
Abstract
Background:
Compared with the single-row technique, the double-row rotator cuff repair technique is known to have a higher load to failure and a lower frequency of gap formation, leading to a lower retear rate. There are some patients with poor clinical outcomes or poor muscle strength without radiologic retear.
Purpose/Hypothesis:
To assess the postoperative position of suture knots via serial ultrasonography in patients who had undergone arthroscopic rotator cuff repair with the suture-bridge technique. Our hypothesis was that the suture would pull out of the lateral anchor (suture slippage), changing the positions of the medial suture knots during healing.
Study Design:
Case series; Level of evidence, 4.
Methods:
This study included 53 patients (55 shoulders) who underwent arthroscopic suture-bridge repair and were evaluated for a minimum of 24 months. On serial ultrasonography, a straight line was drawn between the top of the greater tuberosity and the medial cortex of the anchor hole. The distances between the knots of the medial rows and the perpendicular line through the center of the anchor hole were measured in longitudinal plane images of the supraspinatus. Follow-up ultrasonography was performed at 2, 3, and 6 months postoperatively as well as at the final visit. The visual analog scale, the American Shoulder and Elbow Surgeons score, the Constant score, and the University of California, Los Angeles shoulder score were recorded preoperatively and on the final follow-up.
Results:
Of the 55 shoulders, 6 developed retears at repaired sites. The mean follow-up duration was 37.5 months (range, 24-65 months). Slippage distance increased significantly over time (P < .001). The slippage at the final visit did not differ between patients with retear and no retear (13.4 mm for retear group; 10.6 mm for no retear group [P = .096]).
Conclusion:
Suture knots of the medial row migrated medially via a suture pullout from the lateral row anchor of suture-bridge technique. Suture slippage distance did not differ significantly between retear and no retear groups.
Arthroscopic rotator cuff repair is a common procedure for rotator cuff tears from partial thickness to large-sized, full-thickness tears. 7,40 Many reports support equal or better clinical results compared with open repair. 6,7,15,24,45 The techniques include the single- or double-row repair and the suture-bridge technique, depending on the size and shape of the tear. The double-row technique is known to have higher load to failure and lower frequency of gap formation compared with the single-row technique, thereby leading to lower retear rates. 3,14,15,20,32,33,41
The suture-bridge technique has advantages over the conventional double-row technique in that it affords additional compression imparted by the medial sutures. 35 –37 It is presumed to improve the pressurized contact area and create a greater mean pressure between the tendon and the footprint, thereby enhancing biological healing. 36 The suture-bridge technique and double-row technique are comparable in terms of patient satisfaction, functional outcomes, and retear rates. 23,46 However, despite these remarkable advances, the retear rate of the suture-bridge technique remains high, at 11% to 48.4%, 16,27 which is considered a major cause of postoperative pain. 14,20,32,43
Most rotator cuff retears occur within the first 6 months postoperatively. 31 Yet, there are some patients with poor clinical outcomes or poor muscle strength without radiologic retears. Thus, postoperative evaluation of tendon integrity is important in this group of patients. 31 Ultrasonography can be used as a modality to evaluate the integrity of repaired rotator cuff tendons. It is cost-effective, accessible, simple, and reliable because of the dynamic imaging. 29,39 One cause of these failed outcomes in rotator cuff repair surgery can be suture failure. For example, in the suture-bridge technique, the suture can pull out from the lateral anchor, causing a medial migration of the medial knots during the postoperative period, a term we introduce as “suture slippage.” Therefore, the purpose of this study was to assess the suture-knot positions in the postoperative period via serial ultrasonography in patients who had undergone arthroscopic rotator cuff repair with the suture-bridge technique. We hypothesized that the suture would pull out from the lateral anchor, thereby changing the positions of the medial suture knots in many of these patients who underwent arthroscopic rotator cuff repair with the suture-bridge technique.
Methods
Patient Enrollment
We retrospectively reviewed data from consecutive 87 patients with medium sized (1 to ∼3 cm by the Cofield classification) full-thickness supraspinatus tears. Small or partial-thickness tears that did not require the suture-bridge technique were excluded. All surgeries were performed at a single university hospital by 1 senior surgeon (H.S.S.). The exclusion criteria were as follows: (1) open repair (n = 1 patient); (2) ultrasonography follow-up <2 years (n = 6 patients); (3) conventional double-row repair (n = 1 patient); (4) patients with revision (n = 3 patients); (5) combined repair of subscapularis tendon (n = 18 patients); and (6) patients whose sutures were loose when arthroscopically probed (n = 5 patients). The study protocol was approved by an institutional review board, which waived the requirement for informed consent because of the retrospective nature of this study.
The method of Thomazeau et al 42 was used to evaluate supraspinatus muscle atrophy. Fatty degeneration in the supraspinatus was assessed as described by Goutallier et al 18 (grades 0 to 4).
Surgical Procedure and Postoperative Protocol
All surgical procedures were performed with the patient in the beach-chair position, sitting at an angle of 70 degrees under general anesthesia. The glenohumeral joint was examined through the standard arthroscopic posterior portal. After examination of the articular lesions on the supraspinatus, the arthroscope was moved to the subacromial space. Acromioplasty was performed if a large and sharp bony spur was observed following bursectomy. Then, a shaver was used to remove the frayed, torn end to evaluate the extent of the tear. Tear size in the anteroposterior and mediolateral dimension was assessed using a laser-marked probe. If the excursion of the tendon end was poor, adequate tendon mobilization procedures, such as coracohumeral ligament release and superior capsular release, were performed. Using a shaver, the footprint of the greater tuberosity was lightly debrided, and decortication was performed (Figure 1). Repair was completed with the suture-bridge technique. For the medial row, 2 double-loaded suture anchors (Bio-Corkscrew FT; Arthrex) were used and placed just lateral to the margin of the exposed footprint. The medial sutures were tied with the Revo knot technique. With sutures under tension, 2 lateral row anchors (Bio-SwiveLock; Arthrex) were inserted to compress the repaired tendon across the footprint.
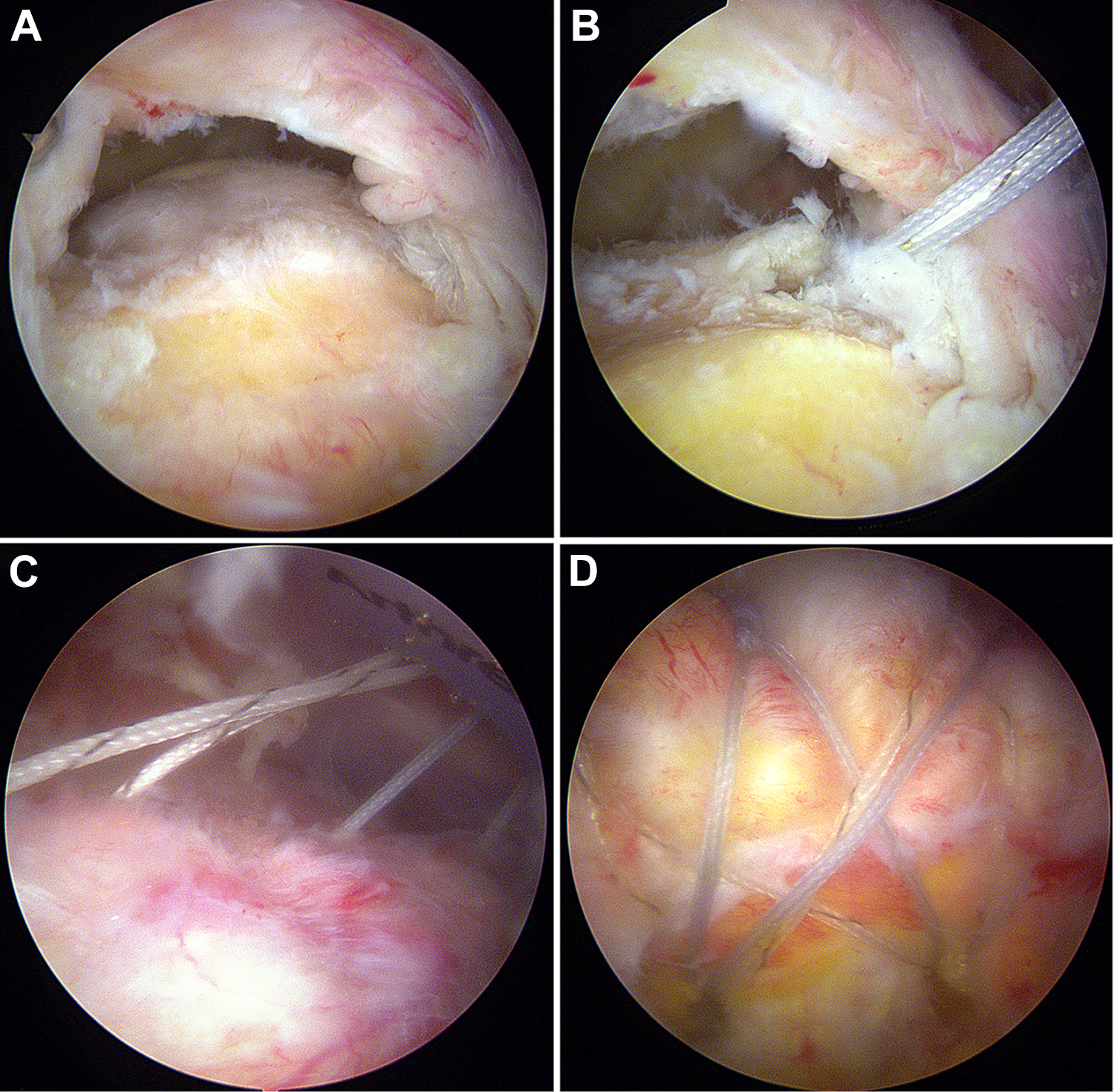
Arthroscopic photos of a 56-year-old man. (A) After decortication, (B) a medial anchor was inserted just lateral to the margin of the exposed footprint. (C) After passing the sutures through the cuff, (D) the procedure was completed with the suture-bridge technique.
All patients were immobilized for 6 weeks in a shoulder abduction brace. Intermittent wrist and hand exercises were encouraged immediately after surgery, and elbow motion was permitted on the second day postoperatively. Passive forward flexion was permitted 4 weeks postoperatively, and active assisted range of motion exercises were permitted 6 weeks postoperatively, with weaning off the abduction brace. Strengthening exercises commenced after 3 months postoperatively.
Ultrasonography Evaluation
All patients underwent ultrasonography, and real-time images were obtained with a linear 1- to 15-MHz transducer (Philips HD11 XE; Philips Medical Systems). All ultrasonographic examinations were performed by the same senior shoulder surgeon, having 10 years of experience with ultrasonography. The examinations were performed with the patient sitting on a chair and the examiner standing behind the patient (Figure 2). To examine the repaired supraspinatus tendon, the patient’s shoulder was extended, the elbow flexed, and the hand placed on the iliac wing (the modified Crass position), thus maximally exposing the supraspinatus tendon under the acromion.

Ultrasound examination. (A) The patient’s shoulder was extended, the elbow flexed, and the hand placed on the iliac wing (the modified Crass position), thus maximally exposing the supraspinatus tendon under the acromion. (B) While examining the supraspinatus tendon in the long axis view (coronal images), the suture knots (arrow) were hyperechoic with posterior acoustic shadowing. Disruption of the cortex showed an anchor hole. An imaginary anchor was drawn (dotted line).
Knot Distance Measurement Methods
While examining the supraspinatus tendon in the long axis view (coronal images), the suture knots were hyperechoic with posterior acoustic shadowing. If the knots were not clearly identified, they could be found by chasing sutures emanating from the lateral suture anchor on the dynamic images.
Reference points were created as follows: A straight line was drawn between the top of the greater tuberosity and the medial cortex of the anchor hole. Then, a perpendicular line was drawn, passing through the center of the anchor hole. The absolute distance was measured between the knot and this perpendicular line (a reference point) (Figure 3).

Longitudinal-plane ultrasound of repaired supraspinatus tendon of the right shoulder in a 62-year-old woman. A reference line was drawn between the medial cortex of the suture anchor (a) and the top of the greater tuberosity (b). A perpendicular line passing through the reference line (c) was drawn from the anchor hole. The distance (dashed arrow) from most medial suture knot (arrow) to line c was measured.
Serial follow-up ultrasonography was obtained at 2, 3, and 6 months postoperatively and at the final visit. All images were saved as videos. To reduce measurement bias, all saved, serial ultrasonography videos of each patient were measured during a single analysis session. All measurements were assessed by 2 orthopaedic surgeons and repeated at 1-month intervals. When assessing the videos, the information of the patients was blinded to the 2 surgeons (H.K. and S.B.H.). The intra- and interobserver reliability of the measurements were evaluated by calculating intraclass correlation coefficients (ICCs). The ICC values were interpreted as poor (<0.4), fair (0.4-0.59), good (0.6-0.74), and excellent (0.75 -1).
At 2-year follow-up, magnetic resonance imaging (MRI) was performed to evaluate the integrity of the repaired tendon retear and record any retears.
Functional Outcome Measures
To measure patient-reported outcomes, the visual analog scale for pain, and the American Shoulder and Elbow Surgeons, Constant, and University of California, Los Angeles shoulder scores were recorded preoperatively and at the final visit.
Statistical Analysis
The repeated-measures analysis of variance and post hoc test using the Bonferroni method were used to analyze measured distances over time. The paired t test was used to assess the slippage distance between time points. The Wilcoxon signed-rank sum test was used to assess the changes in functional outcome scores from preoperatively to the final visit. The Mann-Whitney U test was used to compare changes in the outcome scores between patients with postoperative retears and those without. The chi-square analysis with linear-by-linear association was used to compare the preoperative fatty degeneration and muscle atrophy evident on MRI between groups. SPSS Version 24.0 (IBM) was used for all statistical analyses. The significance level for all analyses was set at P < .05.
Results
This study included 53 patients with 55 affected shoulders who were treated with arthroscopic suture-bridge repair and had a minimum 24-month follow-up. The mean age of the patients was 62 years (range, 40-80 years), and the mean follow-up interval was 37.5 months (range, 24-65 months). Of the 53 patients, 36 were women (67.9%). In 74% of cases, the dominant shoulders were affected. Two patients underwent bilateral surgery, yielding 55 cases. Acromioplasty was performed in 35 patients (63.6%).
The ICCs for intra- and interobserver reliability of the measured slippage distances was 0.825 and 0.792, respectively, indicating excellent agreement.
At 2-year follow-up, 6 shoulders (10.9%) had developed retears (Figure 4). All retears occurred at the tendon-bone interface. According to the Kim et al 25 classification of the fluid signal on MRI, there were 2 grade 1 retears (linear fluid collection around the anchor), 2 grade 2 (local collection of fluid around any location of the anchor), and 2 grade 3 (fluid collection around the entire length of the anchor, with the cyst diameter less than twice the anchor diameter). Significant differences in the extent of preoperative fatty degeneration and atrophy were not evident between the patients with retears and those without (Table 1).
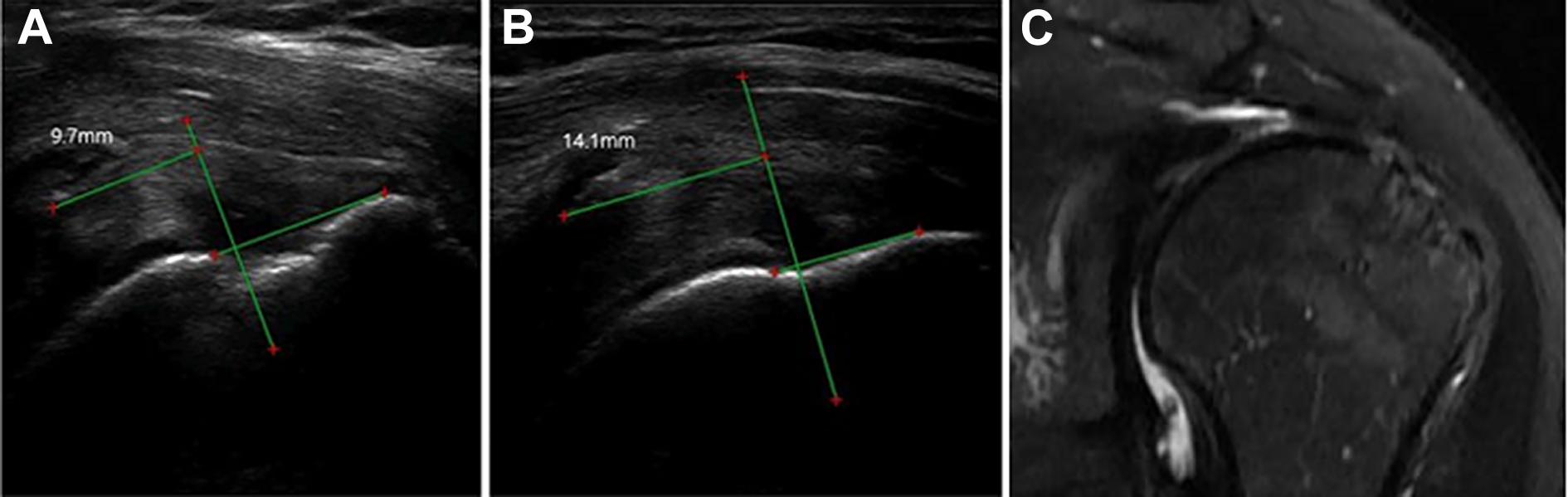
Serial postoperative follow-up right shoulder ultrasonography of a 53-year-old woman. (A) Extensive medial displacement of the knot (9.7 mm) was observed at 2 months postoperatively. (B) Displacement (14.1 mm) continued to the final visit. (C) A retear was confirmed on magnetic resonance imaging. For the green lines and red dots, see measuring methods in Figure 3.
Demographic Data for the Retear and No Retear Groups

a Mann-Whitney U test.
b Pearson chi-square test.
c Chi-square test for trend, linear-by-linear association.
Ultrasonography Evaluation
The mean postoperative suture slippage distance overall and by study group is shown in Table 2. When considering all patients, the mean distance was 6.8 mm at 2 months, 8.5 mm at 3 months, 10 mm at 6 months, and 11.1 mm at the final visit. The increase in slippage distance over time was statistically significant (P < .001). There were no significant differences in slippage distance between the retear and no retear groups at any specific time point; however, the overall P value of .079 suggested a trend toward significance (Figure 5).
Suture Slippage Distance at Postoperative Time Point a
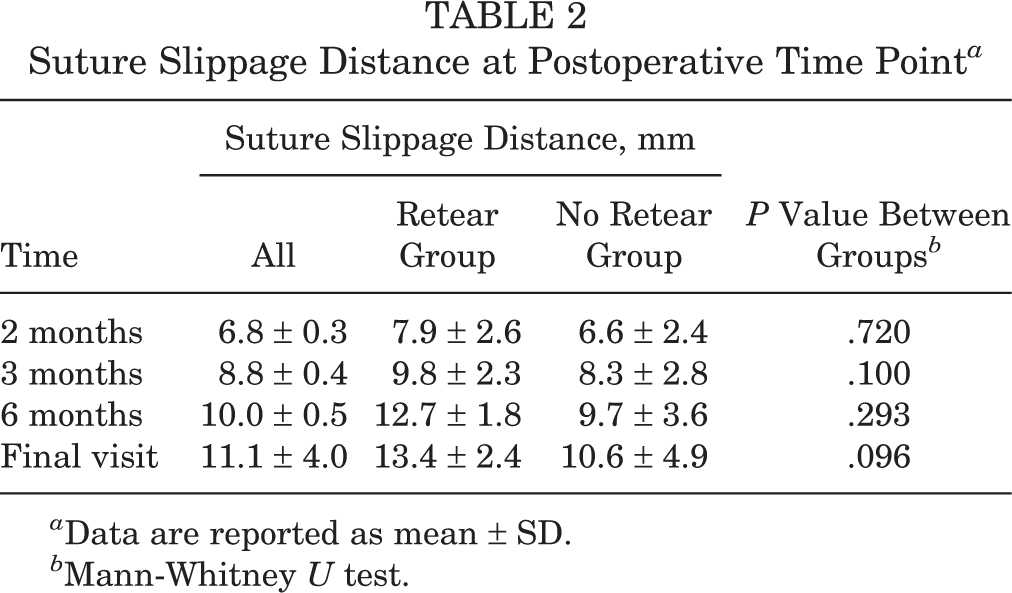
a Data are reported as mean ± SD.
b Mann-Whitney U test.

Suture slippage over time in the retear and no retear groups. Both groups exhibited a significant slippage over time (P < .001 for each), but only a trend toward significance (P = .079) was evident between the 2 groups.
The overall mean slippage distance between time points was 1.8 mm (2-3 months), 1.8 mm (3-6 months), and 0.5 mm (6 months--final visit) (Figure 6A). After 6 months, the slippage did not significantly increase. When the retear and no retear groups were compared, no significant differences in slippage distance were evident between the groups (Table 3).
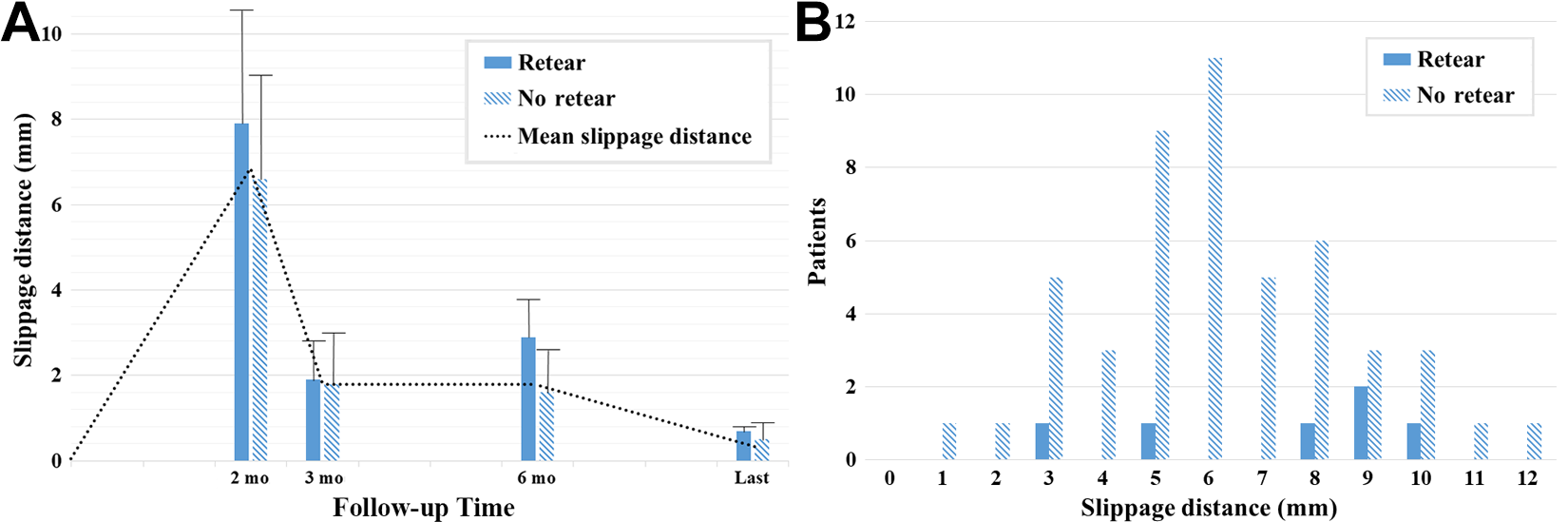
(A) Suture slippage distance in the retear and no retear groups over time and (B) according to number of patients at 2-month follow-up. No significant difference in slippage distance was evident between the 2 groups.
Mean Suture Slippage Distance Between Postoperative Time Points a

a Data are presented as mean ± SD.
b Mann-Whitney U test.
In an effort to define a proper cutoff predictive of retear at postoperative 2 months, a receiver operating characteristic curve analysis was performed. However, the area under the curve (AUC) rate was only 55%, which was not statistically significant (P = .720). At 6 months postoperatively, a slippage of 10.7 mm had a sensitivity of 83% and a specificity of 65% in terms of predicting retear; the AUC was acceptable at 75%.
Functional Outcome Measures
At the final follow-up, there was a clinically and statistically significant improvement in all functional outcome scores in all cases (P < .001 for all). In spite of there being only 6 patients with retears, all outcome scores were significantly better in the no retear group at the final follow-up (P ≤ .005 for all) (Table 4). The extent of suture slippage was not correlated with the outcome scores at the final follow-up (P > .05).
Outcome Scores for the Retear and No Retear Groups at Final Follow-up a
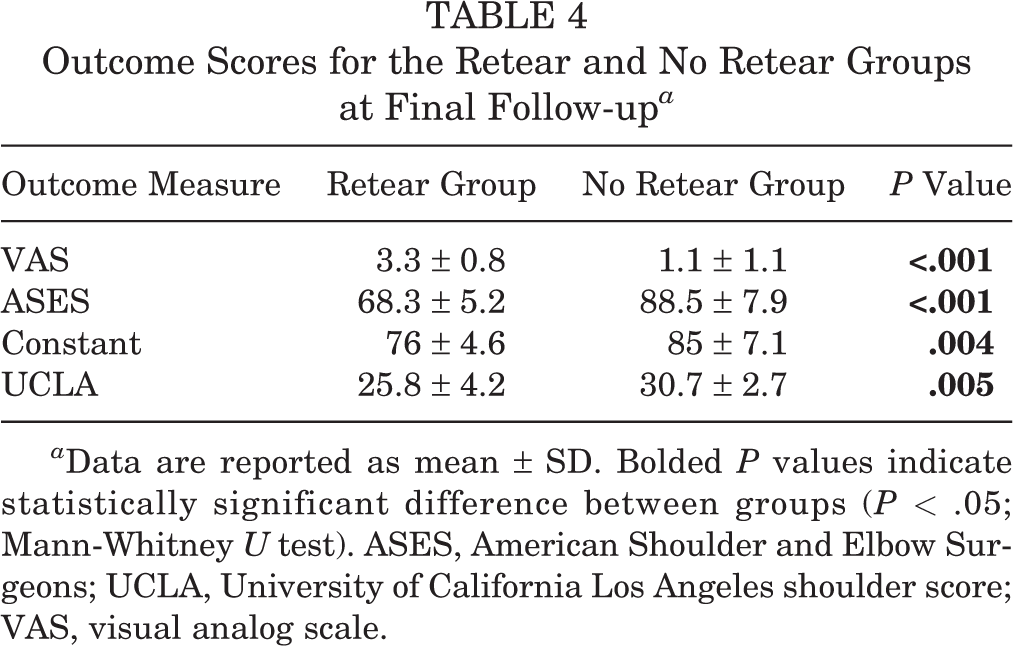
a Data are reported as mean ± SD. Bolded P values indicate statistically significant difference between groups (P < .05; Mann-Whitney U test). ASES, American Shoulder and Elbow Surgeons; UCLA, University of California Los Angeles shoulder score; VAS, visual analog scale.
Discussion
This study showed that after the suture-bridge technique, the suture knots displaced medially over time, suggesting suture slippage from the lateral anchor during healing. This was readily assessed using ultrasonography. It is not surprising that the suture knot moved on the repaired site. Contrary to surgeons’ expectations (firm fixation allows successful healing of the repaired tendon), the suture migrated and the repaired tendon lengthened during healing and rehabilitation. Multiple studies regarding repaired tendon lengthening measured via radiostereometric analysis have been reported. 4,22,30 It is an imaging technique allowing 3-dimensional measurements of distances between metallic markers to assess the integrity and mechanical properties of repaired tendons and ligament grafts in vivo. 4 In addition, computed tomography, combined with metallic marker placement, has been used to measure lengthening of repaired distal biceps. 30 All cases exhibited significant lengthening over time. In some of our cases, the cuff was healed on the follow-up MRI, despite suture slippage (Figure 7).
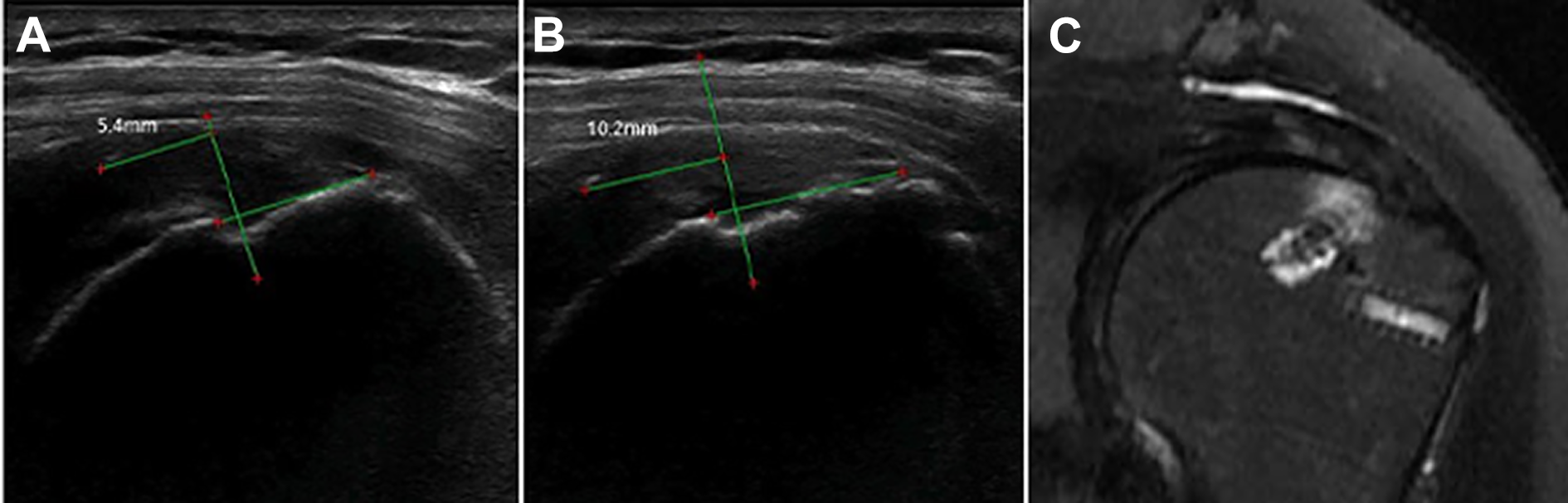
Serial postoperative follow-up right shoulder ultrasonography of a 70-year-old woman. (A) Medial displacement of the knot (5.4 mm) was observed at 2 months postoperatively. (B) Displacement (10.2 mm) continued to the final visit. However, (C) postoperative magnetic resonance imaging performed at 24 months exhibited no evidence of retear and showed good tendon integrity. For the green lines and red dots, see measuring methods in Figure 3.
Maximal lengthening occurred soon after operation. In another study, significant increases in the distances between tendon and bone markers were evident between 3 and 4 weeks and 12 and 14 weeks postoperatively. 2 These are the periods of most intensive physiotherapy. We found most slippages before 2 months (Figure 4).
The suture-bridge technique improves the ultimate load to failure and the pressurized footprint area and is thus a favored technique. 36,37 The results of many studies support both the biomechanical advantages and the surgical ease of the suture-bridge repair. 8 –10,37,46 We used knotless anchors for lateral row fixation. To secure the sutures, lateral row knotless anchors use an internal locking mechanism or exploit the pressure between the anchor body and nearby bone. The anchors are either threaded (screw-in) or not (push-in mechanism). All of our lateral row knotless anchors were the same threaded anchor (Bio-SwiveLock). This type of anchor evidenced good pull-out strength in previous biomechanical studies. 1,38 However, overtightening the suture bridge could reduce the intratendinous blood flow. 11
Many biomechanical studies have evaluated suture slippage of knotless suture anchors. 47 In a cadaveric study by Klinge et al, 26 they compared knotless anchors of the suture retention mechanism, which is press-fitting of the suture between the surrounding bone and the anchor, and the intrinsic suture-locking mechanism, in which the suture is secured within the anchor by the internal ratchet locking mechanism. Suture slippage differed from anchor-bone disengagement. Anchors with the suture retention mechanism exhibited more than 3 mm of suture slippage. A recent case report described subacromial and subdeltoid bursitis caused by suture slippage. 19 Sutures became disconnected from knotless lateral row anchors occurring bursitis. Most case reports of lateral row failure were attributable to anchor pullout. 21,44 Loosened medial knot would be possible because of the suture slippage.
There are several methods to evaluate repaired rotator cuff integrity postoperatively, including ultrasonography, MRI, magnetic resonance arthrography, multidetector computed tomographic arthrography, arthrosonography, and second-look arthroscopy. 5,12,13,39 Although MRI is known for its accuracy in the diagnosis of soft tissue lesions, such as rotator cuff tears, it showed inferior diagnostic accuracy (83%) in postoperative shoulders compared with preoperative shoulders. 28 Moreover, MRI is susceptible to suture-anchor artifacts, causing difficulty in postoperative assessment of rotator cuff integrity. Ultrasonography is used for analysis of postoperative rotator cuff integrity. Its sensitivity and specificity range from 80.8% to 91% and 86% to 100%, respectively, with accuracy of 89%. 17,34,39 Moreover, ultrasonography is cost-effective, noninvasive, readily accessible, and dynamic. Although MRI provides better information regarding repaired tendon integrity than ultrasonography, it is difficult to perform serial MRI scans at short intervals. In this study, video recording of ultrasonography images allows identification of the same knot over time and provides more accurate measurements than those that can be acquired from still images.
The primary goal of this study was to evaluate suture slippage by measuring suture knot distance. We found that suture knots became displaced medially over time. However, we could not prove that slippage was relevant to retear. The mean slippage distances tended to be larger at all times in the retear group, but these differences were not statistically significant.
In this study, all operations, ultrasonography, and outpatient interviews were performed by the same senior surgeon. To the best of our knowledge, no prior study has evaluated suture knot displacement by ultrasonography.
Limitations
This study had several limitations. First, it lacked data from the time zero of operation. Ultrasonography could not be performed right after the repair. Patients could not place the arm in an extended and internally rotated position at early postoperative periods because of pain and fear of retear. The first postoperative ultrasonography examination was performed at 2 months postoperatively. Thus, we simply assumed that the initial suture knot was placed just on the medial anchor. Second, it was difficult to serially measure the knot over time. There would be a measurement bias of the knots, although the ICC showed excellent reliability, 0.825 for intraobserver and 0.792 for interobserver reliability. Thus, we analyzed serial ultrasonography videos of each patient during a single analysis session rather than at the time of ultrasonography undertaken. By this method, we could have a chance to measure the knot serially and avoid measurement bias over time. Third, the relatively small sample size may have affected our results. We found only a trend, not a statistically significant correlation, between retear and suture slippage; there were only 6 retear cases (Figure 6B). Fourth, we used ultrasonography, which is an operator-dependent modality. However, all ultrasonography scans were performed by a single surgeon with 10 years of ultrasonography experience (approximately 100 cases per month). All measurements were assessed by 2 orthopaedic surgeons and repeated at 1 month interval. The ICC to evaluate the intraobserver and interobserver reliability was good (0.825 and 0.792, respectively). Last, cuff tension was not assessed after repair because cases were retrospectively analyzed.
Conclusion
Suture knots of the medial row migrated medially via suture pullout from the lateral row anchor of the suture-bridge technique. Most slippage occurred within 2 months postoperatively. Suture slippage distance did not differ significantly between patients with retear and those without.
Footnotes
Final revision submitted February 1, 2021; accepted February 25, 2021.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Eunpyeong Saint Mary’s Hospital (protocol No. PC19RESI0080).