fields ranging from the generation and simultaneous computation of novel genomic features 17 to the evaluation of postoperative life expectancy of patients with lung cancer. 5 In orthopaedics, a customized 3-D Deep Learning architecture has demonstrated an accuracy above 96% in the diagnosis of complete ACL tears. 4 Moreover, a decision-support model was used to aid differentiation between partial ACL injuries and complete ACL tears using knee MRI scans. 38 In this study, we managed to create a novel predictive model for primary ACL injury with a more than 90% accuracy. This model relies on only 2 variables that can be measured easily before the injury and can be obtained from a standard MRI scan of the knee. This model could be used as a screening tool to identify high-risk patients, one that could give them the opportunity to follow prevention measures such as the use of knee braces, 14 lifestyle modifications, and the implementation of ACL prevention programs. 42
Strengths and Limitations
We present a novel model for the prediction of primary ACL injuries using AI. This algorithm is relatively simple and relies on only 2 variables that could be easily measured on a regular MRI scan of the knee. Moreover, the prediction model only requires the sagittal sequence of the knee, potentially reducing the cost of MRI screening in an uninjured player purely for the purposes of risk assessment. In addition, this study could be used as a precursor for the creation of future models that could include more variables and larger databases.
Ultimately, AI analyses could be used in the future to identify high-risk patients with customized software. On the other hand, our study also presents a number of limitations. The sample size of the study was limited, and we did not include some morphological factors that could influence primary ACL injuries, such as the notch size and alignment of the lower extremities. In addition, patients were only matched by sex, and no propensity or activity level scores were used in this study.
Conclusion
Patients with ACL injury had an increased lateral tibial posterior slope and lateral meniscal slope and a lower medial meniscus and LMH. An algorithm for the prediction of primary ACL injury was created using machine learning techniques, achieving a more than 90% testing accuracy. The final model included lateral tibial slope and medial tibial slope. This AI model should be further investigated in the prediction of failed ACL reconstruction surgery.
Footnotes
Final revision submitted February 22, 2021; accepted March 2, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.B. has received research support from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from McGill University Health Centre.