
Abstract
Background:
There is disagreement as to whether early controlled motion and weightbearing confer a beneficial effect for nonoperatively treated acute Achilles tendon rupture (ATR) compared with immobilization and late weightbearing.
Purpose:
To conduct a meta-analysis of randomized controlled trials (RCTs) to determine whether early controlled motion and weightbearing results in different outcomes compared with immobilization and late weightbearing for nonoperatively treated patients with acute ATR.
Study Design:
Systematic review; Level of evidence, 1.
Methods:
We conducted a search in the PubMed, Web of Science, and EMBASE databases for relevant RCTs in humans from January 1981 to August 2020. The primary outcome was the Achilles Tendon Total Rupture Score (ATRS) at 1-year follow-up. The secondary outcomes were the rerupture rate, return to sports activity and work, and the heel-rise work (limb symmetry index [LSI]). Study quality was assessed using the Cochrane Collaboration risk of bias tool.
Results:
Included were 7 RCTs involving 424 participants (n = 215 treated with early controlled motion and weightbearing [early group], n = 209 treated with immobilization and late weightbearing [late group]). The quality assessment indicated a low risk of bias in all included RCTs. There was no difference between the early and late groups regarding the ATRS (mean difference [MD], -0.220; 95% CI, -4.489 to 4.049; P = .920). Likewise, we found no difference between the 2 groups in terms of the rerupture rate (odds ratio [OR], 1.107; 95% CI, 0.552 to 2.219; P = .775), the number of patients who returned to sports (OR, 0.766; 95% CI, 0.438 to 1.341; P = .351) and returned to work (OR, 0.706; 95% CI, 0.397 to 1.253; P = .234), the time to return to work (MD, -2.802 days; 95% CI, -6.525 to 0.921 days; P = .140), or the heel-rise work LSI (MD, -0.135; 95% CI, -6.243 to 5.973; P = .965).
Conclusion:
No significant differences were found between early controlled motion and weightbearing compared with immobilization and late weightbearing regarding the ATRS, the rerupture rate, return to sports activity and work, and the heel-rise work in nonoperatively treated patients with acute ATR.
Acute Achilles tendon rupture (ATR) is a common problem in foot and ankle surgery. The treatment is still controversial, and the main alternatives are either nonoperative or surgical. 4,5,17,18 During the past decade, surgical treatment has been regarded as the first choice in many hospitals. In addition, it has become common to add early functional controlled motion and weightbearing, such as using an adjustable brace, after surgical treatment. 6,22,23,26 Studies on treatment with only early functional controlled motion and weightbearing, using a mobile cast without any preceding surgery, also show promising results. 25,37 Animal studies in an unrepaired Achilles tendon model have shown faster and stronger tendon healing because of the release of growth factors with early controlled motion and weightbearing. 1,24 Clinical studies in surgically and nonsurgically treated Achilles tendon tears have also shown that early controlled motion could promote faster and better healing of the tendons. 11,35,39 Despite there being no statistically significant differences in functional outcomes, a trend toward better treatment outcome was found in studies both operatively and nonoperatively using early controlled motion and weightbearing. 33,40 This has led to the controversy that the early controlled motion of the ankle might be the key to the best treatment for both operatively and nonoperatively treated patients with acute ATR. 33,38,40
Early controlled motion might have beneficial effects. However, it has also been shown in an animal laboratory study on nonoperatively treated Achilles tears that early controlled motion can cause tendon elongation, 20 which leads to a decrease in humans’ push off strength, and thus a poor functional outcome. 14,32 However, 3 randomized controlled trials (RCTs) 15,27,30 found a tendency toward better push off strength and shorter rehabilitation in both operatively and nonoperatively treated patients with early controlled motion and weightbearing.
To our knowledge, no one has pooled the trials data in a meta-analysis to reconcile those differences. Therefore, we performed a systematic review and meta-analysis of RCTs to determine whether early controlled motion and weightbearing results in different outcomes compared with immobilization and late weightbearing in nonoperatively treated patients with acute ATR. The hypothesis was that there would be no significant differences between the treatment strategies.
Methods
Search Strategy and Criteria
Our study followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines and the PRISMA-IPD (individual patient data) statement. 21,34 We conducted a thorough search of peer-reviewed articles in the PubMed, Web of Science, and EMBASE databases to identify all RCTs comparing early controlled motion and weightbearing versus immobilization and late weightbearing for nonoperatively treated acute ATRs from January 1981 to August 2020. The keywords “Achilles tendon” and “rupture” were chosen, and the following terms were applied to the search in the 3 chosen databases: (Achilles AND (rupture OR ruptures OR tearing OR tears OR tear OR damage OR damages OR injury OR injuries)) OR (gilles AND (rupture OR ruptures OR tearing OR tears OR tear OR damage OR damages OR injury OR injuries)) OR (akilli AND (rupture OR ruptures OR tearing OR tears OR tear OR damage OR damages OR injury OR injuries). The results were limited to human RCTs and were published in all languages.
Initially, the retrieved articles were screened for relevance by the title and abstract. Articles that met the following criteria were included: (1) RCTs; (2) trials enrolling adults diagnosed with acute ATR; (3) trials that compared early controlled motion and weightbearing with immobilization and late weightbearing for nonoperatively treated acute ATRs; (4) trials that reported the Achilles Tendon Total Rupture Score (ATRS), the rerupture rate, return to sports activity and work, times to return to work, the heel-rise work, or other functional measures. Exclusion criteria were case-control studies, case reports, studies without abstracts, patient age <18 years, chronic Achilles tendinopathy, a history of previous injury or surgery to the same Achilles tendon and surgical treatment, and known inflammatory diseases (eg, rheumatoid arthritis, psoriatic arthritis, or inflammatory bowel). We also hand searched the bibliographies of the included trials as well as the conference proceedings and meeting abstracts. Only full-length published articles were included in this study.
Summary of Included Studies
Of the 8120 studies identified by our search, 7 studies 2,3,9,16,19,30,41 were included in the qualitative synthesis. Full-text articles that were excluded were those that related to tendinopathy rather than tendon tears, assessed muscle injuries, were duplicates, related to ligament injuries, or had surgical interventions (Figure 1). Studies were analyzed for control type as well as treatment type and technique. All included studies were RCTs that compared early controlled motion and weightbearing with immobilization and late weightbearing for nonoperatively treated acute ATRs. No included study performed early motion, but they performed delayed weightbearing.

The flow of information is shown through a systematic review for early controlled motion and weightbearing versus immobilization and late weightbearing in nonoperatively treated acute Achilles tendon ruptures.
Quality Assessment and Data Collection
The full-text articles were extracted by 1 reviewer (Y.-j.Z.) and checked by a second reviewer (J-y.D.). We assessed the risk of bias for all the included studies using the Cochrane risk of bias tool. 12,21 An additional quantification of the degree of possible bias was performed by the modified Coleman Methodology Score, 7 consisting of 10 criteria each scored from 0 to 10. A perfect score of 100 represents a study design that largely avoids the influence of chance, different biases, and confounding factors. 8 The level of evidence for all included studies was determined according to the Cochrane Handbook for Systematic Reviews of Interventions. 13
Data that were collected in this study included the number of patients, the mean age, the treatment procedure, and clinical outcomes. We defined early motion and weightbearing as that occurring within the first 4 weeks of treatment. The intervention group in 3 studies 9,19,41 was instructed to perform early controlled ankle motion and weightbearing immediately, 2 studies 2,16 from the first day, and another 2 studies 3,30 after 2 weeks. The control group in all 7 studies was instructed to perform immobilization and nonweightbearing at least for 4 weeks.
Study Outcomes
The primary outcome assessed was the ATRS at 1-year follow-up visit. The ATRS is the only patient-reported outcome measure developed and the validated patient-reported instrument with high reliability, validity, and sensitivity for measuring the outcome related to symptoms and physical activity after treatment in patients with a total ATR. 29 This 100-point scale was scored using identical questionnaires and in an identical setting as at 1-year follow-up. 2 The initial study was designed with a sample size with sufficient power to detect a difference in the ATRS of 10 points and a power of 0.9 (2-sided). 2
The secondary outcomes were the rerupture rate, the number of patients who returned to sports activity and work, and heel-rise work (reported as limb symmetry index [LSI]). The mean time to return to work was also calculated. The heel-rise work was measured as described by Silbernagel et al 31 and Nilsson-Helander et al 28 and reported as an LSI ([injured limb/healthy limb] × 100%). A muscle lab test unit (Ergotest Technology) was used for the data acquisition. Standardized instructions were given to patients, including a 5-minute warm-up on a low-load stationary bicycle, followed by 3 sets of ten 2-legged toe raises. The uninjured side was tested first.
It was possible to conduct a meta-analysis of the ATRS, the rerupture rate, return to sports activity and work, and the heel-rise work. Other functional measures that were used by different studies included tendon strength, quality of life during treatment, and ankle range of motion; we have presented the results of these outcomes separately. The results of the last follow-up examination included in the RCTs were used when possible.
Statistical Analysis
A statistical analysis was performed using STATA Version 12 (Stata Corp). Continuous variables were analyzed using the weighted mean difference (MD), and categorical variables were assessed using relative risks. In this study, P < .05 was statistically significant and 95% CIs were reported. A funnel plot and the Egger test were performed for any publication bias of the pooled results of the ATRS in the meta-analysis. The results of the funnel plot suggested that no publication bias was present (Figure 2), which was also statistically supported by the Egger test (P = .920). Heterogeneity among trials was assessed using the I 2 test statistic (0.50% is considered having substantial heterogeneity). A random-effects model was used if the I 2 value was statistically significant; otherwise, a fixed-effects model was used. In this meta-analysis, there was no heterogeneity in the ATRS (chi-square = 0.27; P = .966; I 2 = 0%), the rerupture rate (chi-square = 1.26; P = .974; I 2 = 0%), return to sports activity (chi-square = 1.06; P = .901; I 2 = 0%), return to work (chi square = 1.78; P = .776, I 2 = 0%), the time to return to work (chi-square = 1.58; P = .664; I 2 = 0%), and the heel-rise work (chi-square = 0.94; P = .626; I 2 = 0%); and a fixed-effects model was used.

The funnel plot with pseudo 95% confidence limits of the Achilles Tendon Total Rupture Score suggested that there was no publication bias, which was also statistically supported by the Egger test (P = .920). WMD, weighted mean difference.
Results
All 7 included studies were RCT studies with low risk of bias and high modified Coleman Methodology scores (>80) (Table 1). A total number of 424 patients were enrolled in the meta-analysis, including 215 patients who underwent early controlled motion and weightbearing (early group) and 209 patients who underwent immobilization and late weightbearing (late group). The mean age between these 2 groups was similar; however, overall there were fewer women than men. The length of follow-up ranged from 3 months to 4.5 years. The detailed demographic characteristics of the included studies are presented in Table 2.
Quality Assessment of Included Studies a
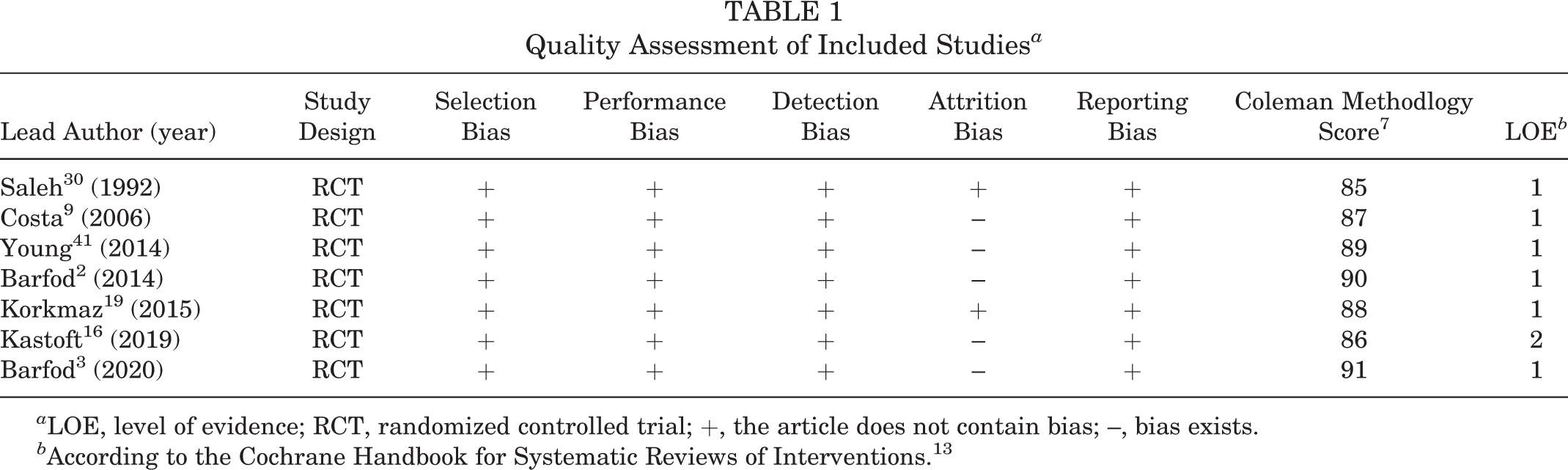
a LOE, level of evidence; RCT, randomized controlled trial; +, the article does not contain bias; –, bias exists.
b According to the Cochrane Handbook for Systematic Reviews of Interventions. 13
Demographic Characteristics of the Included Studies a

a All studies were randomized controlled trials comparing early controlled motion and weightbearing (early group) with immobilization and late weightbearing (late group). AOFAS, American Orthopaedic Foot & Ankle Society; ATRS, Achilles Tendon Total Rupture Score; EuroQol, European Quality of Life; NA, not available; PAS, Physical Activity Scale; ROM, range of motion.
Study Outcomes
There was no difference between the early and late groups regarding the primary outcome in the 4 studies 2,3,16,19 that reported the ATRS (76.2 ± 18.3 [early group] vs 76.6 ± 18.6 [late group]; MD, -0.220; 95% CI, -4.489 to 4.049; P = .920) (Figure 3). There was also no difference between the early and late groups in terms of tendon rerupture rate (7 studies 2,3,9,16,19,30,41 ; odds ratio [OR], 1.107; 95% CI, 0.552 to 2.219; P = .775) (Figure 4), the number of patients who returned to sports activity (5 studies 2,3,9,16,30 ; OR, 0.766; 95% CI, 0.438 to 1.341; P = .351) (Figure 5), or the number of patients who returned to work (5 studies 2,3,16,19,41 ; OR, 0.706; 95% CI, 0.397 to 1.253; P = .234) (Figure 6). In 4 studies 2,3,19,41 that reported the time to return to work, the MD between the early and late groups was -2.802 days, which was not significantly different (56.6 ± 70.9 days [early group] vs 52.3 ± 45.1 days [late group]; 95% CI, -6.525 to 0.921; P = .140) (Figure 7). Finally, we found no difference between the early and late groups in terms of the heel-rise work in 3 studies 2,3,16 (58% ± 22.1% [early group] vs 58.0% ± 24.5% [late group]; MD, -0.135; 95% CI, -6.243 to 5.973; P = .965) (Figure 8).

Forest plot of the ATRS in patients treated with early controlled motion and weightbearing versus immobilization and late weightbearing. There was no heterogeneity in the ATRS (chi square = 0.27; P = .966; I 2 = 0%) and a fixed-effects model was used. ATRS, Achilles Tendon Total Rupture Score; WMD, weighted mean difference.
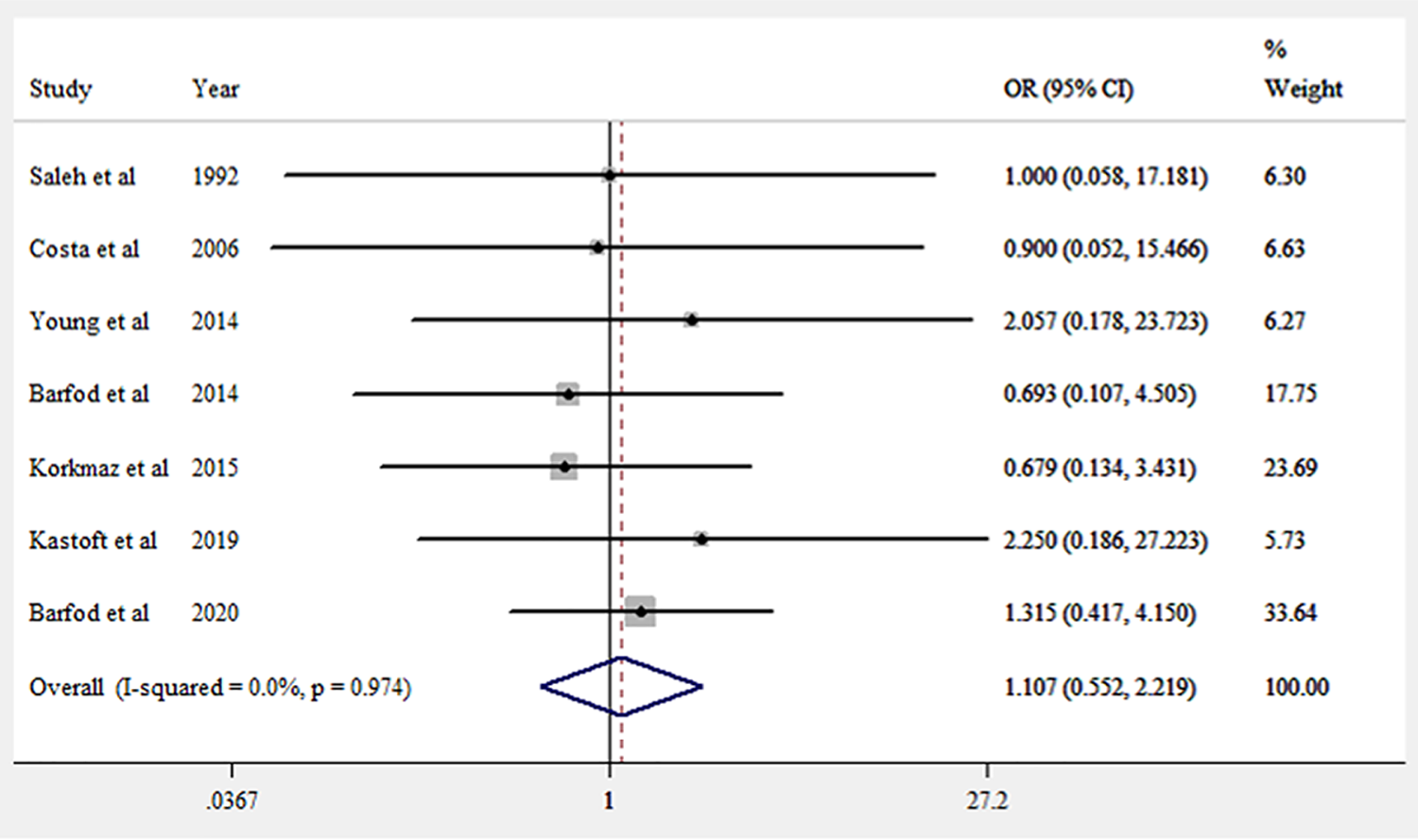
Forest plot of tendon rerupture rate in patients treated with early controlled motion and weightbearing versus immobilization and late weightbearing. No significant heterogeneity was found in the tendon rerupture rate (chi square = 1.26; P = .974; I2 = 0%), and a fixed-effects model was used. OR, odds ratio.
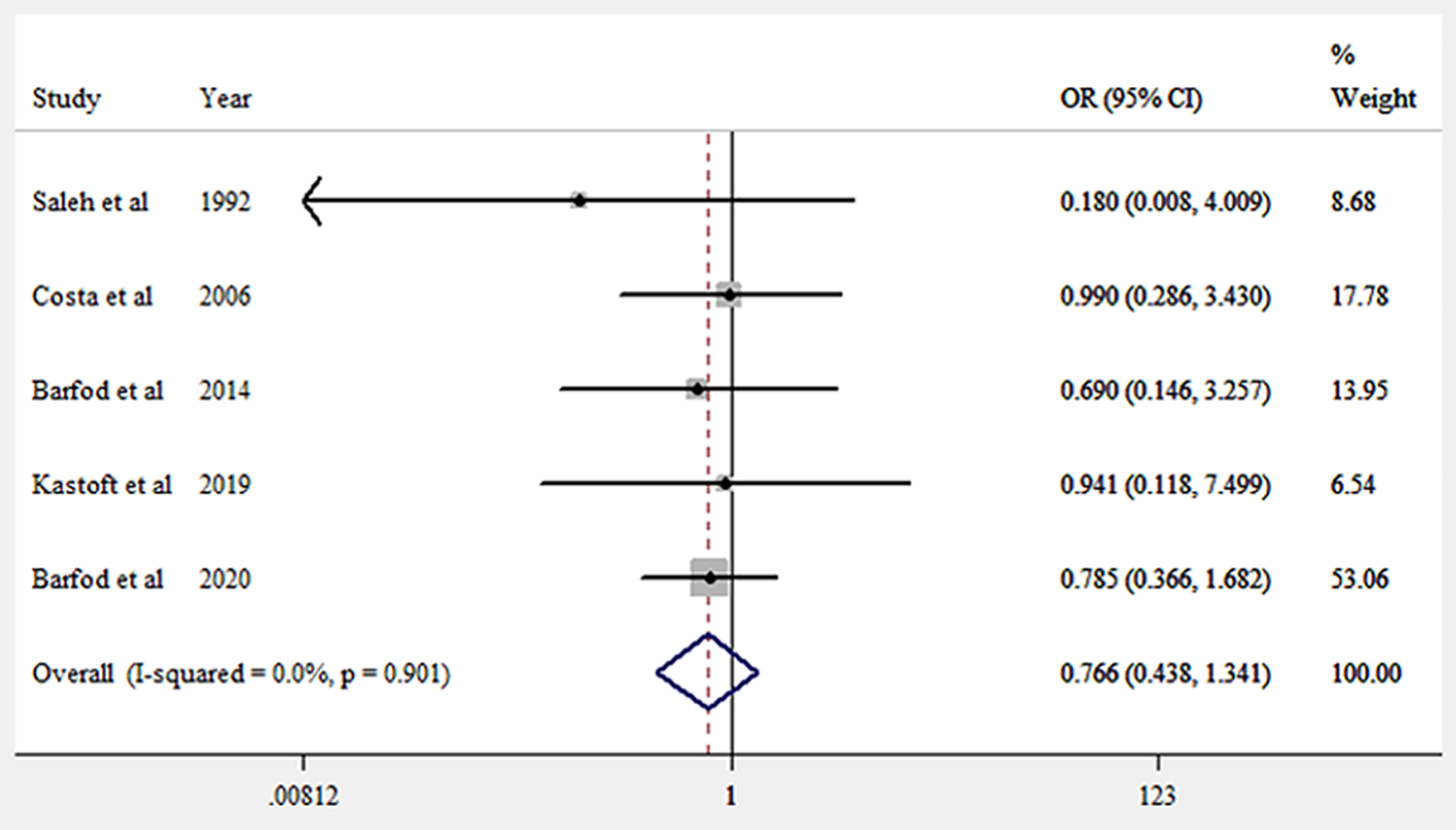
Forest plot of return to sports activity in patients treated with early controlled motion and weightbearing versus immobilization and late weightbearing. No significant heterogeneity was found in the number of return to sports activity (chi square = 1.06; P = .901; I2 = 0%), and a fixed-effects model was used. OR, odds ratio.

Forest plot of return to work in patients treated with early controlled motion and weightbearing versus immobilization and late weightbearing. No significant heterogeneity was found in the number of return to work (chi square = 1.78; P = .776; I2 = 0%), and a fixed-effects model was used. OR, odds ratio.

Forest plot of time to return to work in patients treated with early controlled motion and weightbearing versus immobilization and late weightbearing. No significant heterogeneity was found in the number of return to work (chi square = 1.58; P = .664; I2 = 0%), and a fixed-effects model was used. WMD, weighted mean difference.

Forest plot of the heel-rise work in patients treated with early controlled motion and weightbearing versus immobilization and late weightbearing. No significant heterogeneity was found in the heel-rise work (chi square = 0.94; P = .626; I2 = 0%), and a fixed-effects model was used. WMD, weighted mean difference.
Other Outcomes
Two studies 2,16 evaluated the heel-rise height and found no significant difference between the early and late groups. One study 41 reported no significant difference in tendon isokinetic strength between the 2 groups. Two studies 19,41 reported the subjective outcomes of the Leppilahti questionnaire, Tegner ankle scores, the self-rated Achilles tendon score, the American Orthopaedic Foot & Ankle Society ankle-hindfoot score, and the Physical Activity Scale. Fewer patients in the early group reported pain, stiffness, or weakness at 1 year. 41 However, apart from the subjective stiffness rating, none of these differences were statistically significant. One study 30 reported the results of ankle plantarflexion increasing not significantly between the 2 groups, with dorsiflexion increasing significantly in the early controlled motion and weightbearing group (P < .001). In the early controlled motion and weightbearing group, almost normal dorsiflexion was achieved by 6 months. Other complications were pulmonary embolism, no signs of tendon healing and tendon elongation. 3,9,41
Discussion
In this meta-analysis, the most important result was that no statistically significant difference was found between early controlled motion and weightbearing and immobilization and late weightbearing in nonoperatively treated patients regarding the ATRS, the rerupture rate, return to sports activity and work, and the and heel-rise work with the numbers available.
Four of the included studies 2,3,16,19 had reported that the ATRS increased significantly from 6 to 12 months in both groups. However, in this meta-analysis, we found no significant differences between early controlled motion and weightbearing over immobilization and late weightbearing with respect to ATRS, despite having adequate statistical power to detect a clinically important difference in the ATRS.
The rate of rerupture has been the commonly used outcome in research regarding treatment of Achilles tendon rupture. A previous study reported that early weightbearing increased the force on the Achilles tendon, which could potentially lead to elongation or rerupture of the healing tendon. Use of the orthotic heel lift reduces the Achilles tendon force and the resulting strain while allowing for isometric contraction. 10 In this meta-analysis, the pooled rerupture rate was 7.9% in the early group and 8.6% in the late group. However, there was no significant difference in these 2 groups, indicating that early controlled motion and weightbearing may not increase the risk of rerupture rate during the treatment period of acute ATR.
Regarding the return to sports activity and work as a secondary outcome, we found no statistically significant difference between the 2 groups based on 5 studies 2,3,16,19,41 and confirmed that the individual result from each study showed no significant difference. In addition, great variation existed in the individual incidence of return to sports in each study, which depends on how to define a return to sports. For example, Barfod et al 2 reported 18% of patients, and Costa et al 9 56% of patients, as having returned to sports in the early controlled motion and weightbearing group at 1-year follow-up. Previous studies have shown 30% to 60% return to the same level of sports activity in both operatively and nonoperatively treated patients. 5,26 Two studies 3,19 reported on the times required to return to work and showed no statistically significant difference. However, they did not report the type of work. Young et al 41 reported that the type of work was similar in both groups, and Barfod et al 2 divided work into 3 types, including heavy, light, and sedentary. It seemed that the early weightbearing group included more heavy and light types of employment when compared with the late weightbearing group. 2,41 Three studies 2,3,16 had reported that the heel-rise work and height had no significant differences between early controlled motion and weightbearing and immobilization and late weightbearing groups, although Kastoft et al 16 found that the heel-rise height was significantly higher in the early controlled motion and weightbearing group at 6 months, but it was equalized at 1 year.
One study 2 noted that health-related quality of life during the first 8 weeks of treatment appeared to be better in the early controlled motion and weightbearing group. This is in line with the conclusion of Suchak et al 36 that early weightbearing provides enhanced quality of life. 36 However, the authors indicated that the result should be interpreted with caution, as health-related quality of life was measured with use of a custom-designed measure with unknown validity and reliability. One study 30 reported that the increased range of plantarflexion in the early controlled motion and weightbearing group at 3 and 6 months was not statistically significant, but the increased range of dorsiflexion in the early controlled motion and weightbearing group at 3, 6, and 12 months was highly significant (P < .001). They concluded that ankle dorsiflexion rehabilitation is faster without overstretching, and return to sports activities is more rapid with early controlled motion and weightbearing. One study 41 reported the subjective outcomes, including the scores for the subjective section of the Leppilahti questionnaire, Tegner ankle scores, and self-rated Achilles tendon scores were slightly more favorable in the early controlled motion and weightbearing group, but not significantly so. Therefore, we would recommend to allow early motion and weightbearing because that early motion may minimize problems with stiffness without increasing the rerupture rate or affecting outcomes.
This study has several limitations. First, the sample size was small. Seven RCTs involving only 424 participants were eligible for inclusion, with 215 participants in the early controlled motion and weightbearing group and 209 in the immobilization and late weightbearing group. The power calculation in the present study was based on a standard deviation of 10 points in the ATRS, as reported by Nilsson-Helander et al. 28 However, the actual standard deviation in the meta-analysis study was 16, which should be taken into consideration when utilizing the ATRS as the primary outcome. There might be small but still clinically important treatment benefits, and the size of the meta-analysis we conducted may not have sufficient power to detect this benefit. Second, the studies in this meta-analysis included few competitive elite athlete patients from the general population, and there were fewer women in the study groups. Moreover, physicians often choose surgical repair in higher demand patients. Therefore, there is likely some selection bias. Third, we chose not to focus on different types of orthoses used in individual studies but rather on the time interval until full weightbearing. Fourth, the included studies also used different definitions of early motion and different types of casts. Therefore, we could not rule out the existence of confounding factors stratified by mobilization period and cast type, but we did not believe that they exist.
In conclusion, no significant differences were found between early controlled motion and weightbearing and immobilization and late weightbearing regarding the ATRS, the rerupture rate, return to sports activity and work, and the heel-rise work in nonoperatively treated patients with acute ATR. Larger randomized controlled studies are needed to confirm these outcomes.
Footnotes
Acknowledgment
The authors thank Dr Yang Lu for writing assistance.
Final revision submitted February 3, 2021; accepted February 28, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by Zhejiang Province Public Welfare Technology Application Research Project (CN) (LGF21H060007). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.