
Abstract
Background:
Corticosteroid injection and physical therapy remain the mainstay of treatment for idiopathic adhesive capsulitis of the shoulder; however, a certain percentage of patients will not improve using these interventions and will require manipulation under anesthesia (MUA) and/or lysis of adhesions (LOA).
Purpose:
To evaluate whether the immediate pain reduction after fluoroscopic-guided, mixed anesthetic-corticosteroid injection for idiopathic adhesive capsulitis is related to the eventual need for LOA/MUA or a repeat glenohumeral steroid injection.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
This single-institution study involved patients undergoing fluoroscopic glenohumeral corticosteroid injection for a diagnosis of idiopathic adhesive capsulitis between 2010 and 2017. Included were patients with a minimum of 1-year postinjection follow-up and visual analog scale (VAS) pain scores from immediately before and after the injection. The primary analysis was the relationship between patients with an immediate change in VAS score after injection and those who underwent LOA/MUA. A repeat glenohumeral injection was also evaluated as an outcome. Receiver operator characteristic curves and a multivariate binomial logistic regression analysis were performed.
Results:
Overall, 739 shoulders in 728 patients (mean age, 52.6 years; 68% women) were included, of which 38 (5.1%) underwent LOA/MUA and 209 (28%) underwent repeat injections. The immediate change in the VAS score was not significantly associated with the eventual need for LOA/MUA. Preinjection VAS and immediate postinjection VAS scores were not significant predictors of eventual LOA/MUA or subsequent injection. For all 3 predictors, the area under the receiver operator characteristic curve classified them as extremely poor discriminators.
Conclusion:
The immediate pain response to a fluoroscopic-guided glenohumeral injection for idiopathic shoulder adhesive capsulitis was not predictive of the eventual need for LOA/MUA or subsequent injection. Patients can be counseled that even if their initial pain response to an injection is poor, they still have an excellent chance of avoiding surgery, as the overall rate of LOA/MUA was low (5.1%).
Idiopathic adhesive capsulitis of the shoulder, or frozen shoulder, is a debilitating condition characterized by painful and progressive loss of active and passive range of motion. 14 The cause of the condition is poorly understood, but it is believed to be an inflammatory condition that results in restricted range of motion caused by a thickened glenohumeral joint capsule and fibrosis. 17 Adhesive capsulitis is fairly common, with a reported prevalence of 2% to 5% in the general population and around 13% in patients with diabetes mellitus. 2,11,17,25 It is also associated with female sex, thyroid disorders, Dupuytren contractures, and breast cancer treatment. 4,7,19,20,24 Three distinct phases of adhesive capsulitis have been described: (1) an initial painful phase, followed by (2) a period of stiffness and (3) an eventual recovery phase. 17 Without intervention, the process on average takes about 30 months but could last up to 4 years. 11 Historically, adhesive capsulitis was thought to have a self-limiting natural history that, with time, would lead to full recovery without any interventions 13 ; however, more recent studies have refuted this theory and shown that most improvement occurs in the early stages with intervention. 23 Management of adhesive capsulitis remains controversial because of limited high-quality evidence in the literature, but physical therapy, along with intra-articular corticosteroid injections, continues to be the mainstay initial treatment. 3,6,12 Patients who do not improve will typically undergo a second steroid injection and continued therapy before surgery. 14 Younger patients with diabetes mellitus and patients who do not attend formal physical therapy are more likely to need a second steroid injection. 10 If patients do not improve after using several conservative measures, an arthroscopic lysis of adhesions and manipulation under anesthesia (LOA/MUA) is recommended. 14
After steroid injections for idiopathic adhesive capsulitis, patients often report varying degrees of initial pain relief, or the so called “anesthetic effect.” However, it is uncertain if this relief relates to the eventual outcome of the injection. In general, there is a low incidence of surgical intervention, but timing of conservative treatments has been linked to their success. A retrospective study by Hazleman 9 suggested that patients who receive injections earlier in the course of the condition tend to recover quicker. Corticosteroid injection during the early phase of adhesive capsulitis can act as a chemical ablation of the synovitis, thus limiting the fibrotic process and shortening the natural history of the disease. 8 Following that rationale, it is reasonable to assume that patients in the initial (synovitic) stages would have a greater immediate pain response to a corticosteroid injection and better long-term outcomes.
Therefore, the primary objective of this study was to evaluate whether the immediate pain reduction after corticosteroid injection for idiopathic adhesive capsulitis is related to the eventual need for LOA/MUA or a repeat glenohumeral steroid injection. Secondary objectives of the study were to evaluate whether immediate preinjection or immediate postinjection pain scores have any relationship with the same outcomes. We hypothesized that a more significant immediate response to a steroid injection would be correlated with a lower risk of eventual LOA/MUA or a repeat injection.
Methods
Patient Selection
The study protocol was approved by our institution’s health sciences research institutional review board. A retrospective chart review was performed on all patients who underwent fluoroscopic glenohumeral corticosteroid injections at a single academic institution between January 2010 and December 2017. Study inclusion criteria were as follows: (1) fluoroscopic glenohumeral corticosteroid injection, (2) diagnosis of idiopathic adhesive capsulitis of the shoulder, (3) minimum of 1-year postinjection follow-up, and (4) both pre- and postinjection 10-point visual analog scale (VAS) pain scores that were recorded in the electronic medical record. Overall, 739 shoulders in 728 patients who met all study inclusion and exclusion criteria were identified. Of note, only 5 patients were excluded for a lack of both preinjection and postinjection VAS scores, as these are required entries within the electronic medical record when fluoroscopic glenohumeral injections are administered at our institution.
Treatment Protocol
All patients with diagnosis of idiopathic adhesive capsulitis were evaluated by 1 of 6 fellowship-trained, orthopaedic sports medicine attending physicians (including B.C.W., D.R.D., and S.F.B.) before undergoing initial injection. Patients were approved for injection after documentation of loss of passive and active range of motion without other recognized cause was confirmed. At minimum, all patients undergoing injection were evaluated radiographically to rule out other concomitant pathology contributing to shoulder pain and stiffness. Injection was not performed in patients with (1) previous ipsilateral shoulder surgery; (2) a diagnosis of or radiographic evidence of moderate or severe glenohumeral osteoarthritis; (3) concomitant diagnoses of full-thickness rotator cuff tears or calcific tendonitis; or (4) a history of previous trauma to the shoulder, including fracture.
Intra-articular glenohumeral injections were administered into the joint under fluoroscopic guidance via a posterolateral approach using a 20-gauge spinal needle and consisted of 3 mL of 2% lidocaine and 1 mL (40 mg) of triamcinolone acetonide. The composition of the injection was in accordance with the institutional protocol and with previous studies that have utilized intra-articular injections for treatment of adhesive capsulitis. 18 For patients with multiple injections, the first instance of the injection was included, and subsequent injections were recorded as repeat injections. For patients in whom both shoulders were treated at different times for adhesive capsulitis using an injection, each shoulder was included as a separate shoulder.
The preinjection VAS score was recorded with the patient at rest after being positioned for the injection. Per the protocol, the postinjection VAS score was recorded 3 minutes after the injection after the patient had been encouraged to gently mobilize the shoulder in order to distribute the anesthetic evenly throughout the joint. A paper-based VAS was provided to patients at the time of the assessment to assist in their judgment. 5 All VAS pain scores were on a scale from 1 (no pain) to 10 (greatest pain).
Criteria for performing LOA/MUA required failure of at least 3 months of nonoperative management, including a period of physician or therapist-directed physical therapy. The final decision to proceed with surgical intervention was also determined by patient preference and the attending physician’s best clinical judgment.
Data Acquisition
A retrospective chart review of included patients was performed to identify characteristics, medical comorbidities, previous treatments, pre- and postinjection data, follow-up data, repeat steroid injections, and eventual need for LOA/MUA. Baseline data about the included patients is provided in Table 1. The immediate pain reduction from corticosteroid injection was calculated by subtracting the postinjection VAS score from the preinjection score. For patients who had an increase in pain after the injection, these were counted as no improvement, or zero, for statistical purposes. The primary outcome variable assessed was ipsilateral LOA/MUA within 1 year postinjection. The secondary outcome was repeat injections within 1 year postinjection.
Description of Study Patients a (N = 739 Shoulders)
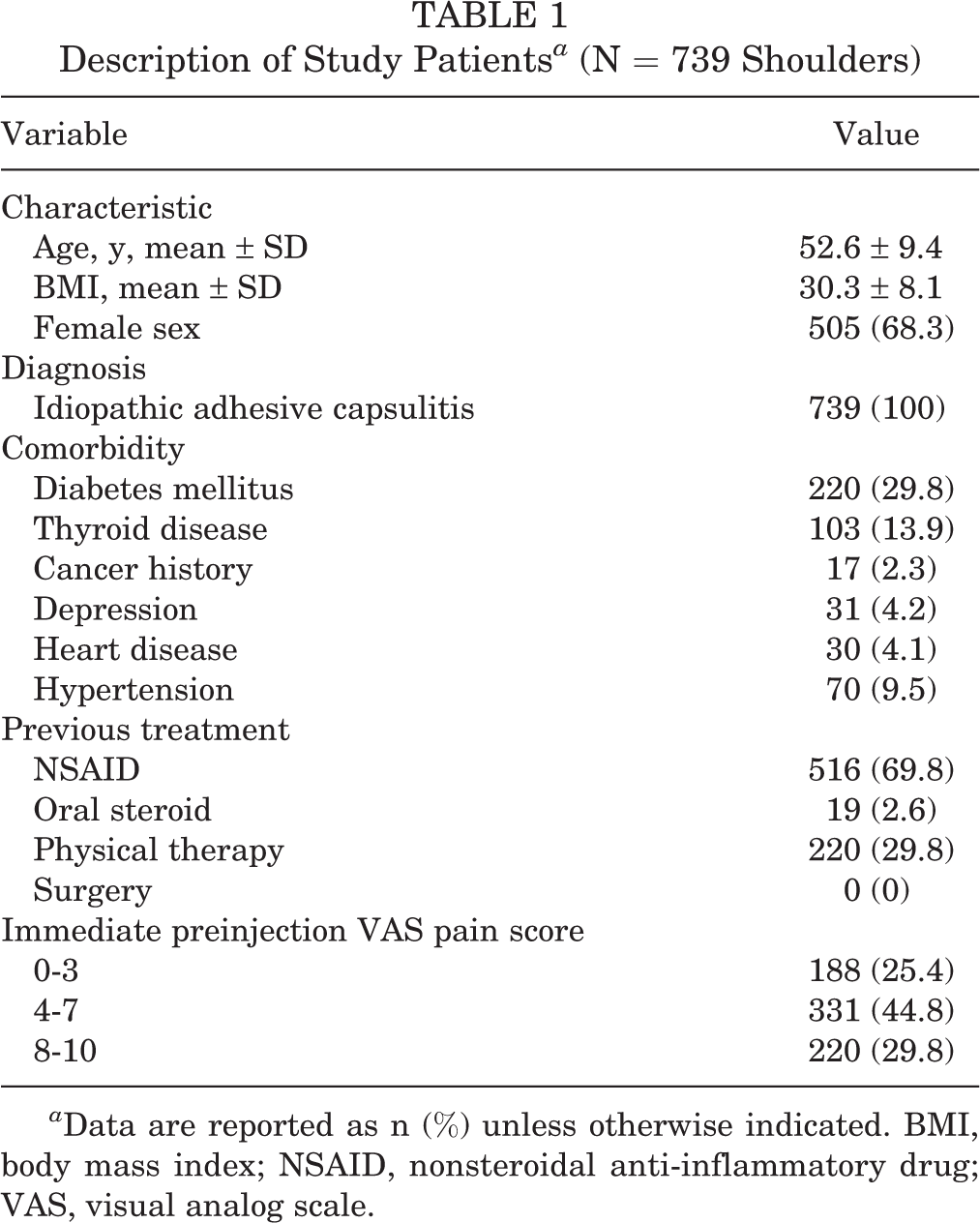
a Data are reported as n (%) unless otherwise indicated. BMI, body mass index; NSAID, nonsteroidal anti-inflammatory drug; VAS, visual analog scale.
Statistical Analysis
All statistical analyses were performed using SPSS Version 26 (IBM Corp). Baseline characteristics were described as means and standard deviations or number of patients and percentages. VAS scores were reported in tertiles for the baseline table; for the remainder of the analysis, VAS scores were considered a continuous variable. Receiver operator characteristic curves (ROCs) were used to determine if a threshold preinjection VAS, postinjection VAS, or VAS improvement existed, above which either study endpoint was more likely to occur. The results of the ROC analysis were reported as area under the curve (AUC), sensitivity, specificity, and a P value indicating significance of any potential threshold. A multivariate binomial logistic regression analysis was used to evaluate whether preinjection and postinjection VAS scores or VAS improvement were significantly associated with eventual LOA/MUA or a repeat injection, while controlling for and evaluating various patient characteristics as potential significant variables. Variables included in the regression in addition to the VAS scores were age, sex, body mass index (BMI), diabetes mellitus, thyroid disease, cancer history, depression, heart disease, and hypertension. For all statistical tests, P < .05 was considered statistically significant.
Results
The mean preinjection VAS score was 5.6 ± 2.7, and the mean postinjection VAS score was 2.3 ± 2.7. Overall, 448 patients (60.6%) saw an improvement of ≤3 points in their VAS score immediately postinjection, while an additional 209 shoulders (28.3%) had a 4- to 7-point improvement. A total of 209 shoulders (28.3%) underwent subsequent steroid injections at a mean of 5.3 ± 6.5 months after the index injection, and 38 shoulders (5.1%) underwent LOA/MUA at a mean of 5.7 ± 4.6 months after the index injection.
Improvement in VAS Score as a Predictor
The immediate improvement in the VAS score from pre- to postinjection was not a good predictor of the eventual need for LOA/MUA or subsequent injection. The rate of eventual LOA/MUA stratified by immediate improvement in pain after the injection is provided in Figure 1, which demonstrates no clear trend and, in fact, the highest rates of LOA/MUA were in patients with more significant anesthetic response to the injection. The improvement in the VAS score was not a useful predictor of LOA/MUA in the ROC analysis, with poor sensitivity and specificity and an AUC of 0.566, which classifies it as a very poor discriminator (P = .169) (Table 2). In the multivariate analysis, improvement in the VAS score did reach statistical significance as a predictor of LOA/MUA (Odds ratio, 1.1; P = .045), but this is of very unlikely clinical significance, particularly in light of the ROC findings (Table 3). Similarly, improvement in the VAS score was not a good predictor of the need for subsequent injection. In the ROC analysis, it had poor sensitivity and specificity, with an AUC of 0.492, classifying it as a very poor discriminator (P = .736) (Table 2). In the multivariate analysis, improvement in the VAS score was not a statistically significant predictor of the need for a repeat injection (P = .578), while lower BMI (P = .037) and diabetes mellitus (P = .040) were predictors of a repeat injection (Table 3).
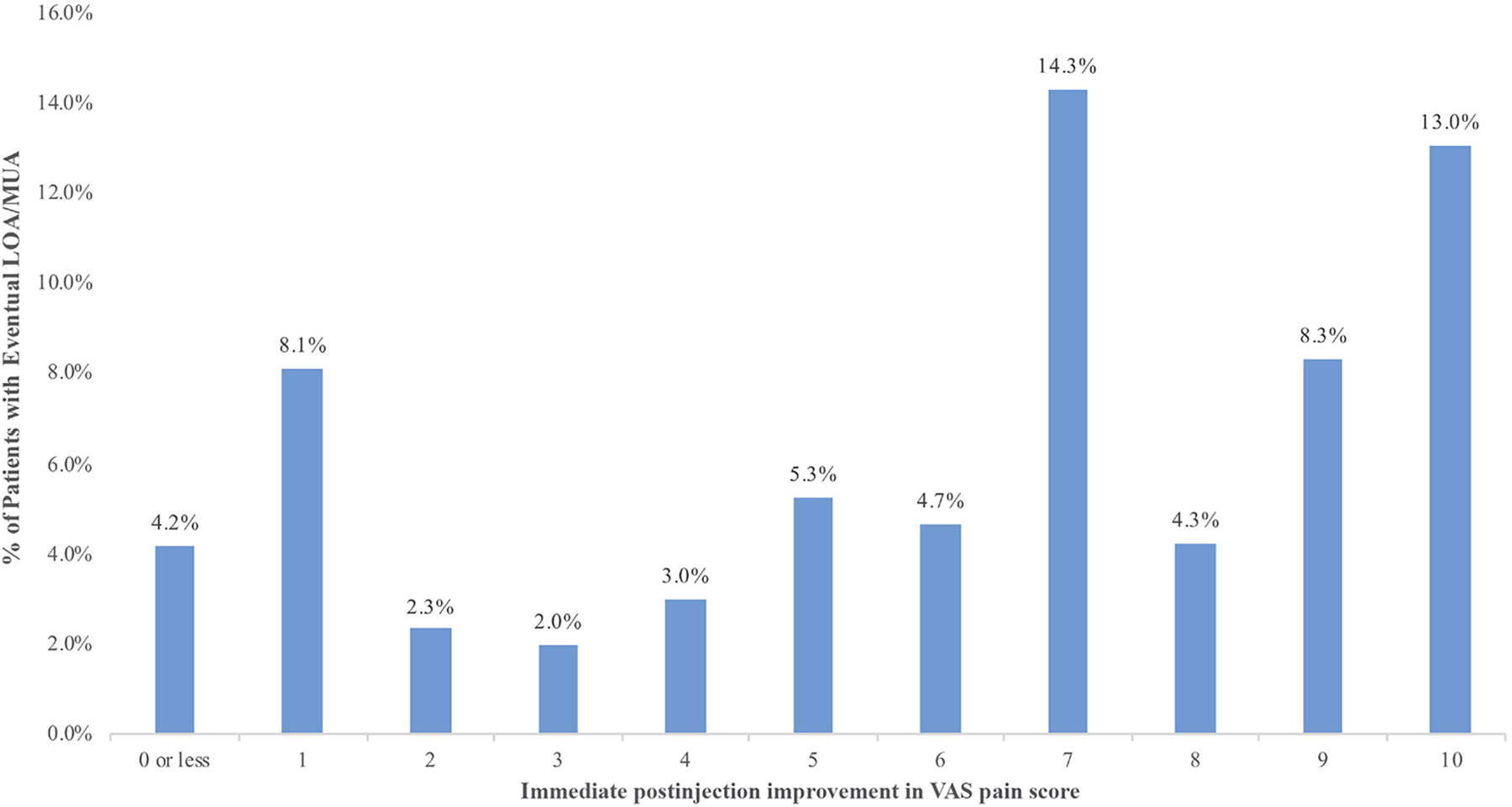
Distribution of LOA/MUA rates stratified by immediate postinjection improvement in the VAS pain score. Immediate postinjection improvement in the VAS score was not a useful predictor of eventual LOA/MUA. LOA, lysis of adhesions; MUA, manipulation under anesthesia; VAS, visual analog scale.
Results of Receiver Operator Characteristic Curve Analysis a

a AUC, area under the curve; LOA, lysis of adhesions; MUA, manipulation under anesthesia; VAS, visual analog scale.
Results of Multivariate Analysis: Predictors of LOA/MUA or Repeat Injection a
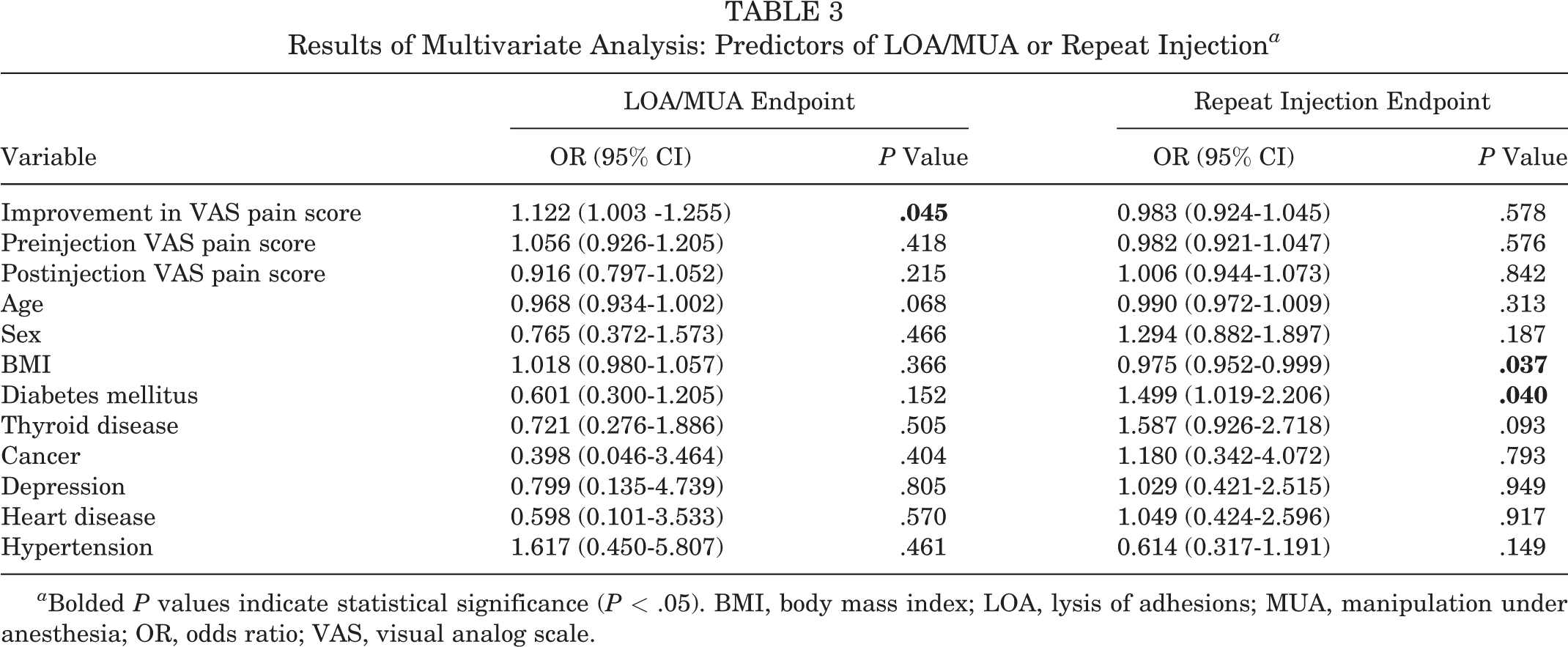
a Bolded P values indicate statistical significance (P < .05). BMI, body mass index; LOA, lysis of adhesions; MUA, manipulation under anesthesia; OR, odds ratio; VAS, visual analog scale.
Preinjection VAS Score as Predictor
The preinjection VAS score was not a good predictor of the eventual need for LOA/MUA or subsequent injection (Figure 2). It was not a useful predictor of LOA/MUA in the ROC analysis, with poor sensitivity and specificity and an AUC of 0.570, which classifies it as a very poor discriminator (P = .148) (Table 2). In the multivariate analysis, the preinjection VAS score was not a statistically significant predictor of LOA/MUA (P = .418) (Table 3). Similarly, the preinjection VAS score was not a good predictor of the need for subsequent injection. In the ROC analysis, it had poor sensitivity and specificity, with an AUC of 0.486, classifying it as a very poor discriminator (P = .552) (Table 2). In the multivariate analysis, the preinjection VAS score was not a statistically significant predictor of a repeat injection (P = .576) (Table 3).

Distribution of LOA/MUA rates stratified by the preinjection VAS score. The preinjection VAS pain score was not a useful predictor of eventual LOA/MUA. LOA, lysis of adhesions; MUA, manipulation under anesthesia; VAS, visual analog scale.
Postinjection VAS Score as Predictor
The postinjection VAS score was not a good predictor of the eventual need for LOA/MUA or subsequent injection (Figure 3). It was not a useful predictor of LOA/MUA in the ROC analysis, with poor sensitivity and specificity and an AUC of 0.464, which classifies it as a very poor discriminator (P = .455) (Table 2). In the multivariate analysis, the postinjection VAS score was not a statistically significant predictor of LOA/MUA (P = .215) (Table 3). Similarly, the postinjection VAS score was not a good predictor of the need for subsequent injection. In the ROC analysis, it had poor sensitivity and specificity, with an AUC of 0.508, classifying it as a very poor discriminator (P = .740) (Table 2). In the multivariate analysis, the postinjection VAS score was not a statistically significant predictor of a repeat injection (P = .842) (Table 3).

Distribution of LOA/MUA rates stratified by immediate postinjection VAS pain score. Immediate postinjection VAS score was not a useful predictor of eventual LOA/MUA. LOA, lysis of adhesions; MUA, manipulation under anesthesia; VAS, visual analog scale.
Discussion
The primary finding of this study was that the immediate anesthetic response to a fluoroscopically guided, mixed anesthetic and corticosteroid glenohumeral injection for idiopathic adhesive capsulitis is not necessarily indicative of the eventual need for LOA/MUA or repeat injections. Therefore, the immediate anesthetic response to an intra-articular injection does not appear to be a good prognostic tool. Similarly, the amount of pain the patient has at the time of injection or the amount of residual pain after the injection are also not predictive of the need for LOA/MUA or a repeat injection.
The affirmation of our study’s null hypothesis in failing to demonstrate the prognostic value of the initial pain response to glenohumeral injection in idiopathic adhesive capsulitis is interesting, as, anecdotally, the authors have typically used the anesthetic response to injections for this condition and others as an indicator of how well the patient would respond to nonoperative treatment. Although the pathophysiology of adhesive capsulitis is not entirely understood, it has been theorized that the disease state progresses from inflammation of the joint capsule into reactive capsular fibrosis, resulting secondarily in decreased range of motion. 15,22 With the earlier disease state being characterized by capsular inflammation and previous evidence from a retrospective study by Hazleman 9 suggesting that the outcome of treatment is partially dependent on the duration of symptoms, it appears plausible that the immediate pain response to a mixed anesthetic corticosteroid injection could have a prognostic value in considering the response to treatment.
Given that adhesive capsulitis is primarily inflammatory and secondarily progresses to fibrosis, the immediate pain response to injection should be indicative of the presence of inflammation within the synovial membrane of the shoulder joint. 14 Diagnosis of inflammation as the primary cause of shoulder pain and loss of range of motion in adhesive capsulitis should indicate the potential for sustained response to the injection of the longer-acting corticosteroid. More progressive adhesive capsulitis, characterized by a greater degree of fibrosis, would therefore be less responsive both to the initial local anesthetic as well as the anti-inflammatory effects of the corticosteroid, and theoretically it would require more extensive treatment and be indicative of an overall poorer response to therapy.
By this theory, we developed our alternative hypothesis that the immediate pain response to a glenohumeral injection for adhesive capsulitis would predict the eventual outcome (ie, range of motion, need for subsequent injection, and need for LOA/MUA). Despite this support in theory, we did not find that this association manifested clinically. In fact, the highest rates of LOA/MUA observed in our study population were among patients with more significant anesthetic response. It may be possible that this observation is representative of these patients having more severe inflammation, which may make them more resistant to resolution of symptoms using 1 or more injections. In conclusion, however, this study was unable to detect an association between the immediate change in VAS pain scores after injection, or the preinjection and postinjection VAS pain scores, and our primary and secondary outcomes of interest.
There are numerous potential reasons why a response was not observed. The 3-minute VAS response may have been measured before the local anesthetic could penetrate deep into the affected synovial tissue. Similarly, the effect of the steroid may be a better predictor than is the response to the local anesthetic; thus, future work should investigate the response up to 7 days postinjection. In addition, adhesive capsulitis may represent a pathological process that involves more than the synovium, which would make intra-articular injections alone not completely effective. For this reason, authors have recommended and reported success using other periarticular injections, such as subacromial 16 or rotator interval injections. 21
A significant association was observed between both diabetes mellitus and obesity and the need for repeat injections. This finding, while not surprising, should be used when counseling patients with these comorbidities about their likelihood of successful resolution of symptoms after a single injection for adhesive capsulitis. Although these comorbidities were not significantly associated with the need for eventual LOA/MUA, this could be due to type I error because of the overall low incidence of LOA/MUA.
Our findings are also interesting considering other supporting evidence for our alternative hypothesis that exists in the spine literature. In a study of lower back pain and radiculopathy, it has been shown that a favorable immediate pain response to injection of bupivacaine and corticosteroids was predictive of the treatment response for inflammatory mediated lower back pain. 1 In a study by Bartynski et al, 1 who examined this phenomenon, the immediate pain response was postulated to be due to the direct action of bupivacaine on the active epidural, neural, or perineural pain generators related to irritation from inflammatory byproducts. Therefore, pain that was not related to this inflammatory process did not generate a significant pain response to the injection. Hence, the immediate response was an indicator of the location of inflammation and a predictor of sustained response to treatment using anesthetic/corticosteroid injections without the need for more aggressive treatment in the long term. 1 This type of clinical association was not observed in the present study.
Despite not demonstrating a prognostic value in the immediate pain response to glenohumeral injection for idiopathic adhesive capsulitis, the findings from our study still prove valuable to surgeons and clinicians. The lack of association observed in our study can be used to counsel patients who demonstrate both excellent and poor initial responses to injections in order to set realistic treatment expectations. The overall rate of LOA/MUA was quite low, and thus patients can be comfortable with the knowledge that regardless of their initial response to the injection for adhesive capsulitis, they are unlikely to proceed to LOA/MUA within 1 year after the injection.
Limitations
Despite our findings, our study does have several limitations. Because of its retrospective nature, it is challenging to ensure that confounding variables were optimally controlled. For example, we were unable to determine whether patients were participating in physical therapy during the treatment period or to control for the number of therapy sessions they received during the treatment interval. Despite this limitation, our large number of included patients helps to offset the potential effect of these confounders. Also, our study was not able to determine the timepoint of symptom onset or duration of symptoms in relation to the date of injection, which has been shown to correspond with treatment outcome. 9 There may be a correlation between anesthetic response and outcome in patients in the acute inflammatory phase with a shorter duration of symptoms, for which we were not able to reliably assess. In addition, our evaluation included only a single evaluation of the VAS at 3 minutes postinjection. The outcomes may differ if assessed an hour postinjection or up to a week postinjection. Moreover, this study only looked at intra-articular injections. The results of this study cannot be extrapolated to rotator interval or subacromial injections. Despite including a large number of patients, the relative incidence of LOA/MUA was small, which increases the risk for type I error that could bias the results. Finally, we were not able to consistently assess range of motion or postinjection symptoms other than the immediate response or need for repeat injections or LOA/MUA. Patients may be reluctant to undergo MUA/LOA despite lack of improvement, and therefore we may be underestimating the true number of patients with a poor result from an injection. Despite its limitations, this study still offers valuable information. The information can be used clinically when counseling patients or in adding objective data to determining a plan of treatment for patients with this condition.
Conclusion
In the current study, the immediate pain response to a fluoroscopically guided glenohumeral injection for idiopathic adhesive capsulitis of the shoulder was not predictive of the eventual need for LOA/MUA or subsequent injection. Patients can be counseled that even if their initial pain response to an injection is poor, they still have an excellent chance of avoiding surgery, as the overall rate of LOA/MUA is low.
Footnotes
Final revision submitted January 5, 2021; accepted February 18, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.T.A. has received education payments from Arthrex and hospitality payments from Stryker. T.E.M. has received royalties from Zimmer Biomet. D.R.D. has received consulting fees from Medical Device Business Services and Mitek; research support from Aesculap/B. Braun, Moximed, and Zimmer Biomet; royalties from Smith & Nephew and Springer; and hospitality payments from OsteoCentric. S.F.B. has received research support from Arthrex and Biomet; consulting fees from Arthrex, Biomet, Exactech, Heron Therapeutics, MicroAire Surgical Instruments, Zimmer Biomet, and WRS; royalties from Biomet, Exactech, Springer, and Zimmer Biomet; and hospitality payments from Supreme Orthopedics Systems. B.C.W. has received consulting and speaking fees from Arthrex; research support from Arthrex, Biomet, Flexion Therapeutics, and Integra LifeScience; and education payments from Supreme Orthopedics Systems. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from University of Virginia (IRB-HSR #:19938).