
Abstract
Background:
Reports of anterior cruciate ligament (ACL) injury in patients with skeletal immaturity have been increasing. Variations in knee joint anatomy have been linked to ACL injury risk factors.
Purpose:
To identify associations between ACL injury, patella alta, and femoral trochlear dysplasia in patients with skeletal immaturity by using magnetic resonance imaging (MRI).
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
This retrospective study included 231 patients with skeletal immaturity—116 with acute complete noncontact ACL injury and 115 without ACL injury (controls)—who underwent knee MRI. Cases of femoral trochlear dysplasia were divided into 4 types according to the Dejour classification scheme. Patellar height and patellar tendon length were measured via sagittal MRI, and the Insall-Salvati ratio (ISR) was calculated.
Results:
In the ACL injury group, 56 (48.3%) knees exhibited trochlear dysplasia, including 51 (91.1%) that were Dejour type A; and in the control group, 12 (10.4%) knees exhibited trochlear dysplasia, 12 (100%) Dejour type A. The prevalence of femoral trochlear dysplasia was significantly higher in the ACL injury group than in the control group (P < .001). The ISR was not significantly different between the ACL injury and control groups (0.9 ± 0.2 vs 1 ± 0.2 mm; P = .16). The correlation between ISR >1.2 and presence of ACL injury was not significant.
Conclusion:
Femoral trochlear dysplasia was associated with ACL injury in patients with skeletal immaturity. In particular, Dejour type A femoral trochlear dysplasia was correlated with ACL injury patients with skeletal immaturity. Also, the possibility of ACL damage exists in patients with skeletal immaturity and femoral trochlear dysplasia.
The occurrence of injuries to the anterior cruciate ligament (ACL) has been increasing in the pediatric population. 8 In particular, the ACL is the most frequently injured ligament of the knee joint and is involved in 50% of all knee joint injuries. 22 In general, anatomical parameters, including intercondylar notch width, ACL size, ligamentous laxity, tibial slope, and the Q angle of the ACL, are key risk factors when assessing ACL injury. 12,23,24 Patellar dislocation and ACL injury are common events and can result in major damage unless treated appropriately. The mechanism of injury is similar to that of a valgus twisting injury and is attributed to sudden noncontact deceleration. 5 Individuals at risk of ACL injury also share similar epidemiological and anatomical characteristics. 5 Female patients tend to present greater ligamentous laxity; and younger, more active adults often show intercondylar notch and trochlear notch dysplasia. 5 In addition, patellofemoral (PF) instability is a clinical syndrome caused by morphological abnormalities in the PF joint and, it has been shown to interfere with knee extension and flexion, contributing to ACL damage. 6,18
Two of the major anatomical phenomena that cause patellar instability are femoral trochlear dysplasia and patella alta. 1 To date, available research on the correlation between ACL injury and these 2 phenomena remains limited. Botchu et al 2 reported that Dejour type A trochlear dysplasia is associated with ACL injury. 2 Meanwhile, Chen et al 3 determined the association between femoral trochlear dysplasia and ACL injury by comparing postoperative computed tomography data of patients with ACL injury against those of patients without ACL injury, finding that femoral trochlear dysplasia might be a significant risk factor for ACL injury.
In the literature, only 2 studies have examined the relationship between ACL injury and the 2 aforementioned anatomical phenomena. 1,18 Ntagiopoulos et al 18 reported increased prevalence of trochlear dysplasia and patella alta in patients with ACL injury relative to the incidence of femoral trochlear dysplasia and patella alta in the general population. However, there was no significant correlation between femoral trochlear dysplasia and ACL injury in adult patients. Another study, performed using magnetic resonance imaging (MRI) in adult patients, found that the 2 anatomical phenomena may be risk factors for ACL injury. 1
To the best of our knowledge, no studies have discerned the correlation between ACL injury and the 2 anatomical phenomena using MRI in patients with skeletal immaturity. Therefore, we researched the associations between ACL injury and patella alta and femoral trochlear dysplasia in patients with skeletal immaturity by using MRI. We hypothesized that there would be a correlation between ACL injury and either patella alta or femoral trochlear dysplasia in patients with skeletal immaturity.
Methods
The patients with skeletal immaturity included in this study were retrospectively selected from among children, aged 3 to 18 years, who presented with knee pain, and who underwent clinical MRI from 2004 to 2020 at our institution. The study design was approved by our institutional review board.
A case-control study design was adopted to minimize potential confounding variables that could be associated with the 2 anatomical phenomena and ACL injury. Patients eligible for inclusion in the ACL injury group were skeletally immature consecutive pediatric patients with preoperative MRI scans available from our institutional database. The official radiology report was used to confirm the definite presence of ACL tears, and we included patients with both clinical and radiologic findings available. Exclusion criteria were evidence of intra-articular injury that precluded measurement of chondral anatomy or the presence of concomitant injuries to other ligaments.
A control group was retrospectively established from among pediatric patients matched by age and sex, with MRI scans that showed no ACL injury. Those with deformed bony structures caused by bone tumors, physeal arrest, osteochondral fracture, or any previous surgery were excluded from this study. MRI scans were acquired using a 3.0-T MRI scanner (Philips Medical Systems) with a 3-dimensional proton density volume isotropic turbo spin-echo acquisition sequence, which is a useful modality with which to observe ligaments and cartilage in the joints. Imaging was performed with a 1400 ms repetition time, 33 ms echo time, 0.5 mm slice thickness, 160 mm field of view, 90° flip angle, 320 × 320 matrix, and 357 Hz/pixel bandwidth. The PF joint parameters were measured using the Mimics Version 17.0 software program (Materialise).
The diagnosis of dysplasia type was made based on the Dejour classification, 14 which stratifies dysplasia as types A through D. All these types involve a crossing sign, which is an intersection between the condylar trochlear and trochlear grooves. Presence of the crossing sign has a high sensitivity (94%) but a relatively low specificity for diagnosis of dysplasia. 9 For this reason, the type shapes are also used as diagnostic criteria. Type A dysplasia is characterized by a shallow trochlea (>145°), type B involves a flat trochlea, type C encompasses medial hypoplasia, and type D includes a cliff. MRI was used to determine Dejour dysplasia type (Figure 1).

Dejour classification of trochlear dysplasia.
In addition, the Insall-Salvati ratio (ISR) was adopted to determine patellar height (Figure 2). The ISR was measured using MRI, where values >1.2 are indicative of patella alta. 13 Two independent observers (Y.H.K. and Dr. Gihun Kim), both orthopaedic surgeons who were blinded to patient medical history, individually assessed the Dejour classification and the presence of patella alta. To determine the intraobserver reliability, measurements in 50 randomly selected patients were repeated 1 month later. The intraobserver and interobserver reliability values of the ISR measurement were 0.93 and 0.88, respectively, calculated using the intraclass correlation method. The intraobserver and interobserver reliability values of the Dejour classification were 1 and 0.71, respectively, calculated using the Cohen kappa. 17

Schematic representation of the Insall-Salvati ratio: A/B, where A is the length of the patellar tendon and B is the maximum length of the patella. 1
Statistical Analysis
The Student t test was chosen to examine significant differences between the mean values of the study groups. The chi-square test was selected to analyze the difference between categorical variables. The significance level was set at P < .05.
A post hoc power analysis was performed. The calculated power was 99.9%, which is higher than the target power (80%) of previous research. 16 Statistical analysis was performed using the Statistical Package for the Social Sciences Version 22 (IBM Corp).
Results
We reviewed 297 MRI scans, comprising those of 115 patients who met the inclusion criteria for the control group and 116 patients in the ACL injury group. The mean age of patients in the ACL injury and control groups was 14 ± 3.7 and 14.2 ± 3.6 years, respectively (Table 1). There were no significant differences in age or sex between the 2 groups.
Comparison of the Age and Gender Ratio Between Korean Pediatric Patients With and Without ACL Injury a

a Data are reported as mean ± SD (range) or No. ACL, anterior cruciate ligament; NA, not applicable.
The prevalence of femoral trochlear dysplasia was significantly higher in the ACL injury group than in the control group (P < .001).
Among the 56 patients with femoral trochlear dysplasia in the ACL injury group, 51 had type A, 3 type B, 1 type C, and 1 type D dysplasia. In contrast, all control group patients had the Dejour type A femoral trochlear dysplasia (Table 2).
Comparison of the Number of Dejour Types Between the ACL Injury and Control Groups a
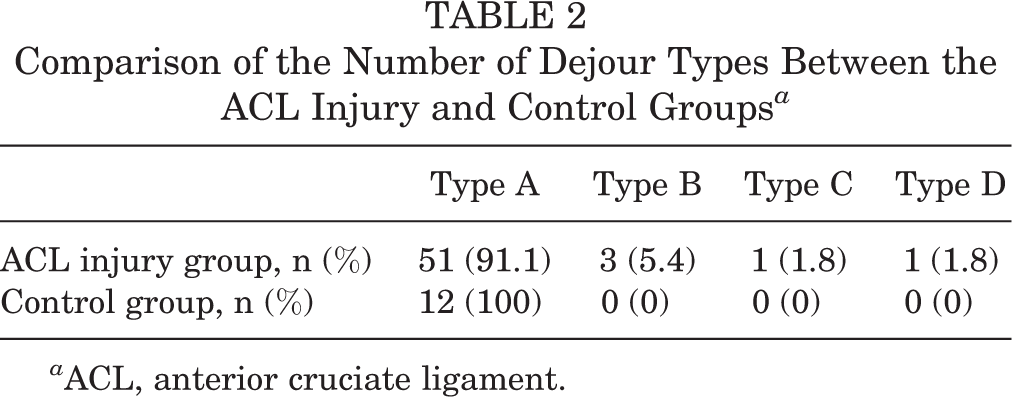
a ACL, anterior cruciate ligament.
The ISR was not significantly different between the ACL injury and control groups (0.9 ± 0.2 vs 1 ± 0.2 mm; P = .16). In the ACL injury group, 10 knees (8.6%) had ISR values >1.2, indicating patella alta (P < .05). In the control group, 10 knees (8.7%) had ISR values >1.2, indicating patella alta (P < .05). However, the correlation between ISR index >1.2 and presence of ACL injury was not significant (P ≥ .99).
Discussion
The most important finding of this study is that femoral trochlear dysplasia was associated with ACL injury in skeletally immature patients and the most common of all knee dysplasias in our groups. In addition, Dejour type A femoral trochlear dysplasia was associated with ACL injury in skeletally immature patients. However, the patella alta index was not significantly different between the ACL injury and control groups. In particular, the correlation between patella alta index >1.2 and presence of ACL injury was not significant. Therefore, our hypothesis was only partially accepted.
ACL injuries are becoming more prevalent in pediatric populations, which may be the result of more frequent organized sports among boys and girls and could be linked to greater levels of competition. 8 Identifying the risk factors for ACL injury to the knee can help reduce its occurrence. One anatomical factor that has been subject to considerable debate is the morphology of the femoral trochlear dysplasia and patella alta. 1 –3,18 To date, there is little literature on the clinical associations between ACL injury and these 2 anatomical phenomena. In patients with femoral trochlear dysplasia, the proximal femoral trochlear joint surface becomes flat, and distal irregularities appear less pronounced. 7 In more severe cases, as the hypoplasia of the medial joint surface increases, the femoral trochlear joint surface may become convex. 7 The involvement of normal femoral trochlear anatomy is essential for the biomechanics of knee flexion and extension. In addition, femoral trochlear dysplasia may increase ACL loading in partially flexed knees because of defects in the extensor mechanism. 19 Malignant tracking of the PF joint with subluxation of the patella may also occur. The stress mainly affects the side of the patella, which increases disproportionately and causes degeneration of the patellar cartilage. 4
Only 2 studies have previously examined these 2 anatomical phenomena. 1,18 Ntagiopoulos et al 18 took measurements from radiographs that had been obtained with knees positioned in standardized 30° of flexion. 18 Another study was performed using MRI but included only adult participants. 1 MRI provides a more accurate bony morphology for measurement of the 2 anatomical phenomena, especially in the pediatric population. In addition, MRI has several benefits over both radiography and computed tomography, including no need for radiation exposure and the ability to reveal cartilage defects and muscle and ligament injuries. 10, 21 Although Stepanovich et al 25 found that the Dejour classification of pediatric patients using MRI has low reliability, the intraobserver and interobserver reliability of our study were 1 and 0.71, respectively. Therefore, we chose MRI, a more sophisticated modality than radiographs and we were able to obtain direct measurements of both femoral trochlear dysplasia and patella alta.
Botchu et al 2 found a significant correlation between Dejour type A trochlear dysplasia and ACL injury in adults. 2 This trend is also found in previous research 18 ; however, Botchu et al examined only the ACL injury group and did not include a control group.
There have been different rates of femoral trochlear dysplasia among studies. In the studies of Botchu et al, 2 Ntagiopoulos et al, 18 Chen et al, 3 and Akgün and Agirman, 1 the percentages were 61%, 48%, 30%, and 15%, while this was 48% in our study. Individual morphometric characteristics are associated with genetic, environmental, and cultural conditions as well as lifestyle, health, and functional status. 15 Therefore, these variations can complicate development of a standard or interpretation of values that are considered “typical.” 15 However, as shown in previous studies, Dejour type A trochlear dysplasia accounted for the most prevalent finding in our study. 1 –3,18 In addition, the prevalence of femoral trochlear dysplasia was significantly higher among patients with an ACL injury in our study. This was similar to 2 previous studies in which ACL injury was correlated with femoral trochlear dysplasia. 1,3 Therefore, we surmise that femoral trochlear dysplasia is associated with an ACL injury.
In terms of patella alta, the degree of flexion needs to be higher for the patella to engage with the femoral trochlea compared with a healthy knee. This causes contact stress between the femoral trochlea and patella and can lead to greater tension or tearing of the ACL. 11 However, the mechanism of injury has not been established clearly, and some studies have reported the simultaneous rupture of the ACL and the patellar tendon. 1 Our study showed that the ISR was not significantly different between the ACL injury and control groups. Among the various methods that measure patella alta, the ISR method was used because the true patellar tendon lengths could be measured using sagittal MRI. 20 In addition, the correlation between ISR index >1.2 and presence of ACL injury was not significant. This is different from the results of Akgün and Agirman, 1 who reported increased patellar tendon lengths and ISR values in patients with ACL injuries compared with healthy controls. However, their results showed that the difference in the ISR value between the ACL injury group and the control group was only 0.03. Although the standard deviation was small, there was statistical significance; however, it is difficult to conclude that this is a clinically significant difference. Further, although there was a difference between their results and ours, Akgun and Agirman reported an 8.1% prevalence of patella alta and reported it as a possible risk factor for ACL injury. Our result for prevalence of patella alta was quite similar at 8.6%. Elsewhere, Ntagiopoulos et al 18 showed that the correlation between Caton-Deschamps index >1.2 and presence of trochlear dysplasia was not significant.
Our results highlight the importance of assessing for anatomic characteristics that may affect the injury pattern. We believe that femoral trochlear dysplasia meaningfully changes the knee biomechanics, increasing the risks of ACL loading and injury in skeletally immature patients. However, in the case of patella alta, further research is needed to determine whether it is a risk factor for ACL injury.
There are several limitations to the present study. First, only Korean pediatric patients were examined; future investigations should include other populations from the Asia-Pacific to establish a general database for this region. Second, patients were matched for age and sex but not for height, weight, or activity level. Third, the design of this study was retrospective, although it would be difficult and expensive to prospectively image and follow up uninjured patients in anticipation of ACL injury. Fourth, the anatomical structure directly related to trochlear dysplasia and ACL injury, such as intercondylar notch, was not measured. Finally, the study cases were selected from a single institution and the sample size was small. Further research is needed to determine whether the coexistence of patella alta and femoral trochlear dysplasia can constitute a risk factor for ACL injury.
Conclusion
Our results showed that the prevalence of femoral trochlear dysplasia was higher among patients with ACL injuries, and the morphological differences between pediatric patients with and without ACL injury indicated that femoral trochlear dysplasia is associated with ACL injury in skeletally immature patients. In particular, Dejour type A femoral trochlear dysplasia was correlated with ACL injury in skeletally immature patients. In the case of skeletally immature patient with femoral trochlear dysplasia, the possibility of ACL damage exists; thus, it is necessary to screen this and receive rehabilitation, such as reinforcement of the extensor mechanism, to reduce the possibility of ACL damage.
Footnotes
Final revision submitted January 24, 2021; accepted February, 24, 2021.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Severance Hospital (No: 4-2020-0962).
Acknowledgment
The authors wish to thank Gihun Kim for his great help with initial data acquisition.