
Abstract
Background:
The use of the interference screw (IFS) for the cortical fixation of tendon grafts in knee ligament reconstruction may lead to converging tunnels in the multiligament reconstruction setting. It is unknown whether alternative techniques using modern suture anchor (SA) or bone staple (BS) fixation provide sufficient primary stability.
Purpose:
To assess the primary stability of cortical fixation of tendon grafts for medial collateral ligament (MCL) reconstruction using modern SA and BS methods in comparison with IFS fixation.
Study Design:
Controlled laboratory study.
Methods:
Cortical tendon graft fixation was performed in a porcine knee model at the tibial insertion area of the MCL using 3 different techniques: IFS (n = 10), SA (n = 10), and BS (n = 10). Specimens were mounted in a materials testing machine, and cyclic loading for 1000 cycles at up to 100 N was applied to the tendon graft, followed by load-to-failure testing. Statistical analysis was performed using 1-way analysis of variance.
Results:
There were no statistical differences in elongation during cyclic loading or peak failure load during load-to-failure testing between BS (mean ± standard deviation: 3.4 ± 1.0 mm and 376 ± 120 N, respectively) and IFS fixation (3.9 ± 1.2 mm and 313 ± 99.5 N, respectively). SA fixation was found to have significantly more elongation during cyclic loading (6.4 ± 0.9 mm; P < .0001) compared with BS and IFS fixation and lower peak failure load during ultimate failure testing (228 ± 49.0 N; P < .01) compared with BS fixation.
Conclusion:
BS and IFS fixation provided comparable primary stability in the cortical fixation of tendon grafts in MCL reconstruction, whereas a single SA fixation led to increased elongation with physiologic loads. However, load to failure of all 3 fixation techniques exceeded the loads expected to occur in the native MCL.
Clinical Relevance:
The use of BS as a reliable alternative to IFS fixation for peripheral ligament reconstruction in knee surgery can help to avoid the conflict of converging tunnels.
Owing to favorable primary stability, interference screw (IFS) fixation is a widely used technique for tendon graft fixation in ligament reconstruction of the knee. 2 However, the creation of the required bony socket may lead to converging tunnels compromising the postoperative outcome, especially in the multiligament reconstruction setting or in combination with an osteotomy. 11,12,23
Converging tunnels may occur especially on the femoral side when an anterior cruciate ligament (ACL) reconstruction is combined with an anterolateral tenodesis or posterolateral reconstructions or when a posterior cruciate ligament reconstruction is combined with a medial collateral ligament (MCL) reconstruction. Recent studies have focused on possible solutions to avoid converging tunnels by changing the orientation or angulation of the bone socket. 12,23 The risk of converging tunnels could thereby be reduced but not entirely avoided. 12,23 The use of an extracortical fixation device, such as suture anchors (SA) or bone staples (BS), may be an answer to solve this dilemma, as these devices do not require a large tunnel for peripheral ligament reconstruction.
Other possible advantages of a BS fixation would be the lower costs per implant as well as a better replication of the flat insertion site of native ligaments, such as the tibial MCL insertion site, 21 which to date is mainly reconstructed using semitendinosus, gracilis, or Achilles tendon and IFS fixation. 5 However, it is unknown whether alternative fixation techniques such as modern SA or BS would provide sufficient primary stability to be considered a reliable alternative to cortical fixation of a tendon graft in knee ligament reconstructions.
Thus, the aim of the present study was to evaluate the primary stability of cortical fixation of tendon grafts in MCL reconstruction using BS and SA in comparison with IFS fixation. We hypothesized that the primary stability of BS and SA fixation would not be inferior to that of IFS fixation.
Methods
Fresh porcine tibias and flexor tendons were obtained from a local butcher. The following devices were commercially purchased: bioabsorbable polylactide Interference Screw Megafix B (6 × 23 mm; n = 10) (Karl Storz), Richards Bone Staple with spikes (width, 8 mm; arm length, 15 mm; n = 10) (Smith & Nephew), and double-loaded titanium Corkscrew FT II Suture Anchor (n = 10) (Arthrex). No ethical approval was needed for this study.
Testing Setup
A total of 30 porcine knee specimens were gently defrosted, dissected, and mounted in a metal cylindrical container using synthetic resin (RenCast FC 52/53 A ISO and Ren Cast FC 53 B Polyol; Gößl & Pfaff). The cylindrical container was firmly attached to the socket of the materials testing machine (Model 8874; Instron). Then, 30 porcine flexor tendons of the knee joint were dissected to a diameter of 6 mm and a length of 80 mm in order to match the length and thickness of a standard human MCL graft. The diameter of the tendons was measured using a standardized sizing device (±0.5 mm) (Karl Storz).
Fixation Techniques
IFS fixation was performed in the control group (n = 10). A transverse bicortical tunnel with a length of 40 to 50 mm and a diameter of 6 mm was created in the center of the tibial insertion area of the MCL. A bicortical tunnel was chosen to standardize the technique and avoid technical bias, although clinically a monocortical tunnel is beneficial. The distal end of the tendon graft was sutured using the Krackow stitch technique with 4 stitches on each side 17 using a polyethylene suture (No. 2 FiberWire; Arthrex) and pulled into the tunnel from the anteromedial to the anterolateral surface of the proximal tibia, creating a tendon-bone interface of 20 mm in length. A nitinol wire was inserted into the tunnel guiding the 6 × 23–mm IFS from the anteromedial cortex to an intracortical position placed flush to the bone surface (Figure 1C).

Fixation of the tendon graft using (A) bone staple, (B) suture anchor, and (C) interference screw at the medial collateral ligament insertion site of the porcine tibiae.
SA fixation was performed in the first intervention group (n = 10). The SA was inserted in the center of the tibial insertion area of the MCL according to the instructions of the manufacturer of the implant. The tendon graft was tied to the suture anchor using the 2 loaded polyethylene sutures (No. 2 FiberWire and No. 2 TigerWire; Arthrex). One arm of each suture was passed through the tendon graft using the Krackow stitch technique starting from the distal portion with 4 stitches up and 4 stitches back down. The second arm of the respective suture was passed through the tendon graft once and then tied to the first arm of the loop using 10 surgical half stitches. This procedure was performed with both sutures (Figure 1B).
BS fixation was performed in the second intervention group (n = 10). The distal end of the tendon graft was sutured using the Krackow stitch technique with 4 stitches on each side using a polyethylene suture (No. 2 FiberWire). The tendon graft was then fixed to the center of the tibial insertion area of the MCL under the BS, which was inserted perpendicular to the bony surface of the proximal tibia using an orthogonal orientation to the tendon graft (Figure 1A).
Biomechanical Testing
Envelope randomization was used to determine the order of testing. A servohydraulic uniaxial testing machine (Model 8874; Instron) was used for cyclic testing. The accuracy of the load cell was ±0.005%, allowing a position control with an accuracy of ±0.5% for the testing unit. A cylindrical container was fixed to the base of the machine using 2 clamps. The free end of the graft was fixed to the testing machine using a cryoclamp, leaving 20 mm of free graft between the clamp and the joint line. The orientation of the tendon graft and the force vector was perpendicular to the joint line of the proximal tibia, corresponding to a worst-case scenario of load applied to an MCL graft (Figure 2). Before testing, a 20-N pretension was applied to the construct by manually positioning the crossbar of the machine.

Testing setup in the servohydraulic uniaxial testing machine using a cryoclamp for the medial collateral ligament graft.
A test protocol was designed using 10 cycles at a load of 50 N for preconditioning. The cyclic testing protocol included 500 loading cycles for each step at 50 and 100 N at a rate of 1 Hz, based on the loads thought to occur in the native MCL in the ACL-intact (50 N) and ACL-deficient (100 N) knee during normal gait. 18,19,22 Elongation and load were recorded continuously. Next, cyclic load-to-failure testing was conducted at a rate of 25 mm/min. Stiffness was determined using the slope of the linear portion of the load-displacement curve during load-to-failure testing. Yield load was determined using the load-elongation curve according to Martin et al. 15 The mode of failure was macroscopically documented.
Statistical Analysis
A power analysis before this study showed that a sample size of 10 per group would lead to a 90% power to detect a difference of 50 N between means at the ß ≥ 0.8 level based on the standard deviations (SDs) found in cyclic testing of tendon graft fixations in porcine knee models. 10,20
For statistical analysis, a 1-way analysis of variance for multiple comparisons was performed. Post hoc testing with Bonferroni correction was used to control for multiple comparison. A P value < .05 was required to identify significant differences. The data are presented as mean ± SD. Statistical analysis was performed using Matlab (R2020a; MathWorks) and PRISM Version 8 (GraphPad Software).
Results
Elongation after 500 cycles at 50-N elongation was 1.2 ± 0.2 mm in the BS group, 1.7 ± 0.6 mm in the IFS group, and 2.8 ± 0.4 mm in the SA group. After 1000 cycles of loading (500 cycles at 50 N and 100 N each), elongation was 3.4 ± 1.0 mm in the BS group, 3.9 ± 1.2 mm in the IFS group, and 6.4 ± 0.9 mm in the SA group. A statistically significant difference was found in elongation between BS and SA fixation at 50 and 100 N (P < .0001) and between IFS and SA fixation at 50 and 100 N (P < .0001). BS and SA fixation yielded comparable elongation during cyclic loading up to 100 N (P = .95). No construct failure was observed during cyclic loading (Figure 3A).

Boxplots presenting mean (horizontal line), SD (whiskers), and range (box) for (A) elongation after cyclic loading at 100 N, (B) load to failure, and (C) yield load. Significant difference between groups: **P < .01; ***P < .001; ****P < .0001. BS, bone staple; IFS, interference screw; SA, suture anchor.
Load to failure for the BS (376 ± 120.0 N) and the IFS groups (313 ± 99.5 N) was not significantly different (P = .43). Load to failure for SA fixation (228 ± 49.0 N) was significantly lower compared with BS fixation (P < .01) but not significantly different compared with IFS fixation (Figure 3B). IFS fixation provided a stiffness more than twice that of the SA group (P < .01). No significant difference was found between stiffness of the IFS and BS groups. Yield load was 209 ± 35.6 N in the BS group and 204 ± 41.1 N in the IFS group (Figure 3C). A significant difference was found between yield load of the SA group (146 ± 16.6 N) and those of the BS and IFS groups (P < .01 for both).
The mode of failure was tendon pullout in all 10 specimens of the IFS group and in 9 of 10 specimens of the BS group. In 1 specimen, load to failure led to a proximal tilt, followed by pullout of the BS; however, elongation at 100 N (2.5 mm) and load to failure (438 N) in this specimen did not differ from the rest of the BS group (Table 1). A rupture of the suture fixation inside the SA was observed in all specimens of the SA group. Neither the 5.5-mm titanium screw nor the sutures from the tendon graft showed signs of loosening. There was no damage to the cortex of the bone, no tendon lengthening, and no slippage at the cryoclamp fixation in any specimen of all groups after load to failure.
Elongation, Load to Failure, Stiffness, and Yield Load a
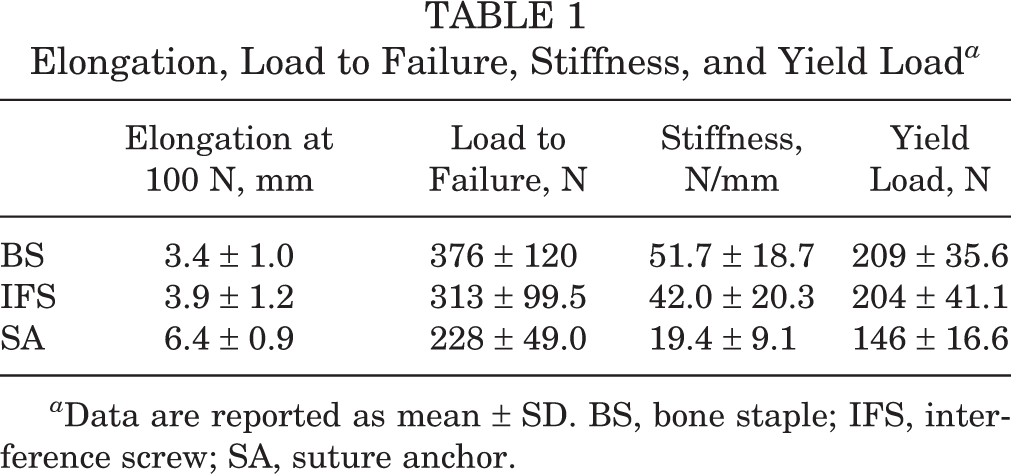
a Data are reported as mean ± SD. BS, bone staple; IFS, interference screw; SA, suture anchor.
Discussion
To our knowledge, the present study was the first to assess primary stability of BS in the cortical fixation of tendon grafts in knee surgery and compare it with IFS and SA fixation. The most important finding of this study was that primary stability of cortical fixation of tendon graft in MCL reconstruction using BS was not inferior to that of IFS fixation in a porcine knee model. Contrary to our hypothesis, the primary stability of the tested SA was inferior to that of the IFS and BS.
Morrison 18,19 determined the maximum loads of the MCL during normal gait and while climbing up and down stairs to be as high as 129 N. Shelburne et al 22 calculated the peak force of the native MCL during walking to be 34 N and found an increase in MCL peak force for the ACL-deficient knee (114 N). In the present study, tibial fixation of an MCL graft was simulated in a porcine knee model in order to compare the primary stability of 3 different devices. Considering the limitations of this time-zero biomechanical testing in an animal knee model, the failure loads of BS, IFS, and SA fixation in the present study were found to be well above the values determined by Morrison 18,19 and Shelburne et al. 22 In the clinical setting of MCL reconstruction, rehabilitation protocols including partial weightbearing and use of a knee joint brace protect the tendon graft and its cortical fixation sides in the early postoperative period. 5 In the present study, elongation after cyclic loading at 50 and 100 N was increased in tendon graft fixation for a single SA. However, primary stability of all 3 fixation techniques was less than the ultimate strength (557 N) and stiffness (63 N/mm) of the native MCL determined by Wijdicks et al. 25
The use of SA and BS for graft fixation in MCL reconstruction has been described in few noncontrolled clinical studies showing acceptable or good clinical outcome. 5,13 DeLong and Waterman 5 summarized the outcome of MCL reconstruction techniques in a systematic review and found no difference between fixation techniques. BS fixation has further been used in MCL repair to achieve reattachment of the torn ligament, 4 in total knee arthroplasty, 24 and for anterolateral tenodesis. 9
Apart from clinical data, there have been only a limited number of biomechanical studies regarding graft fixation techniques in reconstruction of peripheral ligaments of the knee. Omar et al 20 compared fixation of the tendon graft in MCL reconstruction using 4.0-mm cancellous screws and different types of washers or a titanium suture anchor in a porcine knee model. They found that spiked PEEK washers (Synthes) secured using polyester sutures yielded superior biomechanical properties at time zero for both elongation during cyclic loading (2.9 ± 0.7 mm) and ultimate failure load (469.8 ± 64.3 N). Although a different testing setup was used, load to failure of SA fixation was comparable with the results of the present study, whereas BS fixation was not tested. 20
Previously, primary stability of BS fixation of tendon grafts was only assessed for cortical fixation of ACL grafts. Matthai et al 16 found the primary stability of a bone--patellar tendon—bone graft tied to a bone staple in a bovine knee model (726 N) to be comparable with IFS and suture after fixation using a screw. Letsch 14 compared cortical fixation techniques of synthetic ACL grafts in human distal femora. They found a maximum load of 508 ± 51 N for a single staple and 1210 ± 32 N for double staples in a belt-buckle technique. Bargar et al 1 tested the isolated pullout strength of BS without fixation of a graft at the lateral femoral condyle in a canine model compared with a 6.5-mm cancellous bone screw. The pullout load of the BS increased from time point zero to 6 weeks (500 ± 130 N) and was inferior to that of the 6.5-mm cancellous bone screw (1120 ± 490 N). However, comparison with the results of the present study is limited because of different testing setups, ligament reconstructions, and type of specimens.
The results of the present study are of clinical relevance, considering that opting for a BS for cortical fixation of an MCL graft may imitate the broad tibial insertion site of the MCL more closely than would an IFS fixation. Staple fixation may reduce the risk of poor primary stability in the elderly 6,8 and tunnel conflicts in the multiligament reconstruction setting. 3,11,12,23 Furthermore, of the 3 devices tested in the present study, BS was the most economic solution, with a price of approximately $75 per implant, whereas IFS and SA had higher costs ($200 per implant).
When using BS for ligament reconstruction, healing is assumed to occur as the implant is surrounded with necrosis of the tendon graft deep to the BS. 1 Therefore, the tendon graft may also be attached to the surrounding periosteum using sutures. In SA and IFS fixation, the implant is entirely buried within and beneath the cortex, with the depth of the BS arm (15 mm) being similar to that of the IFS (23 mm). Nevertheless, the extracortical portion of the BS may lead to soft tissue irritations that may require implant removal in some cases. 4,9,24 Furthermore, accidental epiphysiodesis has to be avoided in the BS fixation of tendon grafts in children and adolescents.
The results of this study cannot be directly transferred to the clinical setting without a careful interpretation of its limitations. Porcine tibiae and porcine flexor tendons were used to simulate the tibial fixation of a tendon graft in MCL reconstruction. Although it has been previously shown that porcine tendons have similar characteristics to those of the human semitendinosus tendon 7 and that the porcine knee best mimics the anatomy and biomechanics of the human knee, 26 the data of the present study cannot be directly transferred to the human clinical setting. Moreover, some of the porcine flexor tendons were trimmed to a diameter of 6 mm, which may have altered biomechanical properties. Another limitation of the present study was that exact descriptive data of the porcine specimen were not assessable. However, young age and therefore good bone mineral density were confirmed by the butcher. The biomechanical testing simulated forces acting at time zero, where biological factors and graft healing were not taken into account. Furthermore, unidirectional testing was chosen in order to simulate a worst-case scenario but may not mimic the forces acting in vivo, and load to failure was applied after cyclic loading of the construct.
The present study only tested 1 product for each fixation method. Several other products are available and may present different ultimate strength and stiffness values. The SA always failed at the suture fixation inside the anchor, which may have been different in a different type of SA. Furthermore, graft fixation using a second SA or BS may further improve primary fixation stability. 14,20 A comparison of primary stability using different staple designs may be the goal of future studies.
Conclusion
In the current study, BS and IFS fixation provided comparable primary stability in the cortical fixation of tendon grafts in MCL reconstruction, whereas a single SA fixation led to increased elongation with physiologic loads. However, load to failure of all 3 fixation techniques exceeded the loads expected to occur in the native MCL.
Footnotes
Acknowledgment
The authors thank Jens Wermers, MSc, for his contribution to the study conception and design and acquisition of data.
Final revision submitted March 29, 2021; accepted April 14, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: Support for this study was received from the Open Access Publication Fund of the University of Münster. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.