
Abstract
Background:
Focus on the importance of hip muscle strength in patients with patellofemoral pain syndrome (PFPS) has recently increased. It is unknown whether patients with PFPS will benefit more from hip strengthening compared with traditional knee-based strengthening.
Purpose:
To compare the efficiency of isolated hip strengthening versus traditional knee-based strengthening for patients with PFPS.
Study Design:
Systematic review; Level of evidence, 2.
Methods:
We conducted a search for studies comparing isolated hip strengthening and knee-based strengthening by using the MEDLINE, Embase, and Cochrane Library electronic databases. The methodological quality of included studies was assessed using the PEDro scale. Predetermined variables from each study were extracted and analyzed.
Results:
A total of 5 comparative studies were included in this review; all studies were of moderate to high quality and reflected good internal and external validity. Pain (visual analog scale [VAS]) and function (Anterior Knee Pain Scale) scores improved in both the hip and knee groups after strengthening intervention, although no statistically significant differences were seen between groups in the pooled analysis. In 2 studies, VAS pain scores were reduced earlier for patients in the hip group than for those in the knee group (P < .05). In 1 study, improvement in Western Ontario and McMaster Universities Osteoarthritis Index function scores in the hip group was statistically superior compared with those in the knee group after intervention and at 6-month follow-up (P < .05). In 2 studies, patients in the hip group exhibited statistically greater hip abductor and extensor strength than did those in the knee group after intervention (P < .05).
Conclusion:
The best-available evidence suggests that overall, isolated hip strengthening and knee strengthening were equivalent for treatment of PFPS.
Patellofemoral pain affects a large proportion of the population, from adolescents (annual prevalence, approximately 29%) to adults (annual prevalence, approximately 23%), and carries a substantial personal and societal burden. 5,30 Patellofemoral pain syndrome (PFPS) is caused by a complex interplay among various anatomic, biomechanical, psychological, social, and behavioral factors. 25 Numerous studies have interpreted anatomic and biomechanical factors for PFPS. Traditionally, research and clinical practice have focused on an imbalance between the vastus lateralis and the vastus medialis oblique that can lead to increased lateral stress in the patellofemoral joint. 7,8,32 Abnormal patellar tracking secondary to an imbalance in quadriceps muscle performance results in PFPS. Nonoperative treatments have focused mainly on developing strength and balance in quadriceps muscles, especially the vastus medialis oblique. 3,6,15 Although quadriceps exercise is the most commonly prescribed intervention, many patients experience a decrease in pain and dysfunction but not total resolution. 3,21,34
More recently, PFPS has been proposed to be related to strength deficits of the hip musculature and core endurance. 19,22,26 A dynamic weightbearing imaging study suggested that increased femoral internal rotation results in increased lateral patellar displacement and lateral tilt and resultant increased stress in the patellofemoral joint. 24 This suggests that unbalanced hip muscle performance may be a contributing factor to PFPS. In biomechanical studies, persons with PFPS have demonstrated excessive hip internal rotation and hip adduction as well as weak muscle performance of the hip abductors, external rotators, and hip extensors compared with pain-free individuals. 23,31
Recent studies have reported promising results when hip muscle strengthening for PFPS is used before traditional programs of knee-strengthening training. 1,12,13,17,20,28 Ismail et al 17 reported that the addition of hip muscle strengthening to a knee-strengthening program resulted in better improvement in pain control during functional activities compared with the knee program alone. Nakagawa et al 20 found that additional strengthening of hip abductor and lateral rotator muscles improved perceived pain during functional activities and increased gluteus medius electromyographic activity during isometric voluntary contraction after 6 weeks of treatment compared with a control condition that entailed quadriceps strengthening.
Hip and knee strengthening are both advocated in treating PFPS. 2,5 However, the relative contributions of the components have yet to be elucidated. In recent years, many studies have compared the effectiveness of isolated hip strengthening versus knee-based strengthening in terms of improving pain, function, and strength, with inconsistent conclusions. 4,10,11,16,18,27 Considering the recent therapeutic interest and controversy regarding isolated hip strengthening for PFPS, we conducted this review to examine the current evidence and to determine the effectiveness of isolated hip strengthening compared with traditional knee-based strengthening for patients who have PFPS. Information obtained from this review will assist clinicians in better prescribing strengthening exercises for PFPS.
Methods
Search Strategy
A literature search was conducted using MEDLINE, Embase, and Cochrane Library databases on September 10, 2019. This study was reported in line with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) and AMSTAR (Assessing the Methodological Quality of Systematic Reviews) guidelines. The following keywords were used for searches: “patellofemoral pain,” “hip,” “knee,” and “physical therapy and/or rehabilitation.” Reference lists of included studies were searched to ensure that no eligible studies were missed.
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: (1) participants: patients with diagnosed PFPS and a minimum 3-month history of anterior or retropatellar knee pain during activities and present on at least 1 clinical test; (2) outcomes: pain relief, functional improvement, and muscle strength endurance; and (3) study design: comparative clinical studies (randomized controlled trials [RCTs] and prospective comparative studies) that compared isolated hip strengthening versus traditional knee-based strengthening for PFPS.
The exclusion criteria were (1) studies that included patients with recent knee surgery, trauma, or coexisting osteoarthritis and (2) studies that entailed a multijoint strengthening program.
Quality Assessment
Methodological quality of included studies was assessed using the PEDro scale, developed for the Physiotherapy Evidence Database. 33 “Yes” is equivalent to 1 point on the scale and is assigned only if the criteria are specifically stated within the text. “No” is assigned to categories not specifically stated within the text. Articles with more “yes” scores on the PEDro scale are of higher quality given the scale of the assessment. For such articles, the analysis was performed independently by 2 evaluators (Y.N. and C.H.), and disagreements were resolved via discussion and consensus.
Data Collection
The following data were collected from each included study by 2 reviewers (Y.S. and Y.Z.) independently: first author, publication year, study design, sample size, mean age of patients, level of evidence, rehabilitation duration, muscle strengthening protocol, and major outcomes. The following clinical outcome measures were collected and compared: visual analog scale (VAS) for pain, Anterior Knee Pain Scale (AKPS), and hip and knee muscle strength endurance.
The reviewers were not blinded to information on authors, journal of publication, or source of financial support. Methodological quality was evaluated for each study. Disagreements were discussed and resolved by referencing the original article. The full text of articles was read, with a focus on authors and methods, to identify studies that involved the same group of patients.
Statistical Analysis
Data analysis was performed via Cochrane Review Manager 5.3 (Cochrane Collaboration, Nordic Cochrane Centre). Continuous data (VAS and AKPS scores) were measured as mean difference (MD) with 95% confidence interval (CI). P < .05 was considered statistically significant. Heterogeneity among included studies was assessed using the Q statistic and I2 test. 32 If P > .05 or I2 < 50%, the included studies were considered to have low heterogeneity, and the fixed-effects model was applied to outcome data; otherwise, the random-effects model was applied.
Results
Search Results
The search strategy produced 507 records on this topic. A total of 494 articles were excluded after screening of titles and abstracts according to predetermined topic and inclusion criteria. Of the remaining 13 studies identified for possible inclusion, 7 studies were excluded because they did not directly compare hip and knee strengthening for PFPS. A study by Bolgla et al 4 was excluded because it was a secondary analysis of the same patients studied by Ferber et al. 11 Thus, 5 comparative studies (4 RCTs and 1 prospective comparative study) were included. 10,11,16,18,27 A PRISMA flow diagram is presented in Figure 1.
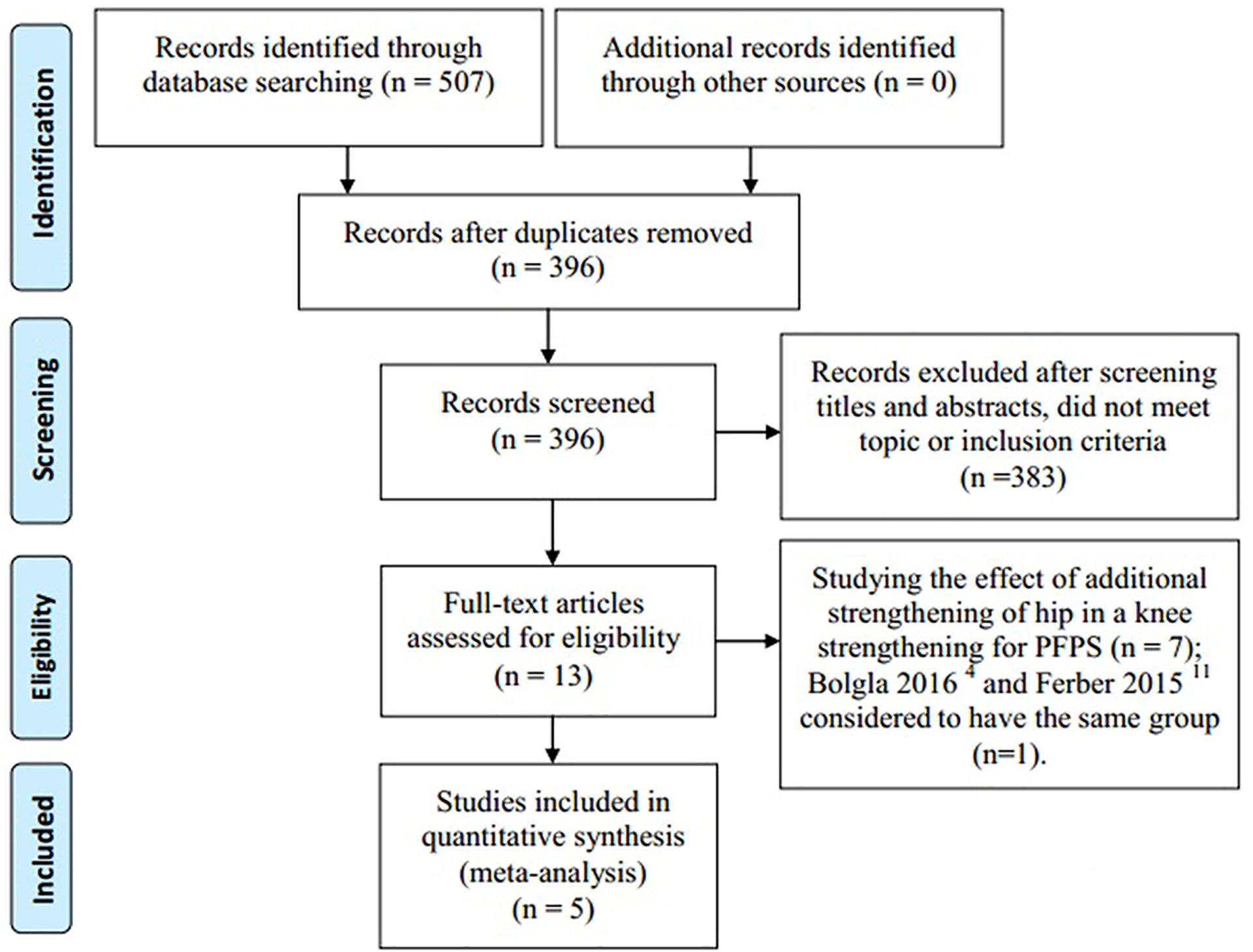
Flow diagram of study selection using PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses). PFPS, patellofemoral pain syndrome.
Characteristics of the Included Studies
Detailed information regarding the included studies is presented in Table 1. The 5 articles included in this systematic review involved 364 patients; there was a predominance of female patients in all studies. The mean age of patients ranged from 22.5 to 29.0 years. Details of the intervention and outcomes of the included studies are presented in Table 2.
Characteristics of the Included Studies a

aDash indicates that corresponding information was not given. BMI, body mass index; F, female; H, hip-strengthening group; K, knee-strengthening group; M, male; PCS, prospective comparative study; RCT, randomized controlled trial.
Summary of Interventions and Outcomes of the Included Studies a
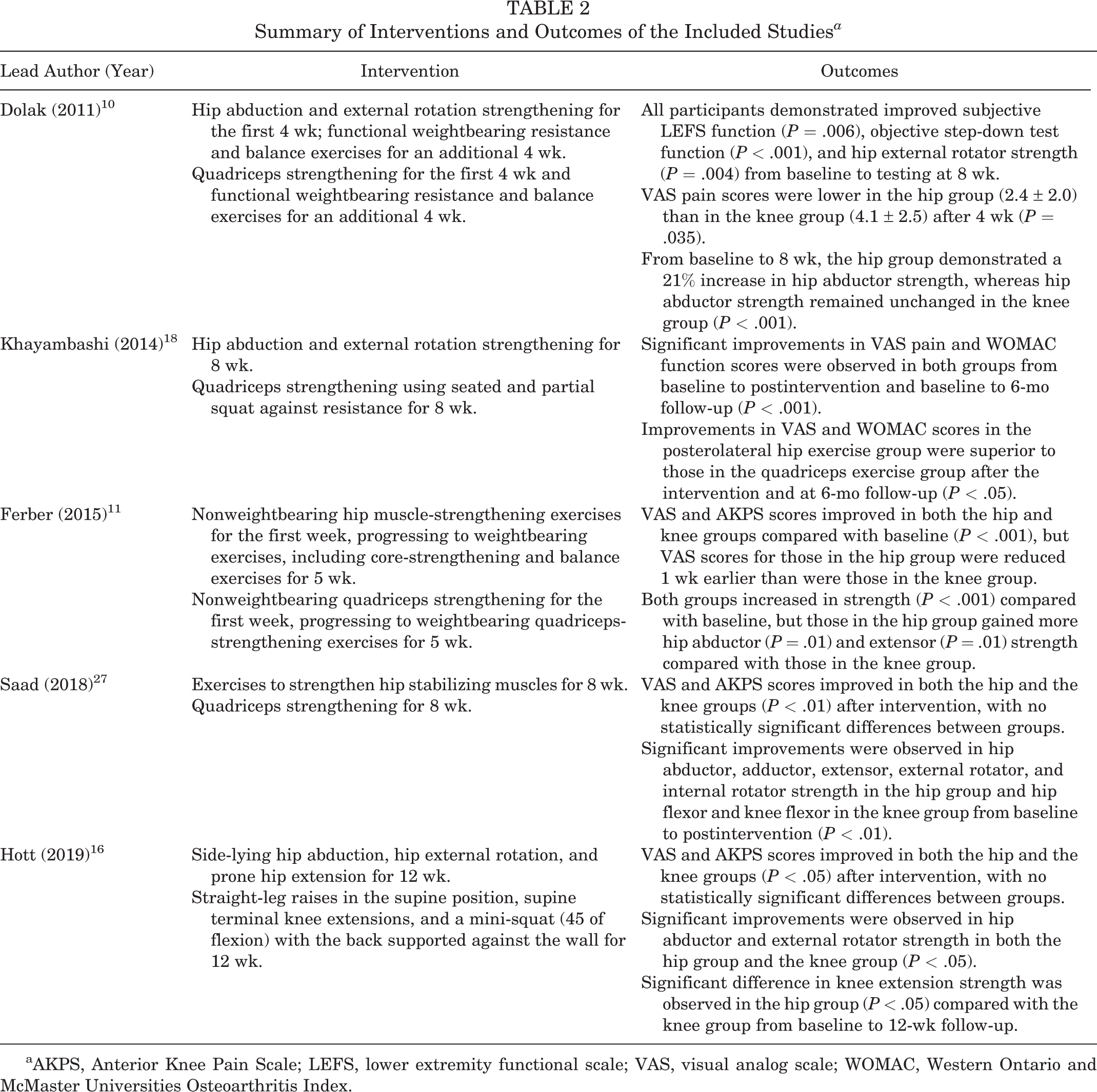
aAKPS, Anterior Knee Pain Scale; LEFS, lower extremity functional scale; VAS, visual analog scale; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Methodological Quality
The methodological quality of the included studies was assessed using the PEDro scale (Table 3). All of the studies received a score of at least 6, which indicated that the included studies were of moderate to high quality and reflected good internal and external validity.
Quality Assessment of the Included Studies a

a Key to item numbers: 1 = eligibility criteria specified; 2 = random allocation of patients; 3 = concealed allocation of patients; 4 = groups similar at baseline; 5 = patient blinding; 6 = therapist blinding; 7 = assessor blinding; 8 = outcome measures obtained from >85% of patients; 9 = treatment received or gave intention to treat; 10 = between-group statistical comparison; 11 = within-group statistical comparison. LoE, level of evidence; N, no; Y, yes.
VAS Pain Scores
All included studies assessed pain using the VAS scale. In all of the studies, significant improvements in VAS score were observed for both hip-strengthening exercise and knee-based exercise groups from baseline to postintervention (P < .05). One study reported lower VAS pain score in the hip group (2.4 ± 2.0) than the knee group (4.1 ± 2.5) after 4 weeks of exercise (P = .035). 10 One study found that the hip group had a significant reduction in self-reported pain starting at week 3 of exercise, which was 1 week earlier than was self-reported pain reduction in the knee group. 11 One study observed that improvement in VAS pain score in the hip group was superior to that in the knee group after the intervention and at 6-month follow-up (P < .05). 18 All included studies were analyzed with regard to VAS pain score; however, a statistically significant improvement in VAS score was not reported in favor of the hip group over the knee group (MD, –0.04 [95% CI, –0.41 to 0.33]; P = .83). Heterogeneity for the VAS score in the included studies was low (I2 = 12%) (Figure 2).
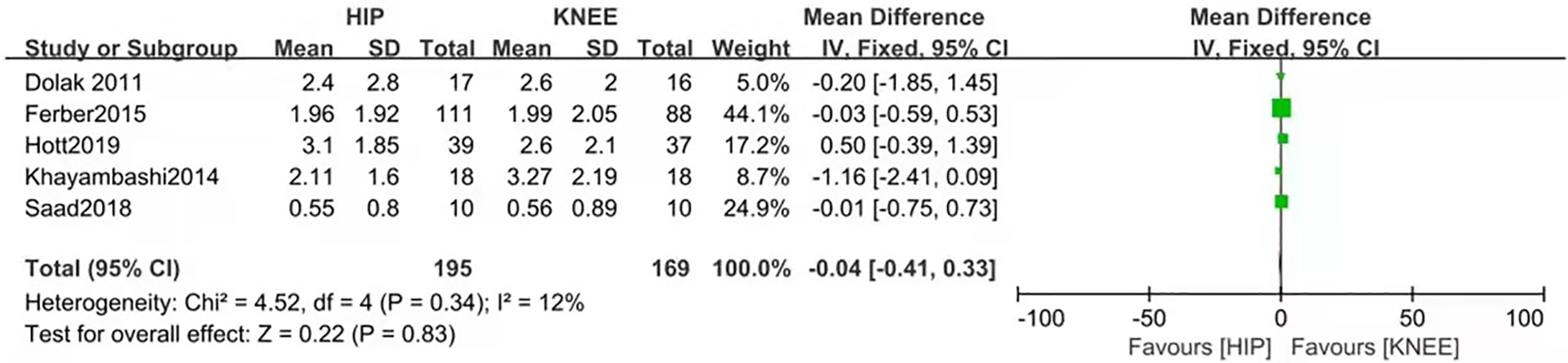
Hip-strengthening exercises compared with knee-based exercises for visual analog scale pain score. IV, inverse variance.
Subjective and Objective Functional Tests
The self-reported Lower Extremity Functional Scale (LEFS), which is a reliable way to assess function, significantly improved from baseline to 4 weeks or 8 weeks (P < .05), regardless of the protocol. 10 The objective step-down test, which was established to assess functional strength in the PFPS population, also significantly improved over the course of rehabilitation, regardless of the group. 10 One study observed that improvement in self-reported Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) was superior in the hip group compared with the knee group after the intervention and at 6-month follow-up (P < .05). 18 A total of 3 studies analyzed self-reported AKPS function score and did not demonstrate statistically significant improvements in favor of the hip group over the knee group (MD, 0.32 [95% CI, –2.06 to 2.70]; P = .79). 11,16,27 Heterogeneity for the AKPS function score in the included studies was low (I2 = 0%) (Figure 3).

Hip-strengthening exercises compared with knee-based exercises for function score on the Anterior Knee Pain Scale. IV, inverse variance.
Hip and Knee Muscle Strength
Dolak et al 10 measured strength of the hip abductor, hip external rotator, and knee extensor using a handheld dynamometer and found that the hip group demonstrated a 21% increase (P < .001) in hip abductor strength whereas hip strength remained unchanged in the knee group from baseline to 8 weeks. Ferber et al 11 used a force dynamometer to measure hip abductor, hip external rotator, hip internal rotator, hip extensor, and knee extensor strength output of the maximal voluntary isometric contraction force and observed that patients in the hip group gained more in hip abductor strength (P = .01) and extensor strength (P = .01) compared with the knee group. Saad et al 27 used a load cell (Kratos) adapted to a digital reader to measure hip abductor, adductor, extensor, flexor, external rotator, and internal rotator strength as well as knee extensor and flexor strength; the investigators found significant improvements in hip abductor, adductor, extensor, external rotator, and internal rotator strength in the hip group and significant improvements in hip flexor and knee flexor strength in the knee group from baseline to postintervention (P < .01). Hott et al 16 measured strength using a force sensor (300 kg; MuscleLab 6000 ML; Ergotest Innovation), which is considered a superior measurement device, and found a significant difference in knee extension strength in the hip group (P < .05) compared with the knee group from baseline to 12-week follow-up. We did not attempt to quantify the amount of hip and quadriceps strength improvement because of the heterogeneity of measuring methods and instruments.
Discussion
The main finding of this systematic review was that muscle strengthening for the hip and the knee joints was effective in decreasing pain and improving function, although no statistically significant difference between groups was observed using pooled analysis. The VAS score was reduced earlier for patients in the hip group than for patients in the knee group in 2 studies. 10,11 Khayambashi et al 18 found that improvement in WOMAC score in the hip group was statistically superior to that in the knee group after the intervention and at 6-month follow-up. In 2 studies, patients in the hip group exhibited statistically greater gains in hip abductor and extensor strength than did patients in the knee group after the intervention. 10,11
The included studies showed good internal and external validity according to the overall PEDro scale, as they satisfied most of the items. Two studies did not describe the method of allocation concealment and thus did not satisfy item 3 on the PEDro scale. 11,18 Blinding of patients and physical therapists was difficult in the included studies because the purpose was to investigate the effect of physical therapy. Therefore, none of the included studies satisfied items 5 and 6.
Crossley et al 9 reported that VAS and AKPS (ie, the Kujala score) are the most reliable outcome assessments for patients with PFPS. The VAS pain score was evaluated by all of the studies included in this review. Significant reductions in VAS pain score were observed in both groups from baseline to postintervention. To compare which physical therapy was more effective for pain relief, we performed a pooled analysis for the VAS score and found that neither group was superior to the other. Of the 5 studies included, 3 studies used the AKPS function score, 11,16,27 1 study used the subjective LEFS function score, 10 and 1 study used the WOMAC function score. 18 There appeared to be more improvements in pain and function scores using hip intervention than using knee intervention, although no statistically significant difference was found after pooled analysis. For example, Khayambashi et al 18 demonstrated that improvements in pain and function scores in the hip group were statistically superior to those in the knee group after the intervention and at 6-month follow-up.
Biomechanical research on PFPS has demonstrated that potential contributors include excessive hip internal rotation and hip adduction as well as weak muscle performance of the hip abductors, external rotators, and hip extensors in participants who report pain compared with pain-free individuals. 23,31 In the study by Dolak et al, 10 female patients with PFPS performed hip strengthening (hip abduction and external rotation strengthening) or quadriceps strengthening for the first 4 weeks before the addition of functional weightbearing resistance and balance exercises for the next 4 weeks; the investigators found that the hip group demonstrated a 21% increase (P < .001) in hip abductor strength whereas hip abductor strength remained unchanged in the knee group from baseline to 8 weeks. Participants in the study by Ferber et al 11 performed nonweightbearing hip (hip abduction and external rotation strengthening) or knee muscle-strengthening exercises for the first week and progressed to weightbearing hip (hip abduction, internal rotation, external rotation, and balance exercises) or knee muscle-strengthening exercises for an additional 5 weeks. The investigators demonstrated that hip exercises exhibited statistically greater improvements in hip abductor and extensor strength than did the baseline condition or knee exercises. Both of these studies reported rehabilitation protocols that entailed a combination of nonweightbearing and weightbearing exercises and showed efficiency in increasing hip abductor and extensor strength, the lack of which both have been confirmed as potential contributors to PFPS. A weightbearing position requires a contribution of both hip and quadriceps musculature, which may contribute to the positive findings. Scali et al 29 showed that a multijoint-strengthening program (involving hip and knee joints) for reducing pain and improving functional performance was superior to a traditional knee-strengthening program.
Harvie et al 14 suggested that effective strengthening for patients with PFPS entailed performing 2 to 4 sets of 10 or more repetitions daily for 6 or more weeks. Scali et al 29 reported that duration and dosage of exercise were major factors in improving pain, function, and muscle strength. All of the studies included in the review by Scali et al involved an exercise duration of >6 weeks and obtained significant improvements from baseline to final follow-up. Ferber et al 11 designed a 6-week hip- and knee-strengthening protocol in which participants performed 3 sets of 10 or more repetitions per week; the investigators observed significant improvements in VAS score, AKPS score, and hip abductor-extensor strength in both groups from baseline to postintervention. The rest of our included studies used protocols with a slightly increased number of repetitions and exercise progression.
This review had some limitations. The method of diagnosing PFPS varied among the included studies, being based on symptom location and reproduction of pain with activities or assessment via radiography and magnetic resonance imaging; this inconsistency might bring about confusion. There were differences in rehabilitation protocols, including intervention programs (such as different positions [side-lying, sitting, and standing] and different testing procedures), rehabilitation duration, and exercise dosage.Heterogeneity of sexes among the included studies is an important variable in this analysis because female patients have a higher prevalence of PFPS than do their male counterparts. Despite these limitations, this review is a synthesis of the available high-quality studies on PFPS and provides useful information to researchers.
Conclusion
The best-available evidence suggests that overall, isolated hip and knee strengthening were equivalent for PFPS. In some of the included studies, isolated hip muscle strengthening was more effective in increasing hip abductor and extensor strength and reducing pain earlier compared with knee-based strengthening.
Footnotes
Final revision submitted December 22, 2020; accepted February 9, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: This research was supported by the Natural Science Foundation of Inner Mongolia (No. 2016MS0366, 2020MS08119). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.