
Abstract
Background:
Interposition grafting (IG), also called bridging grafting, and superior capsular reconstruction (SCR) are the most commonly used joint-preserving surgical methods for irreparable rotator cuff tears (RCTs).
Purpose:
To compare the effectiveness of IG versus SCR to treat patients with irreparable RCTs.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A literature search was performed in MEDLINE, Embase, and Scopus. Included in this review were clinical studies evaluating the effect of IG or SCR in patients with irreparable RCTs with a minimum follow-up of 1 year. Various clinical results from the studies were extracted and compared between IG and SCR, and among them, the results of the American Shoulder and Elbow Surgeons score, graft retear rate, and complication rate were included in the meta-analysis.
Results:
Of 1638 identified articles, 17 (10 studies of IG involving 321 patients and 7 studies of SCR involving 357 patients) were selected. Both surgical methods showed significantly improved clinical outcomes in all but 1 study; however, the IG group had lower pain visual analog scale score, higher Constant score, and bigger active forward flexion and internal rotation compared with the SCR group (all P < .001). The meta-analysis showed no difference in the American Shoulder and Elbow Surgeons score between groups (P = .44), but showed a significantly lower complication rate in the IG group compared with the SCR group (1.12% vs 8.37%, respectively; P < .001). The graft retear rate was not significantly different between groups (IG = 10.64% vs SCR = 12.67%; P = .79). The meta-analysis of graft type indicated no difference between groups in retear rate (autograft: 95% CI, 0.045-0.601; I 2 = 93.28 [IG], 91.27 [SCR]; P = .22; allograft: 95% CI, 0.041-0.216; I 2 = 80.39 [IG], 69.12 [SCR]; P = .64) or complication rate (autograft: 95% CI, 0.009-0.150; I 2 = 0 [IG], 65.89 [SCR]; P = .25; allograft: 95% CI, 0.012-0.081; I 2 = 0 [IG], 30.62 [SCR]; P = .09).
Conclusion:
Both IG and SCR techniques resulted in improvement in patients with irreparable RCTs. Meta-analysis showed a lower complication rate in the IG group; however, the lack of randomized studies limited our conclusions.
Keywords
Rotator cuff tear (RCT) is one of the most commonly diagnosed diseases in orthopaedics. Recently, the techniques and instrumentation used for surgical repair of torn rotator cuffs have rapidly improved, and the clinical and functional outcomes of rotator cuff repair have been satisfactory. 2,25 Nevertheless, large to massive RCTs are still a formidable and challenging problem, 18,26,43 and in some large to massive RCTs, the direct repair of the native rotator cuff tendons to the footprint of the greater tuberosity is impossible, even after adequate release, because of retraction, attenuation, and inelasticity of tendons. 4
Many surgical procedures have been introduced for the treatment of irreparable RCTs: arthroscopic debridement, 27 tuberoplasty, 16,54 partial repair, 3 interposition grafting (IG), 41,46 superior capsular reconstruction (SCR), 34 tendon transfers, 15,17 reverse total shoulder arthroplasty, 6,39,50 and arthrodesis. 11 Among these surgical procedures, IG and SCR are 2 of the most commonly performed. During IG, a patch graft is used to bridge the gap between the torn tendon and the footprint, for a tension-free repair 35 ; in SCR, joint function and stability are restored by reconstructing the superior capsule. 1 In both methods, the lateral margin of the graft is attached on the footprint of the greater tuberosity, but the difference is that the medial end of the graft is attached to the torn tendon end in IG and to the superior glenoid in SCR.
Studies have shown that both these methods lead to satisfactory results, with good pain relief and improved function. 9,29,40,47 However, to our knowledge, there have been no original articles that directly compared the clinical outcomes of IG and SCR. Most studies have evaluated the technique and outcomes of IG or SCR separately, without a control group or a randomized design. There have been only 2 systematic reviews comparing IG and SCR, 30,55 and they lacked meta-analyses of the clinical outcomes, graft retear rates, and complication rates.
The purpose of this study was to comprehensively compare the clinical outcomes of the IG and SCR procedures for irreparable RCTs and include a meta-analysis. We hypothesized that IG, which preserves active rotator cuff muscle function and strength, would show better clinical outcomes and lower graft retear and complication rates compared with SCR.
Methods
Identification and Selection of the Literature
This systematic review and meta-analysis followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 36 A systematic search of the literature in the MEDLINE, Embase, and Scopus databases using controlled vocabulary and keywords was conducted by 2 authors (S.B. and M.H.S.) on March 14, 2020. In addition, the reference lists of retrieved studies and previous literature reviews were manually screened. The detailed search terms were as follows: (1) (irreparable rotator cuff AND (tear OR injury OR repair) AND (interposition OR bridging)) and (2) (irreparable rotator cuff AND (tear OR injury OR repair) AND (superior capsular OR superior capsule)). There was a time limitation between 2000 and 2020 for the publication date.
Eligibility Criteria
The inclusion criteria were as follows: (1) irreparable RCT, which is the inability to suture the rotator cuff back to the footprint at ≤60° of abduction without undue tension despite adequate release, 12,53 (2) clearly defined procedures of IG or SCR used, (3) clinical outcomes measured at least 1 year postoperatively, (4) postoperative radiographic outcomes at a minimum of 1 year after surgery, (5) published in English-language, peer-reviewed journals, and (6) full text of studies available. The exclusion criteria were as follows: (1) nonclinical studies (eg, animal, biomechanical, basic science, and cadaveric studies), (2) expert opinions or review articles, (3) level 5 studies as designated according to the Oxford Centre for Evidence-Based Medicine, 42 and (4) studies with duplicated characteristics data.
Study Selection
Two authors (S.B. and M.H.S.) independently assessed all retrieved studies by title and abstract. Articles that initially met the inclusion and exclusion criteria were then further evaluated by a full-text review. If there was disagreement with regard to the initial review, studies were reviewed by the senior author (S.W.C.) to make an ultimate decision.
Data Collection Process
Two authors (S.B. and M.H.S.) independently extracted all relevant data from eligible studies. Discrepancies were resolved by consensus or by a third author (S.W.C.) if consensus could not be reached. Extracted information was as follows: general study information (author, year of publication, study design, and level of evidence 42 ), patient characteristics (sample size, mean age, sex, hand dominance, and mean follow-up duration), preoperative functional scores (pain visual analog scale [VAS], American Shoulder and Elbow Surgeons [ASES] score, Constant score, and active range of motion [ROM]) and radiologic fatty infiltration data of each rotator cuff muscle, surgical intervention information (surgical position, surgical procedures performed [open or arthroscopic], graft type), imaging method (ultrasound [US] or magnetic resonance imaging [MRI]), and outcomes (graft retear rate, complication rate, pain VAS, ASES score, Constant score, active ROM, and abduction strength). Partial tear of the graft (also described as a partially intact graft or partial healing of the graft) was not regarded as a graft retear; only a complete graft retear or failure was defined as a graft retear in this review.
Data Analysis
A systematic review and qualitative analysis were performed for all eligible studies. Patient characteristics and clinical outcomes were documented in the form of means and standard deviations. The outcomes of interest for this study were graft retear rate, complication rate, pain VAS, ASES, Constant score, active ROM, and abduction strength; and among these, the meta-analysis between IG and SCR was performed for the ASES score, graft retear rate, and complication rate, as those were common denominators reported by most of the studies. Furthermore, outcomes according to graft type (autograft vs allograft) were compared.
Quality Assessment
All studies that met inclusion criteria were assessed for methodologic quality by 2 independent reviewers (S.B. and M.H.S.) using the methodological index for non-randomized studies (MINORS). 48 The 12-item MINORS questionnaire is scored as 0 (not reported), 1 (reported but inadequate), and 2 (adequate), with a maximum score of 16 for noncomparative studies and 24 for comparative studies. Noncomparative studies with a MINORS score of ≥13 and comparative studies ≥21 are considered to have a low risk of bias. The methodologic quality was stratified according to the MINORS score for noncomparative studies and was reported as very low (0-5), low (6-10), fair (11-15), and good (16). For any calculated score, discrepancies between reviewers were resolved by consensus.
Statistical Analysis
All statistical analyses were performed using Comprehensive Meta-Analysis Version 3 (Biostat). The study characteristics at baseline and the clinical outcomes at preoperative status and final follow-up were summarized in the form of means and standard deviations using the Hozo et al 24 formula calculated from the median, range, and size of sample. The overall prevalence was computed for both groups by the use of the Wilson procedure with correction for continuity. 57 Frequency-weighted mean outcomes were used to assess the differences between groups. The Mann-Whitney U test was used for continuous variables, and the Fisher exact test and chi-square test were used for categorical variables.
A meta-analysis was conducted within each group to produce combined estimates of measures of effect with 95% CIs. The meta-analysis was performed using random-effects models weighted by sample size, because the overall heterogeneity was moderate to high. 45 Heterogeneity between studies was quantified using I 22 values. Ranges across outcome measures, derived from the included studies, were displayed on forest plots. The forest plots indicate the mean differences and 95% CIs from preoperatively to the last follow-up. A P value <.05 was deemed statistically significant.
Results
Study Selection
The initial literature search identified a total of 1608 articles. In addition to this, 30 articles were added through citation review. Among the 1638 articles screened, 334 duplications were removed and another 1200 were excluded by title alone. After screening the 104 abstracts for eligibility, we retrieved 21 articles for full-text review. Among these, 4 articles that had repeated data (2 by Mihata, 32,33 1 by Burkhart, 8 and 1 by Snyder 7 ) were excluded. Ultimately, 17 studies § (720 shoulders in 678 patients) from 2006 to 2020 met our inclusion and exclusion criteria and were selected for the current systematic review, as shown in Figure 1.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) study selection flowchart.
Study Characteristics and Demographics
The study characteristics and demographics are reported in Table 1. There were 10 IG studies (357 shoulders in 321 patients) and 7 SCR studies (363 shoulders in 357 patients); 5 were cohort studies and 12 were case series. Regarding surgical techniques, in the IG group, 3 studies performed open surgery, 4 studies performed arthroscopic surgery, 2 studies performed arthroscopy + miniopen surgery, and 1 study performed open or arthroscopic surgery; all procedures in the SCR group were arthroscopic surgery. In the IG group, autografts were used in 43 cases, allografts in 117 cases, xenografts in 98 cases, and synthetic grafts in 99 cases. However, in the SCR group, only autografts or allografts were used; thus, the subgroup comparison according to the graft type was performed only for autografts versus allografts. The study by Lee and Min 28 was excluded, as we could not separate the autograft and allograft data; thus for the SCR group, the subgroup analysis included 131 autograft cases and 196 allograft cases.
Summary of the Characteristics and Demographics of the Included Studies a

a ECM, extracellular tissue matrix; F, female; FL, fascia lata; LOE, level of evidence; M, male; NR, not reported; PTFE, polytetrafluoroethylene.
b We attempted to use autografts in all patients; however, in sarcopenic patients, patients with a history of surgery at the thigh level, or patients who did not want an autograft, allografts were used.
The mean age at the time of surgery was 61.96 ± 5.19 years for the IG group and 63.10 ± 2.93 years for the SCR group (P = .044); 51.3% of patients in the IG group and 63.9% in the SCR group were men (P = .002). In addition, patients in the IG group had a longer follow-up period than in the SCR group (35.92 ± 9.55 vs 19.25 ± 7.71 months, respectively; P < .001). Fatty infiltration grade, as defined by Goutallier et al, 19 was documented in 6 of the 17 studies 22,13,29,37,38,43 (3 using IG 37,38,43 and 3 using SCR 22,13,29 ); the grades for the infraspinatus and subscapularis were lower in the IG group compared with the SCR group (Appendix Table A1).
Risk-of-Bias Assessment
There were 5 studies with evidence level 3 and 12 studies with evidence level 4. Nine of 14 noncomparative studies had a low risk of bias. However, none of the comparative studies had a low risk of bias. The results of the assessment of methodologic quality using MINORS scores are summarized in Appendix Table A2.
Clinical Outcomes
Functional Outcome Scores
Functional outcome scores were reported in all 17 studies, but 2 studies 40,47 only reported postoperative scores. The most commonly documented outcome scores were pain VAS, ASES, and Constant scores. Pain VAS scores were reported in 10 of the 17 studies (58.82%), ASES scores in 14 of the 17 studies (82.35%), and Constant scores in 8 of the 17 (47.05%) studies. The University of California Los Angeles shoulder score, 37,58 12-Item Short Form Health Survey score, 20,21 and Oxford Shoulder Score 43 were reported in the IG group, and the Japanese Orthopedic Association score 31 and Subjective Shoulder Value score 9,13 were reported in the SCR group. However, these scores existed only in 1 group (either IG or SCR group) and thus were excluded from the comparison.
Range of Motion
ROM was reported in 13 of the 17 studies (76.47%), and active forward flexion (FF), external rotation (ER), internal rotation (IR), and abduction were documented. Active IR was measured in various ways. One study 4 used the Constant score’s IR points, another 1 study 40 measured the IR with an arm at 90° abduction position, and the other studies 13,28,31,37,38,47 measured the IR by determining how far the patient’s thumb could reach along the spinal segments (segments from T1 to T12 as 1-12, segments from L1 to L5 as 13-17, and the sacrum as 18). This last definition of IR was used for the comparison between groups. Abduction was reported in 5 of the 17 studies (29.41%), but only 1 study 44 in the SCR group; thus, a mean comparison between groups was not possible.
Strength Testing
Nine of the 17 studies (52.94%) measured strength in various directions using methods such as the Constant score strength subscale (points), 4 digital dynamometer (lb, N), 37,40,44,47 Nottingham mecmesin myometer (kg), 5,29 or modified Medical Research Council scale (grade) 20,21 ; thus, a direct comparison of the strength results was restricted. In most of the studies (7 of 9 studies), 4,5,20,21,40,44,47 strength significantly improved postoperatively, but 1 study 37 in the IG group (using autograft) reported no difference in IR strength at final follow-up, and another 1 study 29 in the SCR group (using autograft) reported no substantial postoperative change in supraspinatus and external rotator muscle strength.
Graft Repair Integrity
All studies (720 shoulders; 357 in the IG group and 363 in the SCR group) reported complete graft retear rates among their cohorts at final follow-up, which ranged from 12 to 50.3 months. Graft repair integrity was evaluated by using MRI in 8 studies, 9,13,29,31,37,38,44,58 US in 6 studies, 4,20,21,40,43,47 and a combination of both in 3 studies. 22,5,28
Complications
Complications were reported in most of the studies (15 of the 17 studies), but 2 studies 28,44 did not document any complications. In the IG group, 4 patients with complications (3 superficial subcutaneous infections and 1 deep wound infection) were reported, and all were resolved after arthroscopic irrigation and debridement and antibiotic treatment. In the SCR group, 20 patients with complications (3 deep infection, 4 suture anchor pullout, 2 severe shoulder contracture, 1 discomfort in the gluteal muscle after fascia lata autograft surgery, 1 persistent biceps pain, and 9 nonspecified) occurred, and 8 cases (40%) required revision surgery (debridement and antibiotic spacer, arthroscopic capsular release, open subpectoral tenodesis, reverse total shoulder arthroplasty, or revision SCR). There were no cases of definitive graft rejection in either group.
For all studies, mean pre- and postoperative clinical scores, ROM, graft retear rate, and complication rate are described in Appendix Tables A3 and A4.
The IG group showed significantly lower pain VAS, higher ASES score, and better active FF, ER at side, and IR at final follow-up (all P < .001). On comparing the mean differences 30 between pre- and postoperative functional outcome scores and active ROM, we found the IG group showed significantly improved pain VAS score, Constant score, and active FF and IR (all P < .001). Although there was no difference in the final Constant score between groups, the mean difference was significantly higher in the IG group, indicating greater improvement in Constant scores postoperatively compared with the SCR group. With respect to differences in patient-reported outcome measures between groups, only the Constant score reached the minimal clinically important difference (MCID) of 15 points as reported in previous studies. 23,51,52 But mean improvement in the ASES score was significantly better in the SCR group. There was no significant difference in the amount of gains in ER between groups (Appendix Table A5).
For the graft retear rate, there were 38 cases of complete graft retear in the IG group (documented by site as follows: at the repaired infraspinatus [19 cases], graft-humerus interface [2 cases], graft-tendon interface [2 cases], both the graft-humerus and graft-tendon interface [2 cases], graft midsubstance [1 case], and not specified [12 cases]); and there were 46 cases of complete graft retear in the SCR group (documented by site as follows: at the lateral humeral attachment site [31 cases], graft midsubstance [4 cases], medial glenoid site [4 cases], and not specified [7 cases]). The total graft retear rate was slightly lower in the IG group, although it did not reach statistical significance (IG = 10.6% vs SCR = 12.7%; P = .397); however, in the subgroup analysis of the autograft results, the IG group showed a significantly higher graft retear rate compared with the SCR group (IG = 51.2% vs SCR = 10.7%; P < .001). The total complication rate was significantly lower in the IG group compared with the SCR group (IG = 1.1% vs SCR = 8.4%; P < .001), and in the subgroup analysis of the autograft and allograft results, the IG group also showed significantly lower complication rates (autograft: IG = 0% vs SCR = 12.2%, P = .013; allograft: IG = 0.9% vs SCR = 3.7%, P = .197), although the allograft subgroup analysis did not reach statistical significance (Appendix Table A6).
With regard to graft type, the xenograft and synthetic graft were used only in the IG group, and the results of the xenograft were poor. However, the results of the synthetic graft used in the IG were overall satisfactory when evaluated with a frequency-weighted mean (Appendix Table A7).
Meta-Analysis
ASES Score
This meta-analysis was possible in 8 studies (43 shoulders in the IG group and 327 shoulders in the SCR group) in which the ASES results were presented as mean ± SD, and all these 8 studies used arthroscopic surgeries. 22,9,13,29,31,37,38,44 The mean differences from preoperative to last follow-up of the IG and SCR groups were 43.49 (95% CI, 24.29-62.70) and 36.68 (95% CI, 28.27-45.09), respectively. Although the IG group showed a higher mean ASES score than the SCR group, the meta-analysis did not show a statistical difference between groups (95% CI, 30.07-45.48; I 22 = 97.24 [IG], 97.40 [SCR]; P = .44) (Appendix Figure A1). A subgroup analysis by autograft or allograft was not possible because of the limited number of cases.
Graft Retear Rate
All studies reported the graft retear rate (357 shoulders in the IG group and 363 shoulders in the SCR group). Although slightly lower in the IG group than the SCR group, there was no significant difference in the graft retear rate between groups in the meta-analysis (95% CI, 0.073-0.223; I 22 = 81.97 [IG], 81.44 [SCR]; P = .79) (Appendix Figure A2).
The graft retear of autografts was reported in 4 studies 29,31,37,38 (43 shoulders in the IG group and 131 shoulders in the SCR group), and that of allografts was reported in 7 studies 22,9,13,20,43,44,58 (117 shoulders in the IG group and 196 shoulders in the SCR group). There were no differences in the graft retear rate according to graft type in the meta-analysis (autograft: 95% CI, 0.045-0.601; I 22 = 93.28 [IG], 91.27 [SCR]; P = .22; allograft: 95% CI, 0.041-0.216; I 22 = 80.39 [IG], 69.12 [SCR]; P = .64) (Appendix Figures A3 and A4). The statistical difference of the frequency-weighted mean of the autografts shown in Appendix Table A6 disappeared in the meta-analysis because of the wide confidence interval.
Complication Rate
The complication rate was reported in all except 2 of the studies 28,44 (357 shoulders in the IG group and 239 shoulders in the SCR group). There was a statistically significant difference in the total complication rate in favor of the IG group (95% CI, 0.022-0.065; I 22 = 0 [IG], 52.83 [SCR]; P < .001) (Figure 2).
The complication rate of autografts was reported in 4 studies 29,31,37,38 (43 shoulders in the IG group and 131 shoulders in the SCR group), and that of allografts was reported in 6 studies 22,9,13,20,43,58 (117 shoulders in the IG group and 108 shoulders in the SCR group). There were no differences in the complication rate according to graft type in the meta-analysis (autograft: 95% CI, 0.009-0.150; I 22 = 0 [IG], 65.89 [SCR]; P = .25; allograft: 95% CI, 0.012-0.081; I 22 = 0 [IG], 30.62 [SCR]; P = .09) (Appendix Figures A5 and A6).
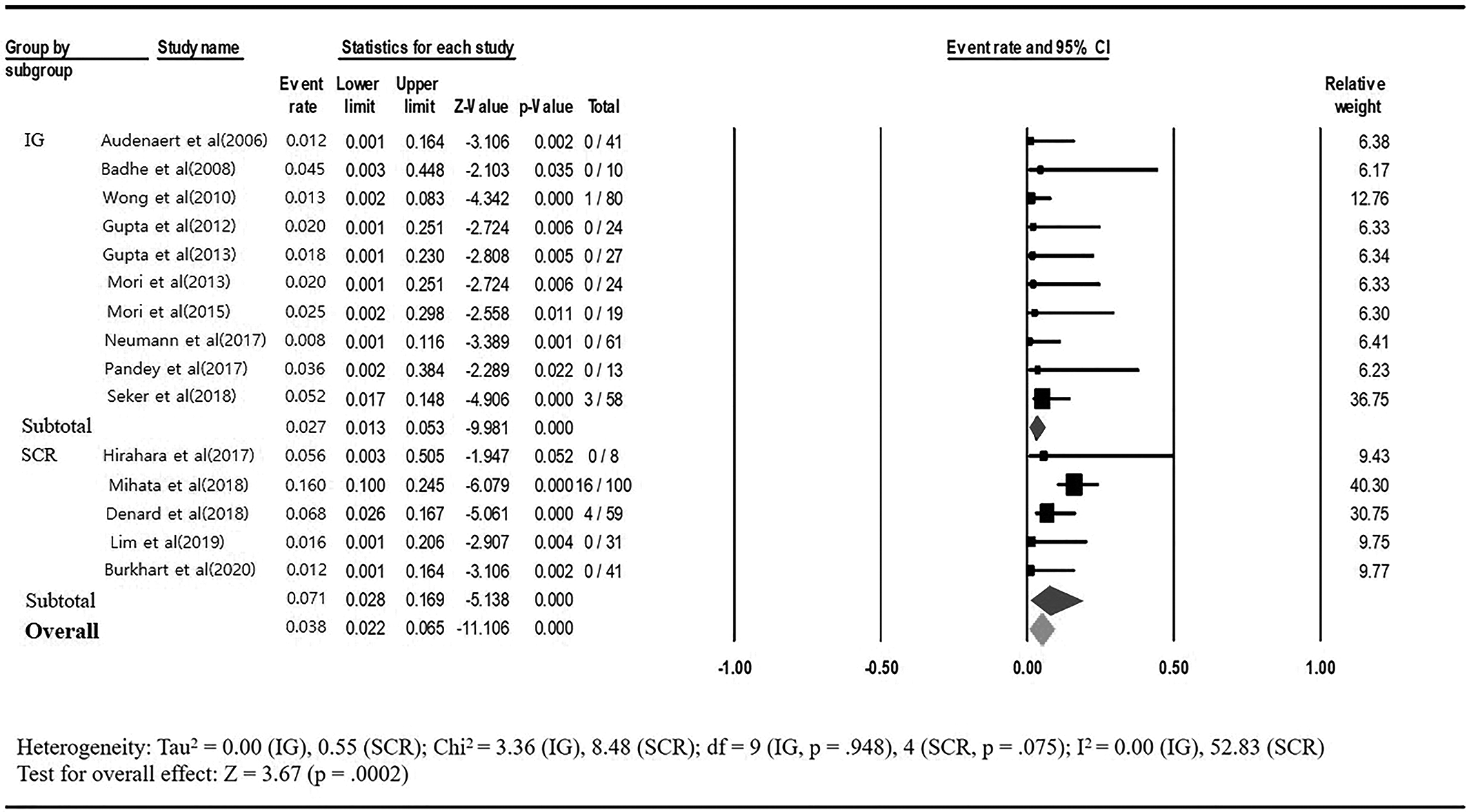
Forest plot comparing the total complication rate between interposition grafting (IG) and superior capsular reconstruction (SCR) groups.
Discussion
In this systematic review, we found that both the IG and SCR groups showed improved outcomes. The IG group displayed a tendency toward better results in overall clinical outcomes compared with the SCR group, although several outcomes did not reach to the significant level. Specifically, in the frequency-weighted mean analysis, the IG group showed better results in pain VAS, Constant score, active FF and IR, and complication rate, and in the meta-analysis, the complication rate was lower in the IG group compared with the SCR group. The graft retear rate was slightly lower in the IG group but did not show statistical significance, and results were not affected by graft type in this meta-analysis.
Two recent systematic reviews 30,55 have evaluated IG and SCR for massive irreparable RCTs. Wall et al 55 reviewed 16 articles published from 2014 to 2017 and documented the surgical techniques and the results of several biomechanical and animal studies. They concluded that, as no known literature comparing the 2 procedures existed, it was difficult to definitively assess the outcomes of IG and SCR. 55 More recently, Lin et al 30 reviewed 23 articles published from 2006 to 2019 and concluded that the IG group showed significantly better clinical and functional outcomes postoperatively than the SCR group. We tried to compare the effectiveness of IG and SCR more thoroughly, including more recent studies and using meta-analysis.
In this study, the mean differences in ASES scores of all included studies were 34.42 ± 11.81 and 38.17 ± 11.99 for the IG and the SCR groups, respectively, and they were 43.49 (95% CI, 24.29-62.70) and 36.68 (95% CI, 28.27-45.09) for the IG and the SCR groups, respectively, of the studies included in the meta-analysis. We believe the results of the meta-analysis are more reliable, as it was a more homogeneous comparison of the arthroscopic surgery. We should be cautious when interpreting the results, as there was no significant difference between groups in the meta-analysis, and the differences did not reach the MCID for the ASES (12 points, as reported previously 51 ). However, when compared with a systematic review, which evaluated the change in postoperative ASES scores in patients undergoing arthroscopic repair of massive RCTs (mean difference, 32.5), 49 the improvement in ASES score was comparable or even better in both groups, especially in the IG group.
The overall graft retear rate was not statistically significant between groups. In this study, we included the retear on the repaired infraspinatus as one of the graft retears, because it could affect the healing and function of the IG, and it was the most common retear site in the IG group (19 of 38 retear cases). If we had excluded this repaired infraspinatus from the graft retear cases, the difference may have been significant. However, we should be cautious that various factors, including the diagnostic modality (US or MRI), patient age, sex, and fatty infiltration of the rotator cuff muscles, may affect the results. Specifically, the fatty infiltration of the infraspinatus has been reported as a single independent prognostic factor in the massive RCTs. 10 It is important to consider that the SCR group had significantly worse preoperative status, with the exception of the Constant score (Appendix Table A5), and a significantly higher fatty infiltration grade (Appendix Table A1).
The subgroup analysis of the autografts showed a higher graft retear rate in the IG group. This result may be because there were only 2 studies 37,38 in the autograft subgroup of the IG group, and 1 of those studies 38 included only grade 3 or 4 fatty infiltration of the infraspinatus and showed an 89.4% graft retear rate. Unlike the graft retear site in the IG group, the most common graft retear site in the SCR group was the lateral humeral attachment site (31 of 46 retear cases). As Lim et al 29 reported, greater stress and abrasion seem to be concentrated on the distal portion of the SCR graft rather than the medial glenoid site during active shoulder abduction and elevation via acromiohumeral impact, which causes the retears on the lateral humeral side.
The IG group showed significantly lower complication rate (1.12%) compared with the SCR group (8.37%) in the meta-analysis. Moreover, the severe complication of deep wound infection occurred only in 1 case in the IG group, compared with the 3 cases in the SCR group. The 1 deep wound infection in the IG group was related to the patient's immunocompromised condition, 58 and it resolved after arthroscopic irrigation and debridement. Among the 3 deep infections in the SCR group, 2 were resolved by arthroscopic irrigation and debridement without removing the reconstructed superior capsule, 31 but 1 required additional placement of an antibiotic spacer. 13 In addition, there were no anchor-related complications in the IG group, compared with the 4 anchor pullouts in the SCR group. The reduced tension in the IG group may be the reason for the low number of anchor-related complications. Considering the previously reported complication rate associated with arthroscopic shoulder surgery (5.8%-9.5%), 56 the complication rate of IG seems to be very satisfactory. There are concerns regarding the possibilities of immunologic reaction of the allograft due to DNA from an allogenic source. 14,59 However, there were no graft rejection cases in either group. Rather, there was a donor site–related complication in the autograft case. Thus, we conclude that allograft is a good option for both IG and SCR as an easy-to-use, strong, and safe scaffold. Regarding graft type, it is hard to recommend which graft is better than the others because we could not compare xenograft and synthetic since these were not used in the SCR group.
The goals of surgery in patients with irreparable RCTs are to reduce pain, restore shoulder function, minimize complications, and delay the development of advanced cuff tear arthropathy. SCR was developed to improve glenohumeral kinematics by preventing humeral head superior migration and recentering the glenohumeral articulation, and it has been shown to improve function. 33 However, SCR is basically a salvage surgery, which gives up the active muscle function of the posterosuperior rotator cuffs. On the other hand, IG preserves rotator cuff muscle function and restores balanced shoulder mechanics by reconnecting the viable cuff tendon with less tension to the footprint through a graft. 38 This restoration of the active rotator cuff muscle function and the recovery of muscle strength in IG may bring better clinical outcomes, as shown in this systematic review. Previously, Elhassan et al 15 showed that lower trapezius transfer with an Achilles tendon allograft to restore active rotator cuff muscle function led to increased ER muscle strength and better clinical outcomes in massive RCTs. More specifically, Mori et al 37 suggested that IG could improve the healing of the infraspinatus tendon, resulting in the recovery of rotator cuff muscle strength and improved clinical outcomes. These studies support the importance of recovery of active rotator cuff muscle function with the IG procedure. Thus, IG that restores anatomy should be considered first as a joint-preserving surgery, and SCR could be considered as a next option as a salvage procedure for the cases where there is no cuff remnant to bridge. This is an area needed for future study.
There are several limitations in the present study. First, the sample size was relatively small in this systematic review, as we applied strict inclusion and exclusion criteria and as SCR is a recently developed surgical procedure. Second, there may have been some overlap of patients who participated in studies conducted at the same research center, 9,13,21,40 even though we tried to remove duplicate data. More high-quality studies with larger sample sizes are needed to show statistical significance in the meta-analysis and confirm the results. Fourth, the data of the included studies were heterogeneous. Although we presented a comprehensive review of the literature on IG and SCR following PRISMA guidelines and performed the meta-analysis using a random-effects model, which has a conservative nature on forest plots, the heterogeneity of the data made comparisons difficult and potentially problematic. The baseline characteristics for sex, fatty infiltration of each rotator cuff muscle, surgical method and position, and follow-up period were not the same between the IG and SCR groups, which may have acted as a bias. In fact, it is likely that the surgeon’s consideration for each procedure was different: SCR may be more useful in cases with a high Goutallier grade, and IG may be more useful if the quality of the rotator cuff muscles is still preserved. This variability in the included patients should be considered when interpreting the results. Notwithstanding these limitations, we believe that this systematic review and meta-analysis provides valuable information for orthopaedic surgeons planning the use of IG or SCR for irreparable RCTs.
Conclusion
Both IG and SCR techniques resulted in improvement in patients with irreparable RCTs. Meta-analysis showed a lower complication rate in the IG group; however, the lack of randomized studies limited our conclusions.
Footnotes
Notes
Acknowledgment
The authors thank So Jung Shin for support with data analysis.
Final revision submitted February 1, 2021; accepted February 24, 2021.
One or more of the authors declared the following potential conflict of interest or source of funding: This study was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science and ICT (NRF-2020R1A2B5B01001936). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
APPENDIX
Frequency-Weighted Mean Difference (Pre- vs Postoperative) in Clinical Outcomes According to Graft Type a

| SCR | IG | ||||||
|---|---|---|---|---|---|---|---|
| Autograft 29,31 | Allograft 9,13,22,44 | Autograft + Allograft 28 | Autograft 37,38 | Allograft 20,43,58 | Xenograft 5,21,40 | Synthetic 4,47 | |
| Pain VAS | 3.50 | 3.29 | 4.73 | 6.70 | 4.50 | 3.52 | NR |
| Constant | 12.00 | NR | 26.40 | 34.64 | 42.70 | 20.70 | 46.40 |
| ASES | 47.31 | 32.94 | 33.66 | 44.63 | 22.10 | 29.10 | NR |
| Active FF | 45.82 | 32.93 | 43.63 | 48.96 | 45.60 | 22.40 | 52.27 |
| Active ER | 11.92 | 14.33 | 15.32 | 11.60 | 18.90 | 12.19 | 12.98 |
| Active IR b | 3.00 | 2.00 | 5.26 | 3.63 | NR | NR | 6.00 |
| Active ABD | NR | 56.00 | NR | NR | 46.70 | 31.40 | 53.99 |
| SST strength | NR | 22.24 | NR | 45.00 | NR | NR | 13.00 |
| Graft retear | 5.94 | 5.36 | 5.91 | 10.30 | 0.44 | 2.34 | 3.34 |
| Complications | 12.21 | 2.18 | NR | 0 | 0.68 | 0 | 1.75 |
a ABD, abduction; ASES, American Shoulder and Elbow Surgeons score; ER, external rotation at the side; FF, forward flexion; IG, interposition grafting; IR, internal rotation; NR, not reported; SCR, superior capsular reconstruction; SST, supraspinatus; VAS, visual analog scale.
b Active IR was compared in the studies that assessed the IR by using the vertebral level (levels T1-T12 were designated as 1-12, levels L1-L5 were designated as 13-17, and the sacrum was designated as 18). 28