
Abstract
Background:
Bioabsorbable interference screws and metallic interference screws are both widely used for graft fixation, but it remains unclear which screw type is superior.
Purpose:
To compare clinical outcomes and complications between bioabsorbable and metallic interference screws for anterior cruciate ligament reconstruction (ACLR).
Study Design:
Systematic review; Level of evidence, 1.
Methods:
The literature was searched for relevant randomized controlled trials published between 1966 and 2020. Two investigators independently assessed risk of bias in the included studies, and data were pooled to calculate mean differences (MDs) for continuous outcomes and risk ratios (RRs) for dichotomous outcomes, together with 95% CIs. Meta-analysis was performed using a random- or fixed-effects model, depending on the heterogeneity in the data.
Results:
Included were 14 randomized controlled trials involving 1032 patients who underwent ACLR: 528 patients with bioabsorbable screws and 504 patients with metallic screws. The 2 groups did not differ significantly in International Knee Documentation Committee score (RR, 1.04; 95% CI, 0.97 to 1.11), Lysholm score (MD, 0.59; 95% CI, –0.46 to 1.63), range of motion deficit (RR, 0.95; 95% CI, 0.67 to 1.34), positive pivot-shift test (RR, 0.87; 95% CI, 0.61 to 1.24), positive Lachman test (RR, 0.82; 95% CI, 0.48 to 1.39), or KT-1000 arthrometer value (MD, 0.01; 95% CI, –0.16 to 0.18). However, bioabsorbable screws were associated with a significantly higher risk of complications (RR, 1.70; 95% CI, 1.16 to 2.50), such as graft rupture, joint effusion, and infection.
Conclusion:
The results of this review showed that there was no difference between metallic and bioabsorbable screws for ACLR in terms of subjective knee function or knee laxity, but metallic interference screws had fewer complications.
Keywords
The anterior cruciate ligament (ACL), one of the strongest ligaments in the knee joint, connects the tibia to the femur and resists anterior translation and medial rotation of the tibia relative to the femur. 37 Injury of this ligament is common among orthopaedic patients who have suffered sports injuries or car accidents. During the acute phase of ACL injury, patients feel pain and the knee joint swells, preventing movement; during the chronic phase, the knee joint feels unstable. Approximately 100,000 ACL injuries occur in the United States each year. 33
ACL reconstruction (ACLR) is one of the most frequent arthroscopic surgeries. During ACLR, the grafts can be fixed by suspensory, cross-pin, or interference screw methods in order to achieve appropriate tension. 34 This study focused on the types of screws used in ACLR; currently, there are 2 types of screws from which to choose—bioabsorbable interference screws and metallic interference screws. 1,12
Metallic interference screws are still the gold standard to some extent, and they promote early integration into bone, with high initial fixation strength and load-to-failure outcomes. Metallic interference screws provide a positive clinical effect and a lower incidence of complications. The disadvantages of the metallic screws are that they interfere with magnetic resonance imaging (MRI) and may need to be removed in a revision surgery. 8,25
The introduction of bioabsorbable interference screws is a result of the development of biomaterials and some patients preferring that the screws disappear.
5
While most metallic interference screws are composed of titanium today, bioabsorbable interference crews can be composed of various biomaterials, including polyglycolic acid (PGA), poly-
Several randomized controlled trials (RCTs) 9,20,27 have compared outcomes for ACLR involving bioabsorbable or metallic screws, but they have provided unclear results about which screws may give superior outcomes. To compare clinical outcomes and complications between metallic and bioabsorbable interference screws for ACLR, we performed a meta-analysis of RCTs in the literature. The hypothesis was that bioabsorbable interference screws were no better than metallic interference screws, especially in terms of complications.
Methods
Study Selection
The PubMed, Embase, and Cochrane databases were searched for relevant studies published between 1966 and August 2020. Search terms included “anterior cruciate ligament reconstruction,” “ACLR,” “orthopaedic fixation devices,” “absorbable implants,” “bone screws,” “bioabsorbable screws,” “metallic screws,” and “randomized controlled trial.” The gray literature and databases of unpublished studies were also examined, as were potentially eligible studies manually identified from the reference lists of included studies.
Studies were included if they were RCTs that compared outcomes between ACLR patients who received bioabsorbable or metallic interference screws. All types of grafts (allografts, autografts, or artificial grafts) were included. Duplicate studies with different follow-up times of the same patients were excluded, as well as those published in a language other than English, cadaveric studies, and those with a follow-up period less than 12 months.
Two reviewers (B.X. and Yuling Y.)
Data Extraction
Two investigators (B.X. and Y.Z.) independently extracted the following data using a standardized form: title, first author, publication year, country where the study was conducted, study design, inclusion and exclusion criteria, follow-up duration, outcomes, and patient characteristics at baseline. If necessary, the corresponding author of the included studies was contacted in an effort to obtain original data. Disagreements about the extracted data were resolved by discussion or by another investigator (W.F.).
The following data on complications (the primary outcome) were extracted: superficial or deep infection, joint effusion, and graft rupture. Data were collected on the following secondary outcomes: the International Knee Documentation Committee (IKDC) score and the Lysholm score, range of motion (ROM) deficit, positive pivot-shift test, positive Lachman test, and KT-1000 arthrometer measurement.
Assessment of Study Quality
Two investigators (B.X. and Yuling Y.) independently assessed the risk of various types of bias in the included studies, based on the Cochrane Handbook for Systematic Reviews of Interventions. This assessment comprised 7 bias domains: random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias), or other bias. Risk in each domain was classified as high, low, or unclear; the assessment of “unclear” was supported with a reason. Disagreements in quality assessments were resolved by discussion.
Data Analysis
All data analyses were performed using Revman 5.3 (Nordic Cochrane Centre, The Cochrane Collaboration). Dichotomous outcomes were meta-analyzed to yield risk ratios (RRs) and 95% CIs, while continuous outcomes were meta-analyzed to yield mean differences (MDs) and 95% CIs. Meta-analysis involved a fixed-effects model if I 2 ≤ 50% and the associated P > .1, indicating low heterogeneity. Otherwise, a random-effects model was used. Publication bias for a given outcome was assessed using funnel plots, as long as data for that outcome could be pooled from more than 10 studies. Sensitivity analysis was performed to assess excessive influence of individual studies on the pooled results.
Results
Search Results and Study Characteristics
The search strategy yielded 241 studies, which were first screened based on titles and abstracts and subsequently based on reading of the full text. After excluding ineligible studies and duplicate publications, 14 studies were included in the final meta-analysis (Figure 1). Three studies 5-7 involved the same patient samples, so only the most recent was included in the meta-analysis.
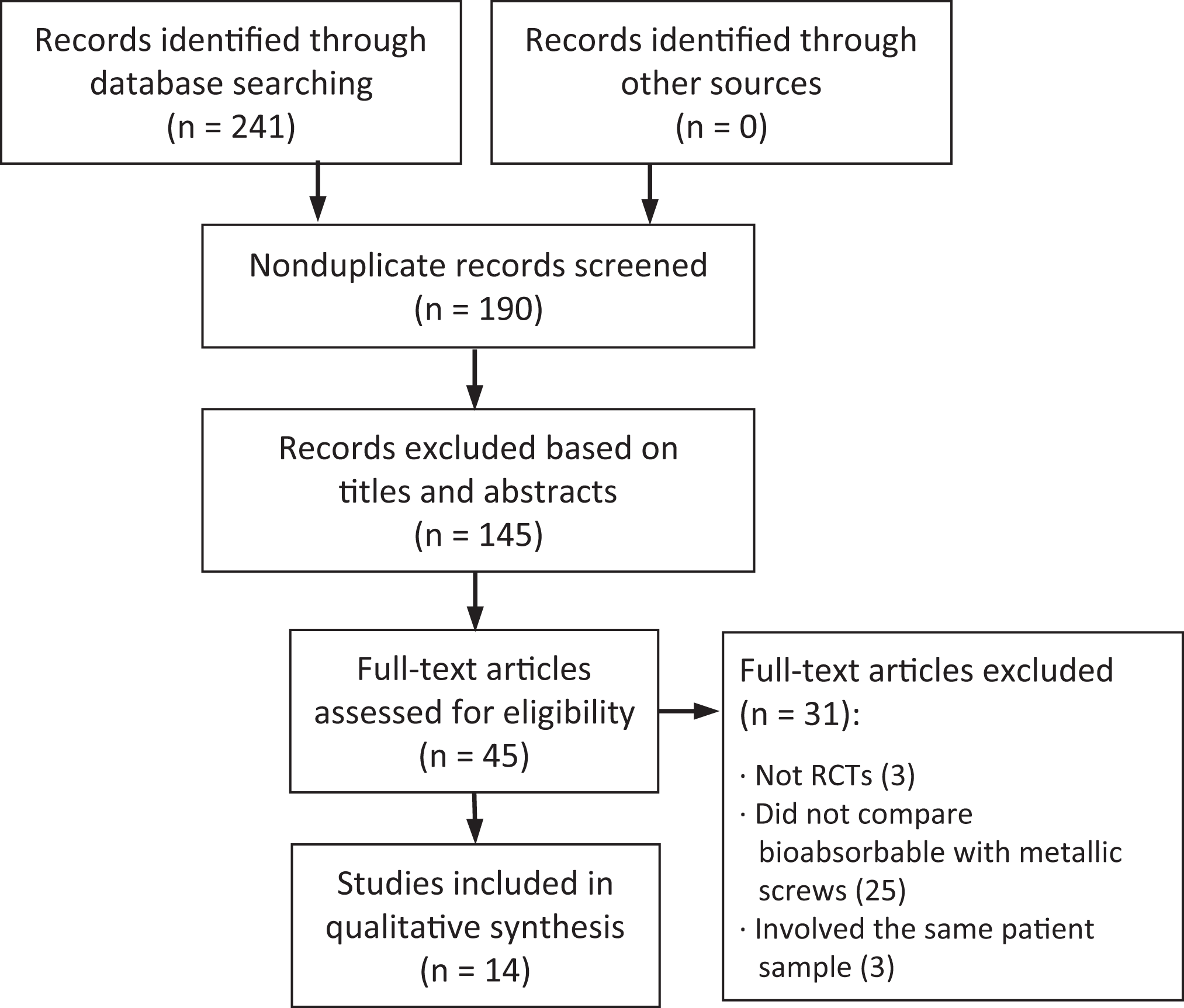
Flowchart of study screening and selection. RCT, randomized controlled trial.
The final set of 14 RCTs § involved 1032 ACLR patients with a mean age of 28.9 years, of whom 528 received bioabsorbable screws and 504 received metallic screws (Table 1). All studies reported level 1 or 2 evidence and were published between 1999 and 2020. Two studies were performed in the United States, 18,27 2 in Australia, 29,36 3 in Finland, 15,16,28 and 1 each in Austria, 9 Germany, 14 India, 13 Japan, 20 the Netherlands, 2 Norway, 7 and Sweden. 24 Seven studies involved hamstring autografts, 13,15,16,24,28,29,36 6 involved bone–patellar tendon–bone autografts, 2,7,9,14,18,20 and 1 study 27 involved autografts and allografts. Six studies involved bioabsorbable screws made of PLLA 7,14,18,20,24,27 ; 2 studies each involved screws of PLLA-HA, 29,36 PGA/TMC, 2,9 or PLLA/TMC/PDLA 16,28 ; and 1 study 15 involved screws of PLLA/TMC. One study 13 did not mention the composition of its bioabsorbable screws. Ten studies used metallic screws of titanium, while the remaining 4 studies 13,15,24,27 did not mention the type of metal. Follow-up times ranged from 11 to 156 months postoperatively.
Characteristics of the Included Studies a

a
Allo, allograft; auto, autograft; BPTB, bone–patellar tendon–bone; BS, bioabsorbable screw; HA, hydroxyapatite; MS, metallic screw; NA, not available; NR, not reported; PDLA, poly-
Quality Assessment and Risk of Bias
Nearly three-quarters of the studies (71%) showed high risk of performance bias, and more than half (64%) showed unclear risk of selection bias (Figure 2). Risk of other types of bias seemed low in all studies.

(A) Risk of bias of the included studies. (B) Visual summary of bias risk.
Complications
Twelve studies ∥ reported data on adverse complications, of which 5 studies 2,14,18,27,36 reported data on joint effusion, 6 studies 2,9,14,18,24,27 reported data on deep or superficial infection, and 9 studies 2,7,14 –16,24,27 –29 reported data on graft rupture. Across all 12 studies, data on complications did not show significant heterogeneity (I 2 = 0%; P = .72), and bioabsorbable screws were associated with a significantly higher risk of complications (RR, 1.70; 95% CI, 1.16-2.50) (Figure 3). There was no significant difference between patients receiving bioabsorbable or metallic screws among the subsets of studies reporting data on joint effusion (RR, 1.46; 95% CI, 0.87-2.46) or infection (RR, 1.05; 95% CI, 0.39-2.85). Bioabsorbable screws were associated with significantly higher risk of graft rupture (RR, 2.54; 95% CI, 1.27-5.08).

Forest plots of complications after anterior cruciate ligament reconstruction involving bioabsorbable or metallic screws. M-H, Mantel-Haenszel.
Lysholm Score
Five studies 7,9,15,16,36 reported Lysholm scores, and the data showed no significant heterogeneity (I 2 = 0%; P = .88) (Figure 4). Across all 5 studies, there was no significant difference between patients who received bioabsorbable or metallic screws (MD, 0.59; 95% CI, –0.46 to 1.63), and similar results were observed at follow-up periods of 1 year (MD, 0.37; 95% CI, –1.12 to 1.87), 2 years (MD, 0.58; 95% CI, –1.12 to 2.28), and more than 5 years (MD, 1.40; 95% CI, –1.48 to 4.28).
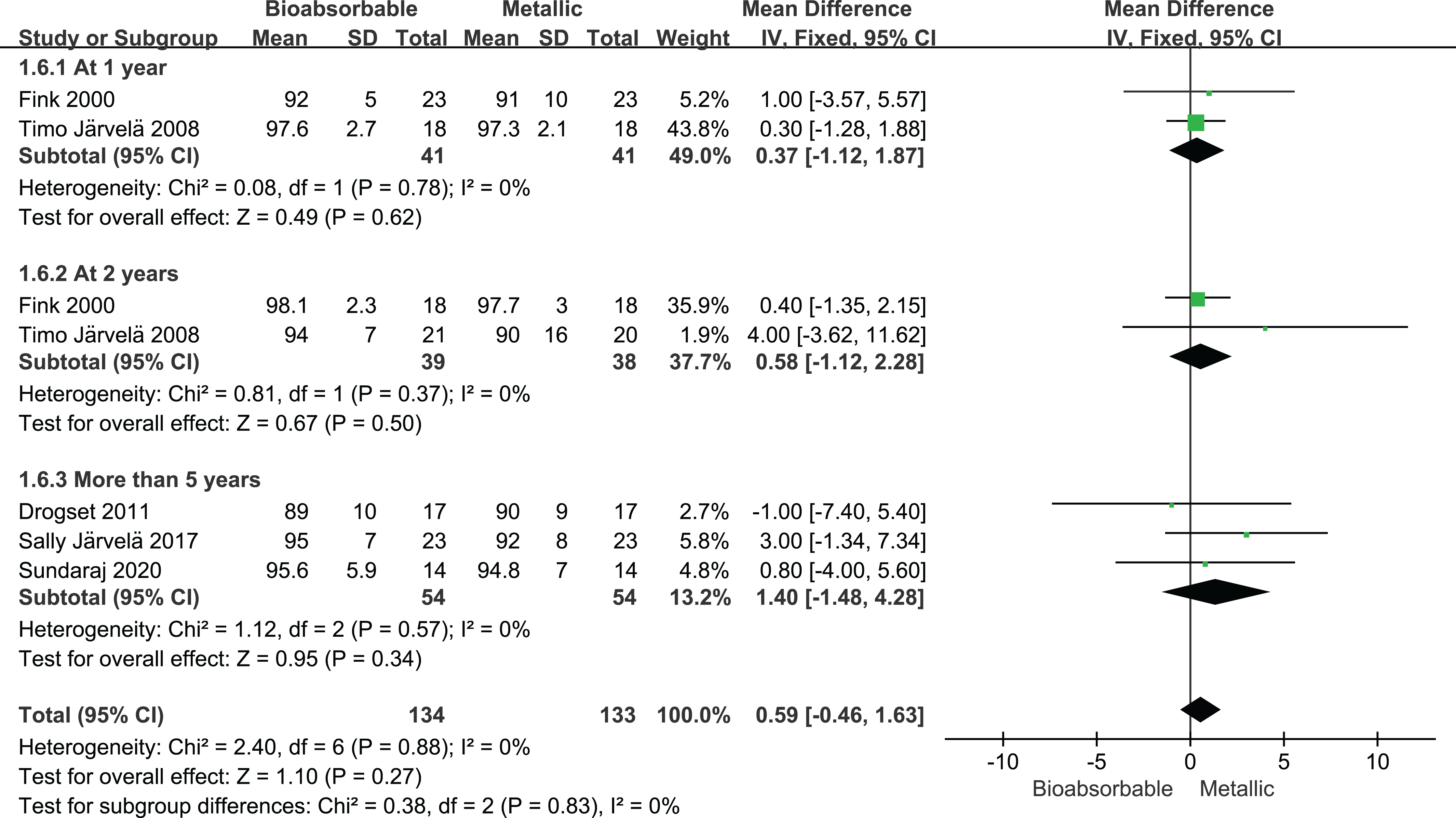
Forest plots comparing Lysholm score after anterior cruciate ligament reconstruction involving bioabsorbable or metallic screws. IV, inverse variance.
IKDC Score
Seven studies 2,9,15,16,24,28,36 reported the IKDC score of subjective knee joint function. There was no significant difference in risk of suffering self-reported inadequate function between those receiving bioabsorbable or metallic screws (RR, 1.04; 95% CI, 0.97-1.11; I 2 = 0%; P = .58) (Figure 5). Similar results were observed at follow-up times of 1 year (RR, 1.03; 95% CI, 0.94-1.12), 2 years (RR, 1.05; 95% CI, 0.93-1.19), and more than 5 years (RR, 1.03; 95% CI, 0.87-1.22).

Forest plot of International Knee Documentation Committee score after anterior cruciate ligament reconstruction involving bioabsorbable or metallic screws. M-H, Mantel-Haenszel.
ROM Deficit
Four studies 2,7,20,24 reported data on ROM deficit after ACLR, and there was no significant difference between patients who received bioabsorbable or metallic screws (RR, 0.95; 95% CI, 0.67-1.34; I 2 = 0%; P = .95) (Figure 6).

Forest plot of range of motion deficit after anterior cruciate ligament reconstruction involving bioabsorbable or metallic screws. M-H, Mantel-Haenszel.
Positive Pivot-Shift Test
Six studies 2,7,15,16,20,29 reported the rates of a positive result in the pivot-shift test, and these rates did not differ significantly between patients receiving bioabsorbable or metallic screws (RR, 0.87; 95% CI, 0.61-1.24; I 2 = 39%; P = .13) (Figure 7). The same results were observed for follow-up times of 1 year (RR, 0.98; 95% CI, 0.56-1.70), 2 years (RR, 0.98; 95% CI, 0.60-1.61), and more than 7 years (RR, 0.15; 95% CI, 0.02-1.10).
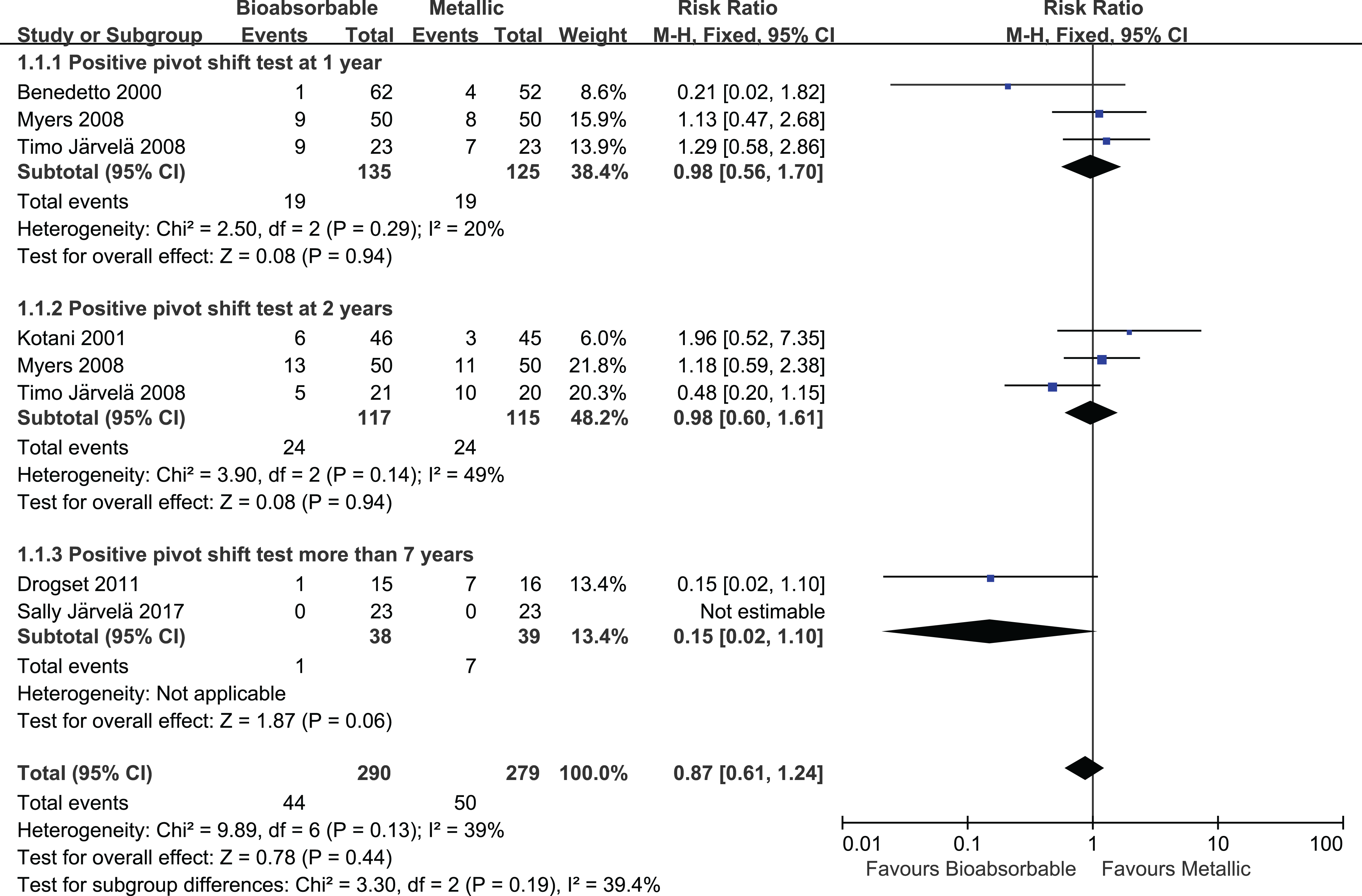
Forest plot of the rate of a positive result on the pivot-shift test after anterior cruciate ligament reconstruction involving bioabsorbable or metallic screws. M-H, Mantel-Haenszel.
Positive Lachman Test
Only 3 studies 7,14,20 reported rates of a positive result on the Lachman test. There was no significant difference between patients receiving bioabsorbable or metallic screws (RR, 0.82; 95% CI, 0.48-1.39) (Figure 8).
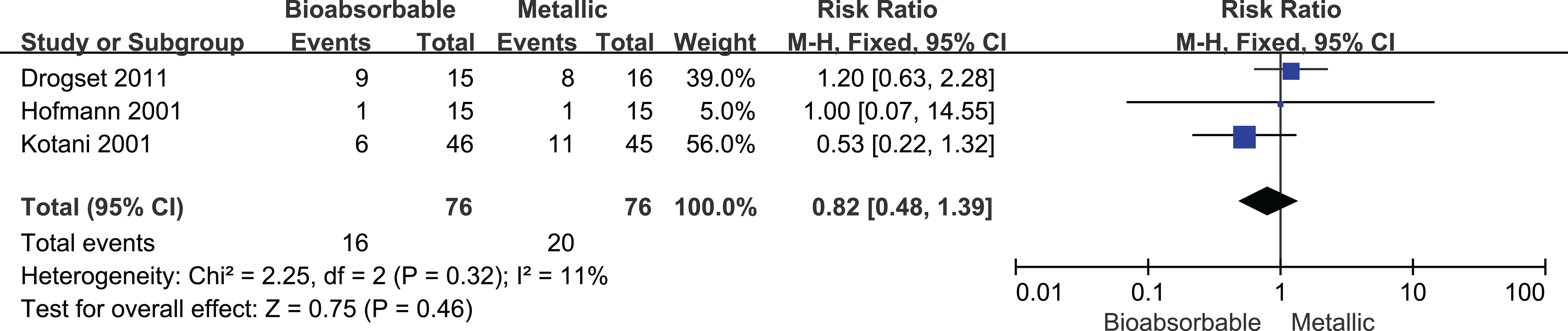
Forest plot of the rate of a positive result on the Lachman test after anterior cruciate ligament reconstruction involving bioabsorbable or metallic screws. M-H, Mantel-Haenszel.
KT-1000 Arthrometer Measurement
Eight studies 2,7,9,15,16,18,20,28 reported KT-1000 results, and there was no significant difference between patients receiving bioabsorbable or metallic screws (MD, 0.01; 95% CI, –0.16 to 0.18; I 2 = 0%; P = .91) (Figure 9). The same results were observed at follow-up times of 1 year (MD, 0.02; 95% CI, –0.16 to 0.21), 2 years (MD, –0.06; 95% CI, –0.50 to 0.38), and more than 5 years (MD, –0.10; 95% CI, –1.07 to 0.87).

Forest plot of KT-1000 arthrometer measurement after anterior cruciate ligament reconstruction involving bioabsorbable or metallic screws. IV, inverse variance.
Publication Bias
The funnel plot of studies reporting data on different complications was symmetric, indicating a low risk of publication bias (Figure 10).

Funnel plot of data on complications after anterior cruciate ligament reconstruction involving bioabsorbable or metallic screws. RR, risk ratio.
Discussion
In this meta-analysis of 14 RCTs, we found that Lysholm and IKDC scores of knee function after ACLR did not differ significantly between patients who received bioabsorbable or metallic screws, regardless of whether the follow-up was short term (1 year) or long term (more than 5 years). At the same time, we found that although the 2 types of screws were associated with similar rates of infection and effusion, metallic screws were associated with a significantly lower risk of graft rupture.
Our results suggest that bioabsorbable screws can provide sufficient strength for graft fixation and can exert biomechanical effects similar to those of metallic screws, as reported previously. 21 However, the pooled results seemed to be more supportive of metallic screws and indicated that bioabsorbable screws have a higher graft rupture rate than metallic screws. The finding of a high graft rupture rate in the bioabsorbable screw group was complicated by 2 included RCTs in which the study intentions were not to compare metallic and bioabsorbable screws. One study 15 aimed to evaluate the clinical outcomes of patients after ACLR performed with either the double-bundle or single-bundle technique, and the graft rupture was mainly the result of a minor accident. The other study 16 aimed to assess the clinical results of anatomical double-bundle ACLR using doubled semitendinosus and gracilis autografts, and the reason for graft rupture was the same: a minor accident. Our sensitivity analysis showed that after excluding the above 2 studies, there was no statistically significant difference between the 2 fixation groups in graft rupture (RR, 2.31; 95% CI, 0.92-5.81). However, the total effects also favored metal screws (RR, 1.54; 95% CI, 1.01-2.33); therefore, the rupture of the graft cannot be simply attributed to the fixation method, and our results should be interpreted with caution.
Three studies 24,28,29 involved tunnel widening, but the data were not pooled because of heterogeneity. Myers et al 29 reported that the tunnel was wider in the bioabsorbable group in the middle femur bone tunnel on anteroposterior (AP) (P = .05) and lateral (P = .003) films, but there was no difference in the results of the 2 types of screws in the tibia and distal femur. Moisala et al 28 found that the femoral tunnel in the bioabsorbable group was wider in the AP dimension of MRI (P = .01), but no difference was found in the mediolateral dimension and the tibial tunnel. Laxdal et al 24 found that at 2 years after ACLR, the bone tunnels in the bioabsorbable group were wider than those in the metallic group on the femoral side (P < .001) and tibial side (P < .001). Bioabsorbable screws may cause tunnel widening in the long term, 28,29 which implies greater osteolysis during ACLR when bioabsorbable screws are used. The tunnel widening may result when absorption of bioabsorbable screws leads to synovitis. 11,21,23 The risk of such widening may depend on the graft material: 1 study found that autografts of hamstring tendon, but not bone–patellar tendon–bone, led to tunnel widening at the 7-year follow-up, regardless of the initial graft tension. 4 Heterogeneity prevented us from reaching a unified conclusion, and we were limited by the sample size; therefore, we should understand the result of tunnel widening with caution.
Our analysis suggests that bioabsorbable screws and metallic screws may be associated with comparable outcomes in terms of the pivot-shift test, Lachman test, KT-1000 measurement, ROM, and scores on the IKDC and Lysholm scales. Nevertheless, metallic screws may be associated with lower rates of complications, which may need to be considered if a patient is particularly sensitive to the health effects of such complications.
Limitations to our analysis exist. Our results should be interpreted with caution because, although all the included studies were RCTs reporting level 1 or 2 evidence, the studies were at high risk of multiple types of bias. Not all studies reported data on all outcomes that we wished to analyze. Conference recordings were not retrieved, and we may have missed some trials. Another limitation was that postoperative radiographic data (e.g., tunnel widening) were insufficient to reach a clear conclusion.
Conclusion
The results of this meta-analysis indicated that there was no statistically significant difference between the bioabsorbable screw and the metallic screw in terms of subjective knee joint function and knee laxity, but there appeared to be fewer complications listed in the literature with metallic interference screws. So, it seems that there is no further evidence to support the use of bioabsorbable interference screws. In consideration of the economic benefits, future high-quality RCT studies are needed to obtain a more robust conclusion.
Footnotes
Notes
Final revision submitted January 10, 2021; accepted February 23, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding for this research was provided by the National Natural Science Foundation of China (81972123); Fundamental Research Funds for the Central Universities (2015SCU04A40); The Innovative Spark Project of Sichuan University (2018SCUH0034); Sichuan Science and Technology Program (2020YFH0075); Chengdu Science and Technology Bureau Project (2019-YF05-00090-SN); 1.3.5 Project for Disciplines of Excellence of West China Hospital, Sichuan University (ZY2017301); and 1.3.5 Project for Disciplines of Excellence–Clinical Research Incubation Project, West China Hospital, Sichuan University (2019HXFH039). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.