
Abstract
Background:
In a sheep rotator cuff model, tenotomy predominantly induces fatty infiltration, and denervation induces mostly muscle atrophy. In clinical practice, myotendinous retraction after tendon tear or lateralization after tendon repair tear may lead to traction injury of the nerve.
Purpose/Hypothesis:
To analyze whether an additional nerve lesion during rotator cuff repair leads to further degeneration of the rotator cuff muscle in the clinical setting. We hypothesized that neurectomy after tendon tear would increase atrophy as well as fatty infiltration and that muscle paralysis after neurectomy would prevent myotendinous retraction after secondary tendon release.
Study Design:
Controlled laboratory study.
Methods:
Twelve Swiss alpine sheep were used for this study. For the 6 sheep in the tenotomy/neurectomy (T/N) group, the infraspinatus tendon was released; 8 weeks later, the suprascapular nerve was transected. For the 6 sheep in the neurectomy/tenotomy (N/T) group, neurectomy was performed, and the infraspinatus was tenotomized 8 weeks later. All sheep were sacrificed after 16 weeks. Magnetic resonance imaging (MRI) was performed before the first surgery (baseline) and then after 8 and 16 weeks. The MRI data were used to assess muscle volume, fat fraction, musculotendinous retraction, pennation angle, and muscle fiber length of the infraspinatus muscle.
Results:
Three sheep (2 in the T/N and 1 in the N/T group) had to be excluded because the neurectomy was incomplete. After 8 weeks, muscle volume decreased significantly less in the T/N group (73% ± 2% of initial volume vs 52% ± 7% in the N/T group; P < .001). After 16 weeks, the mean intramuscular fat increase was higher in the T/N group (36% ± 9%) than in the N/T group (23% ± 6%), without reaching significance (P = .060). After 16 weeks, the muscle volumes of the N/T (52% ± 8%) and T/N (49% ± 3%) groups were the same (P = .732).
Conclusion:
Secondary neurectomy after tenotomy of a musculotendinous unit increases muscle atrophy. Tenotomy of a denervated muscle is associated with substantial myotendinous retraction but not with an increase of fatty infiltration to the level of the tenotomy first group.
Clinical Relevance:
Substantial retraction, which is associated with hitherto irrecoverable fatty infiltration, should be prevented, and additional neurogenic injury during repair should be avoided to limit the development of further atrophy.
Keywords
One key limiting factor for the successful repair of long-standing rotator cuff tears is musculotendinous retraction, which is characterized by change of the pennation angle of the muscle with corresponding fiber shortening, fatty muscle infiltration, interfascicular and interfibrillar fibrosis, and atrophy. Most of these changes are currently essentially considered irreversible, so the prevention and reversion thereof are most relevant research topics. 4,8
Rotator cuff tears are associated with retraction of the musculotendinous unit. This leads to medial deviation and traction on the suprascapular nerve, 1,14 potentially causing suprascapular neuropathy. 3 During rotator cuff repair, lateral traction is applied to the musculotendinous unit, a maneuver that may also result in secondary traction injury to the suprascapular nerve. 15
In human rotator cuffs, muscle degeneration after rotator cuff tear is different from muscle degeneration caused by suprascapular nerve lesion. 2 Differences between neurologically or tenotomy-induced infraspinatus muscle degeneration have also been analyzed in a sheep model 6,7 : Suprascapular neurectomy caused greater infraspinatus muscle volume loss with a slow- to fast-twitch muscle fiber transformation and an increase of the extracellular matrix, with more edema when compared with tenotomy. 6,9,10 Conversely, tenotomy caused substantially greater fatty muscle infiltration. 6 The pennation angle in the tenotomized infraspinatus muscle increased with a corresponding decrease of muscle fiber length. As opposed to neurectomy, a fiber shift was observed from fast to slow muscle fibers. 6 The combination of neurectomy plus tenotomy did not lead to more fatty infiltration than tenotomy alone.
The most likely clinical scenario is a complete tendon tear with subsequent musculotendinous retraction and delayed suprascapular traction damage. To reproduce this situation in the sheep model, a neurectomy of the suprascapular nerve was added 6 weeks after tenotomy of the infraspinatus tendon. The aim of this study was to analyze the effect of sequential muscle damage on infraspinatus muscle degeneration. In addition, it is hitherto unknown whether denervation causes additional changes in an already retracted musculotendinous unit. We hypothesized that neurectomy after tendon tear would increase atrophy as well as fatty infiltration and that muscle paralysis would prevent myotendinous retraction after secondary tendon release.
Methods
The investigational review board and local federal authorities approved the study protocol and the use of 12 female Swiss alpine sheep (mean age, 27 ± 3 months; mean weight, 61 ± 5 kg) for the purpose of this study, confirming that the Swiss laws of animal welfare were respected. All surgical procedures followed an established anesthetic protocol. 7
Surgical Technique and Experimental Protocol
The experiments were performed on the right shoulder. After shaving the wool, we made a 15-cm skin incision along the scapular spine. In the tenotomy/neurectomy (T/N) group, 6 sheep first underwent (week 0) an osteotomy of the greater tuberosity to release the infraspinatus tendon. The osteotomy of the greater tuberosity was preferred to simple tenotomy because the edge of the bone chip is a radiographically well-defined structure suited for precise radiographic measurement of retraction. The triangular bone chip had a size of 10 × 10 × 20 mm. The bone chip with the contiguous infraspinatus tendon was enveloped into a silicon tube (12 mm–diameter Silicone Penrose Drain Tube; Fortune Medical Instrument) to prevent scarring of the released chip and tendon and allow musculotendinous retraction. 6
In the neurectomy/tenotomy (N/T) group, 6 sheep underwent a neurectomy without tenotomy at time zero (week 0). The neurectomy was performed at the level of the acromion where the nerve runs around the acromial neck. The interval between the supraspinatus and infraspinatus muscle at the level of the acromion was used to expose the suprascapular nerve. The nerve was first exposed and identified with the aid of a nerve stimulator (Stimuplex HNS 11; B. Braun Melsungen; and Polymedic 21-gauge stimulation needle, Temena). The nerve was divided, and the proximal part of the nerve was excised to prevent reinnervation. After hemostasis, the fascia, subcutaneous layer, and skin were closed, and a compressive dressing was added with staples to prevent postoperative hematoma.
After surgery, all sheep underwent a magnetic resonance imaging (MRI) scan of the right and left shoulder under general anesthesia. Eight weeks after the first surgical intervention, all sheep had another MRI scan under general anesthesia immediately before the second surgical intervention. Under the same general anesthesia, the sheep were transported to the operating room to perform the neurectomy in the T/N group and the tenotomy in the N/T group. Sixteen weeks after the first surgery and 8 weeks after the second surgery, the sheep were again anesthetized, and the same standardized MRI scans were performed followed by harvesting of the right and left musculotendinous limb. At the end of the surgery, all sheep were sacrificed.
Magnetic Resonance Imaging
MRI was performed with the sheep under general anesthesia in the supine position. The paws were tied together, and a 1-kg pull was added to the paws in a caudal direction to expose the scapula for the MRI scan. T1-weighted turbo spin-echo (TSE) transverse, proton density–weighted TSE transverse, T1-weighted TSE coronal, T2-weighted spectral presaturation with inversion recovery coronal, and Dixon transverse in-phase, transverse out-phase, transverse water-only, and transverse fat-only pulse sequences were performed. The readout of the MRI scans with a Digital Imaging and Communications in Medicine 32-bit Osirix Version 5.6 viewer was performed by 1 coauthor (A.H.), who, for the 16-week analysis, was blinded to the animals’ group affiliation. A previous intraobserver analysis had shown an excellent intraobserver correlation for the volume calculation and fat fraction. 5
Muscle Volume
On the T1-weighted transverse images, all segmented images containing the infraspinatus muscle were used to calculate the infraspinatus total muscle volume.
Fatty Infiltration
On the transverse Dixon sequences, the fat fraction of the infraspinatus muscle was measured using the previously described and validated technique. 5,6
Myotendinous Retraction, Pennation Angle, and Fascicle Length
On T1-weighted transverse images of the scapula, the bone chip retraction representing myotendinous retraction, the pennation angle, and muscle fiber length of the medial and lateral muscle fibers related to the central tendon of the infraspinatus and its medial and lateral aspects of the muscle were measured according to a previously described protocol. 5,6
Statistical Analysis
None of the factor levels showed deviation from normal distribution when tested with the Shapiro-Wilk test, and consequently, parametric inference tests were employed. To assess differences in changes of the respective outcome between the groups over all points in time, a repeated-measures analysis of variance (ANOVA) with Greenhouse-Geisser correction was employed. For post hoc comparisons, the absolute changes in fatty infiltration and sheep weight from baseline to each follow-up measurement were computed. Likewise, relative changes in infraspinatus muscle volume were calculated. Significant factors between the groups were then analyzed in a pairwise manner between the groups with independent-samples t tests. These P values were Bonferroni-corrected. Muscle weight was compared between the treatment groups using univariate ANOVA. If not stated otherwise, means and standard deviations are reported. The analysis was conducted with IBM SPSS Statistics for Windows Version 24.0 (IBM). P <.05 was considered statistically significant.
Results
Dropouts
In 3 sheep (2 in the T/N group and 1 in the N/T group), an intact branch of the suprascapular nerve was observed while harvesting the infraspinatus muscle after euthanasia, and therefore, the neurectomy had not been complete. The suprascapular nerve showed branching before winding around the scapular spine, and as such, only 1 of the branches was dissected during the first surgery. This explains why no severe atrophy was seen in the infraspinatus of these 3 sheep. These 3 sheep were excluded from analysis.
Muscle Volume
The muscle volume decreased in the T/N group from 100% at the time of surgery to 73% ± 2% after 8 weeks and to 49% ± 3% after 16 weeks. In the N/T group, the muscle volume decreased from 100% at baseline (surgery day) to 52% ± 7% after 8 weeks and 52% ± 8% after 16 weeks. The difference between the muscle decrease in the N/T group was significantly greater than the muscle decrease seen in the T/N group after 8 weeks (P < .001). After 16 weeks, the decrease of muscle volume was not different between the 2 groups (P = .732) (Figure 1).

Mean change in muscle atrophy (percentage of baseline). *P < .001. N/T, neurectomy/tenotomy; T/N, tenotomy/neurectomy.
Fatty Infiltration
Because of the different amount of fat infiltration at the beginning of the study, relative values (increase) were used to compare the 2 groups (fat infiltration was 19% ± 5% in the T/N group and 13% ± 4% in the N/T group at baseline). After 8 weeks postoperatively, the mean increase in intramuscular fat was 13% ± 4% in the T/N group and 8% ± 8% in the N/T group from baseline (P = .455). At 16 weeks, the mean intramuscular fat increase was 36% ± 9% in the T/N group compared with 23% ± 6% in the N/T group (P = .060) (Figure 2).
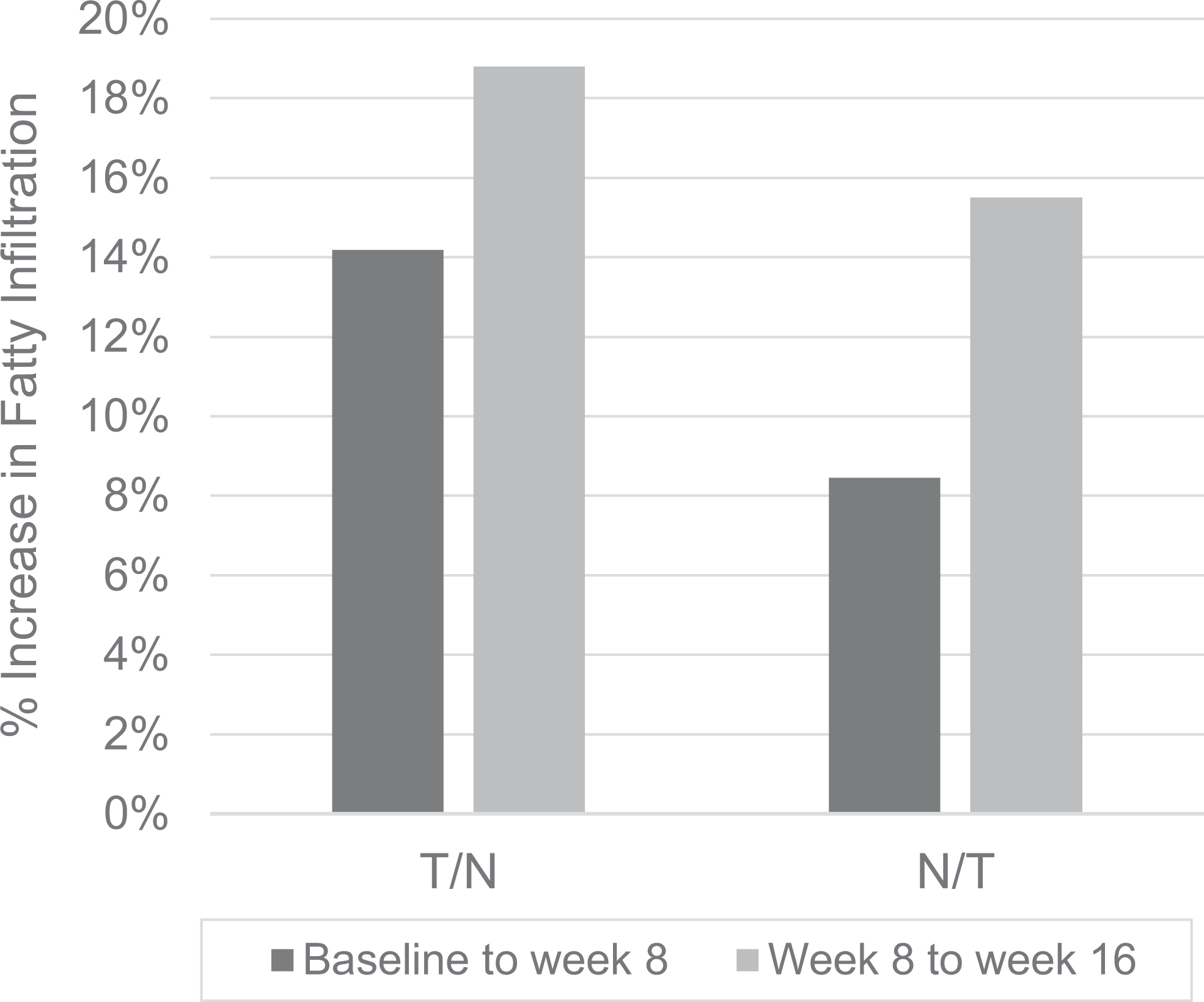
Mean percentage increase in fatty infiltration. N/T, neurectomy/tenotomy; T/N, tenotomy/neurectomy.
Musculotendinous Retraction
At week 16, the mean tendon retraction was 7.0 ± 0.5 cm in the T/N group and 6.7 ± 0.7 cm in the N/T group (P = .866).
Pennation Angle and Muscle Fiber Length
The medial pennation angle of the infraspinatus in the T/N group was 22° ± 7° at baseline, decreased to 19° ± 4° at week 8, and increased to 23° ± 4° at week 16. In the T/N group, it decreased from 25° ± 7° at baseline to 23° ± 7° at week 8 and 22° ± 8° at week 16.
The lateral pennation angle of the infraspinatus decreased in the T/N group from 25° ± 7° at baseline to 23° ± 7° at week 8 and 22° ± 8° at week 16. The lateral pennation angle decreased in the N/T group from 27° ± 7° to 15° ± 2° at week 8 and then increased to 26° ± 8° at week 16 (Figure 3).

Mean pennation angle. N/T, neurectomy/tenotomy; T/N, tenotomy/neurectomy.
The mean medial-lateral muscle fiber baseline length was 3.3 ± 0.5 cm in the T/N group and 3.5 ± 0.8 cm in the N/T group. Eight weeks after the first intervention, the mean lengths were 2.5 ± 0.5 cm and 3.5 ± 0.8 cm in the T/N and N/T groups, respectively. Eight weeks after the second intervention, the mean muscle fiber length was 2.5 ± 0.5 cm in the T/N group and 2.8 ± 1.0 cm in the N/T group (Figure 4). All reported changes in pennation angle and fiber length did not differ significantly between the 2 groups.

Mean fiber length. N/T, neurectomy/tenotomy; T/N, tenotomy/neurectomy.
Discussion
Denervation of a tenotomized muscle increases muscle atrophy in the infraspinatus muscle of sheep. Conversely, tenotomy of a denervated muscle does not. Clinically, this experimental observation is compatible with the hypothesis that a clear increase of atrophy after an established rotator cuff tear might be associated with an additional neurogenic component and with the hypothesis that rotator cuff tears associated with very pronounced atrophy could have an additional neurogenic component. Also, an increase of atrophy after repair may suggest an injury to the suprascapular nerve.
The T/N group showed a trend toward more fatty infiltration of the infraspinatus than the N/T group, without reaching significance. This result is compatible with previous findings, which showed that fatty infiltration is closely correlated with the degree of change of the pennation angle. 10
Whereas retraction leads to a substantial change in the pennation angle, denervation does not, so that the postulated effect of opening a space through architectural changes in the muscle does not apply. The pattern of fatty infiltration caused by secondary neurectomy is not significantly different from single-stage tenoneurectomy. It is notable that the pennation angle remains close to normal after neurectomy–secondary tenotomy because it first decreases with the substantial atrophy and then almost normalizes despite the retraction, which is comparable in the T/N and N/T groups. Thus, this experiment shows that retraction without a substantial increase in the pennation angle leads to less fatty infiltration than retraction without changes of the pennation angle. 6 This may explain that muscles that are much less pennate than the rotator cuff muscles show less fatty infiltration after tendon tear than the cuff muscles. 12,13
Surprisingly, myotendinous retraction of both groups was equally pronounced after 16 weeks. One would expect that a denervated muscle would have a lower tendency to retract: A denervated muscle is known to lead to increased atrophy, which leads to a reduction in the size of the pennation and a corresponding lengthening of the muscle fibers. This observation from previous studies 6 was confirmed in the N/T group after 8 weeks. These data suggest that in a combined situation of nerve injury and tendon tear such as after shoulder dislocation with associated massive cuff tear, tendon repair cannot wait, with the argument that a denervated muscle will not retract.
Our findings support the clinical relevance of avoiding additional suprascapular nerve traction during rotator cuff repair. There is no evidence in the literature as to whether release of the suprascapular nerve can improve the clinical outcome of patients after cuff repair, 16 but a benefit is not excluded in large revision cuff repairs. 11
Although the sheep model is common in rotator cuff research, our findings cannot directly be transferred into clinical practice. For ethical reasons, the study size cannot be increased arbitrarily and thus remains small with 12 animals (similar to a previous study 6 ), although the study size was reduced again because of the insufficient neurectomy in 3 animals. This may have resulted in a type 2 error, as possibly seen in the lack of significance regarding the different pattern of fatty infiltration. The neurectomy performed in this study is an attempt to simulate a chronic neuropathy of the suprascapular nerve, which otherwise cannot be reliably achieved in animal models. A single observer performed the MRI readouts, but the selected method has a documented, excellent intraobserver and interobserver correlation. 6
Conclusion
This study documented that sequential damage through neurectomy of a tenotomized musculotendinous unit increases muscle atrophy of the infraspinatus muscle in sheep, whereas neither secondary neurectomy nor secondary tenotomy influences the ultimate amount of fatty infiltration. It also showed that tenotomy of a denervated muscle does not further increase the muscle atrophy. In sheep, a denervated infraspinatus muscle was able to retract after tenotomy.
Footnotes
Final revision submitted January 3, 2021; accepted February 18, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by the Swiss National Science Foundation (grant 170040). C.G. has received royalties from Zimmer Biomet Holdings. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the regional ethics commission of Zürich Canton (No. 100/17).