
Abstract
Background:
Throwing-related shoulder and elbow pain continues to be reported among adolescent baseball players. Few prospective studies have specifically examined the association between throwing-related shoulder and elbow pain and physical and developmental changes.
Purpose:
To evaluate the changes in physical and developmental characteristics during 1 year with respect to throwing-related shoulder and elbow pain in adolescent baseball players.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
This 1-year prospective follow-up study investigated 164 baseball players aged 7 to 13 years. Player data (age, height, weight, field position, and pitch count), lower extremity muscle tightness, and range of motion (ROM) of the shoulder, elbow, and hip joints were assessed during the 2016 and 2017 preseason medical examinations. After the 2016 season, the participants completed questionnaires related to throwing-related shoulder and elbow pain, defined as an inability to play for ≥1 week because of elbow or shoulder difficulties. For study participants with and without throwing-related shoulder or elbow pain during the 2016 season, we conducted univariate and multivariate logistic regression analysis to identify risk factors for throwing-related shoulder or elbow pain.
Results:
Overall, 21 players (12.8%) reported a shoulder pain episode, 56 players (34.1%) had an elbow pain episode, and 70 players (42.7%) reported having experienced shoulder and/or elbow pain during the 2016 season. In multivariate logistic regression analysis, (1) shoulder pain was associated with 2016 preseason height (odds ratio [OR], 1.06; 95% CI, 1.01-1.11; P = .01) and change in dominant-side elbow extension ROM from 2016 to 2017 (OR, 1.12; 95% CI, 1.02-1.24; P = .02); (2) elbow pain was associated with change in weight from 2016 to 2017 (OR, 1.21; 95% CI, 1.04-1.41; P = .014); and (3) throwing-related shoulder and/or elbow pain was associated with greater 2016 preseason height (OR, 1.04; 95% CI, 1.003-1.68; P = .03) and an increase in height from 2016 to 2017 (OR, 1.17; 95% CI, 1.01-1.35; P = .03).
Conclusion:
Our results indicated that adolescent baseball players who were taller in the preseason and those with an increase in height over the 1-year study period faced significant risks for developing throwing-related shoulder and/or elbow pain.
Throwing-related shoulder and elbow pain continue to occur among adolescent and skeletally immature baseball players. 3,8,9,14,16 –19,22,29 –33 A study by Bone and Joint Decade Japan, the Committee for the Prevention and Education of Sports Injuries During the Growth Period, and the Japanese Orthopaedic Association included a nationwide survey of elementary school baseball players to assess practice conditions and prevalence of shoulder and elbow pain. 30 Results indicated that among 7894 adolescent baseball players with no shoulder or elbow pain, 17.4% had newly experienced shoulder or elbow pain after 1 year.
Various factors have been reported as influencing throwing-related shoulder and elbow pain. † Previous prospective studies in adolescent baseball players have shown that risk factors for elbow pain were older age, increased weight, decreased height, weight lifting during the season, baseball playing outside the league, being a pitcher or catcher, decreased satisfaction with playing ability, arm fatigue during the game pitched, increased pitches during the season, and longer training hours per week. 9,17 Furthermore, an earlier cross-sectional study of 122 adolescent baseball players demonstrated that limitations to hip flexion and internal rotation (IR) at 90° of hip flexion were risk factors for elbow injury. 22
One musculoskeletal characteristic of immature athletes is growth. 7 An increase in height engenders increased bone length but not the concomitant growth of soft tissues around the bone. Muscle-tendon imbalances around the shoulder and elbow joint attributable to bone growth can occur in adolescent baseball players. Assessing the association between developmental factors and throwing-related shoulder and elbow pain in adolescent baseball players is particularly important. Producing training programs suitable for individuals’ growth may prevent difficulties among adolescent baseball players.
The aim of this prospective study was to evaluate the changes in physical and developmental characteristics during 1 year with respect to throwing-related shoulder and elbow pain in adolescent baseball players. We hypothesized that taller or heavier players and those with rapid growth and hip range of motion (ROM) loss will be at increased risk for shoulder and elbow pain.
Methods
This prospective study examined 164 male baseball players who were members of regional youth baseball teams during the 2016 season. All players participated in preseason medical examinations held in February 2016 and February 2017. We assessed the association between shoulder and/or elbow pain in the 2016 season and the amount of change in physical and ROM characteristics during 1 year (February 2016 to February 2017).
The inclusion criteria of the study were preseason participation, but there were no restrictions on throwing activity. Players were excluded from the study if they had prior injury or surgery to the pitching arm. We defined “shoulder and elbow symptoms” as any condition caused directly by throwing that resulted in a loss of participation for at least 1 week of baseball. All participants and their parents gave informed consent to participation in this study, which was approved by an institutional review board.
Participant Characteristics
Player height and weight were measured during the 2016 and 2017 preseason medical examinations. Height was measured using a digital height meter (A&D Corp). A multifrequency segmental body composition analyzer (MC780U; Tanita Corp) was used to measure body weight. After the 2016 season, participants completed a self-administered questionnaire including items related to age, position, hand dominance, years of playing baseball, hours of practice per day, number of days practiced per week, and present and prior experiences of shoulder or elbow pain.
Preseason Medical Examinations
The 2016 and 2017 physical examinations were performed by 2 orthopedic surgeons (H.S. and T.I.) with >15 years of experience. Participants were guided not to pitch within at the least 24 hours before the examination. 13 All ROM testing was measured and recorded as a single value after each joint ROM was moved through its full range a few times to provide opportunity for the joint structure to loosen and relax. Physical examinations were conducted with respect to ROM of the shoulder, elbow, and hip on both the dominant and nondominant sides. For each player, we calculated the difference between the nondominant and dominant sides in elbow ROM (extension and flexion) as well as the dominant/nondominant ratio for shoulder ROM, hip ROM, and straight-leg raise (SLR) angle. Figure 1 demonstrates our assessment techniques for each extremity.
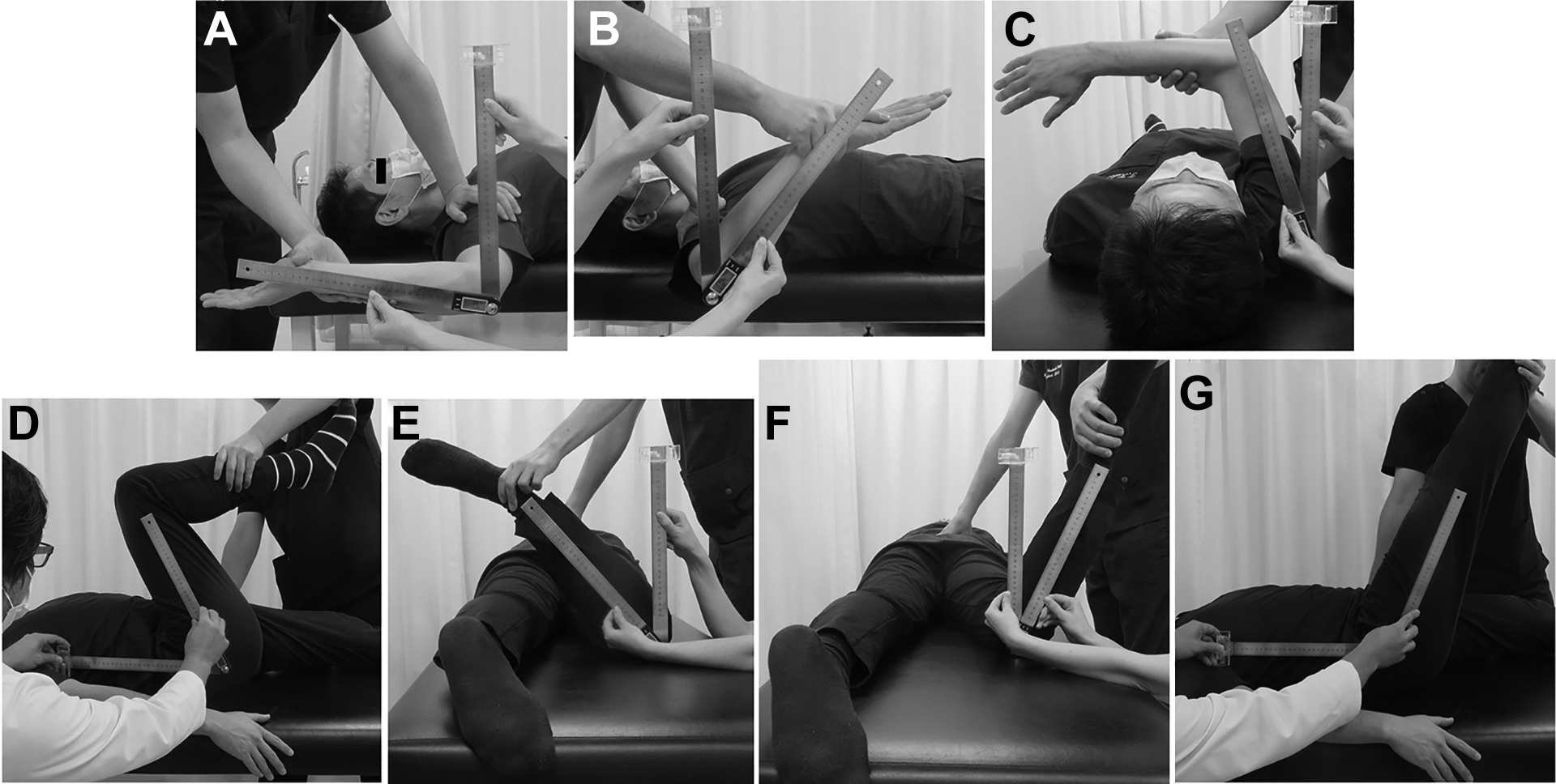
Assessment techniques for (A) shoulder external rotation, (B) shoulder internal rotation, (C) shoulder horizontal flexion, (D) hip flexion, (E) external rotation at 90° of hip flexion, (F) internal rotation at 90° of hip flexion, and (G) passive straight-leg raise angle.
Shoulder ROM
The participants lay supine on an examination table during measurement of passive shoulder ROM at 90° abducted external and internal rotation (ABER and ABIR, respectively). One examiner stabilized the scapula and moved the forearm to the end range, and the second examiner measured the ROM using a digital goniometer (iGaging) (Figure 1, A and B). This procedure has been used in earlier studies. 21,27,28
In a prior study, 31 we evaluated the intratester reliability of passive shoulder ABER and ABIR measurements in 10 healthy men who were measured and remeasured 5 days later by the same examiner; the intraclass correlation coefficient (ICC) was found to be 0.84 for shoulder ABER and 0.88 for shoulder ABIR.
Shoulder Horizontal Flexion
In the follow-through phase of a pitch, horizontal flexion is necessary to minimize stress on the posterior shoulder soft tissue. The horizontal flexion (HF) test was employed to evaluate posterior shoulder tightness. Players were positioned supine on an examination table with the humerus abducted to 90° and elbow flexed to 90°, and stabilization was achieved at the scapula behind the chest wall. The player was then instructed to move the arm passively into HF (Figure 1C).
Elbow ROM
Elbow ROM was measured with the participant in a seated position. The shoulder was elevated 90° with the elbow in full extension and flexion and the wrist in full supination. The fulcrum of the goniometer was positioned over the lateral epicondyle of the humerus, with 1 arm of the device along the length of the humerus to the tip of the acromion process and the other arm along the length of the radius to the radial styloid process. In our prior study, 31 10 healthy men were measured and remeasured for passive ROM of elbow extension and flexion within 5 days by the same examiner, and the ICC was found to be 0.97 for elbow extension and for 0.98 for elbow flexion.
Hip Flexion ROM
Players were positioned supine with both the hip and knee flexed to 90°. While 1 examiner stabilized the pelvis and contralateral thigh, the other rotated the hip internally and externally to its maximal point (H.S. and T.I.). The distal limb of the digital goniometer was aligned parallel to the midaxillary axis, 15 and maximal passive external rotation (ER) and IR were recorded for each hip (Figure 1, E and F). A pilot test was conducted to evaluate the intratester reliability of the hip ROM measurements in this study. Ten healthy men were measured and remeasured for passive hip flexion ROM within 5 days by the same examiner, and the ICC was found to be 0.96 for hip flexion, 0.86 for hip ER, and 0.98 for hip IR.
Passive SLR
The passive SLR test, used to evaluate changes in hamstring muscle flexibility, has demonstrated high interobserver reliability (ICC, 0.94-0.96). 10 Each test was performed with the individual supine, wearing shorts or underwear. The following bony landmarks were identified and labeled with a marker: the anterior superior iliac spine; the greater trochanter and lateral epicondyle of the femur; and the head of the fibula and the fibular malleolus. One examiner (T.I.) performed the passive SLR test by keeping the knee in full extension and the ankle in neutral plantarflexion/dorsiflexion (Figure 1G). Full ankle dorsiflexion was avoided to prevent calf muscle stiffness or pain (gastrocnemius and soleus) from confounding the sensation of hamstring stiffness and pain. The SLR angle was recorded once using a digital goniometer.
Statistical Analysis
After data collection was completed, participants were stratified according to those with shoulder or elbow pain and those without. First, comparative evaluations of the 2016 preseason data between the 2 groups were made using univariate analysis and multivariate logistic regression analysis to investigate the risk factors related to shoulder and elbow pain during the 2016 season. Second, we calculated the amount of change of the evaluated items (height; weight; ROM of shoulder, elbow, and hip; and SLR angle) between the February 2016 and February 2017 examinations, and the data between the 2 groups were compared using univariate analysis and multivariate logistic regression analysis to elucidate risk factors for shoulder and elbow pain in the 2016 season. The data are shown as odds ratios (ORs) and 95% CIs.
Multivariate logistic regression analysis was used to identify variables independently related to players with shoulder pain, with elbow pain, and with shoulder and/or elbow pain. Variables considered for the model were selected based on results of univariate analyses (P < .1). 19 For all analyses, results with P values <.05 were considered statistically significant.
Results
The mean age of the 164 baseball players was 10.5 ± 1.4 years (range, 7-13 years). There were 23 pitchers, 15 catchers, and 126 fielders.
Shoulder Pain
Of the players, 21 (12.8%) had experienced episodes of shoulder pain during throwing in the 2016 season. In the univariate analysis of shoulder pain in the 2016 season and preseason variables, shoulder pain was associated with height (without pain: 140.9 ± 10.1 cm; with pain: 147.9 ± 11.0 cm; OR, 1.06; 95% CI, 1.02-1.11; P = .007) and shoulder ABER ratio (OR, 283.0; 95% CI, 1.18-677,796.5; P = .04) (Appendix Table A1). Multivariate logistic regression analysis was conducted with the following explanatory variables: height; shoulder ABER ratio; and difference between the nondominant and dominant sides for elbow flexion ROM. It revealed a significant association between shoulder pain in the 2016 season and preseason height (OR, 1.06; 95% CI, 1.01-1.11; P = .01).
In the univariate analysis of changes from 2016 to 2017, shoulder pain during the 2016 season was associated with Δdominant elbow extension (OR, 1.13; 95% CI, 1.03-1.24; P = .009) and Δnondominant hip ER (OR, 1.04; 95% CI, 1.01-1.08; P = .02) (Appendix Table A2). The multivariate logistic regression analysis for predictors of shoulder pain used Δheight, Δdominant elbow extension, Δdominant hip ER, and Δnondominant hip IR as explanatory variables. Results indicated a significant association between shoulder pain in the 2016 season and 1-year Δdominant elbow extension ROM (OR, 1.12; 95% CI, 1.02-1.24; P = .02).
Elbow Pain
Of the participants, 56 (34.1%) had experienced episodes of elbow pain during throwing in the 2016 season. Univariate analysis demonstrated no relation between elbow pain in the 2016 season and preseason variables (Appendix Table A3).
Regarding 1-year changes, univariate analysis results showed that elbow pain in the 2016 season was associated with Δheight (OR, 1.20; 95% CI, 1.03-1.38; P = .015) and Δweight (OR, 1.30; 95% CI, 1.10-1.43; P < .001) (Appendix Table A4). Multivariate logistic regression analysis using Δheight, Δweight, Δdominant hip IR, and Δnondominant SLR angle as explanatory variables indicated a significant association between elbow pain in the 2016 season and Δweight (OR, 1.21; 95% CI, 1.04-1.41; P = .014).
Shoulder and/or Elbow Pain
Of the players, 70 (42.7%) had experienced episodes of shoulder and/or elbow pain during throwing in the 2016 season. In the univariate analysis related with shoulder pain and/or elbow pain in the 2016 season and variables in the 2016 preseason, height (OR, 1.04; 95% CI, 1.01-1.07; P = .01) and being a pitcher (OR, 2.95; 95% CI, 1.16-7.47; P = .02) were significantly associated with throwing-related shoulder and/or elbow pain (Appendix Table A5). Multivariate logistic regression analysis indicated that greater height at preseason (OR, 1.04; 95% CI, 1.003-1.68; P = .03) was significantly associated with throwing-related shoulder and/or elbow pain.
In the univariate analysis of 1-year changes, an increase in height (OR, 1.17; 95% CI, 1.01-1.35; P = .02) and a decrease in elbow extension ROM (OR, 1.08; 95% CI, 1.01-1.15; P = .03) were significantly associated with throwing-related shoulder and/or elbow pain (Appendix Table A6), and multivariate logistic regression analysis showed that an increase in height (OR, 1.17; 95% CI, 1.01-1.35; P = .03) was significantly associated with throwing-related shoulder and/or elbow pain during the 2016 season.
Discussion
Our results showed that shoulder pain during the 2016 season was associated with greater preseason height (OR, 1.06; 95% CI, 1.01-1.11; P = .01). Our data also demonstrated that throwing shoulder and/or elbow pain was associated with greater preseason height (OR, 1.04; 95% CI, 1.003-1.68; P = .03) and an increase in height from 2016 to 2017 (OR, 1.17; 95% CI, 1.01-1.35; P = .03).
Few studies have investigated risk factors for shoulder and elbow pain in adolescent baseball players. Lyman et al 17 conducted a longitudinal study and demonstrated that shoulder pain was associated with increased game pitches, decreased cumulative pitch count, arm fatigue, and decreased self-perceived performance in 298 young baseball pitchers. Matsuura et al 18 conducted a 1-year prospective study that found history of shoulder or elbow pain, playing pitcher, playing catcher, and increasing training as factors affecting shoulder pain in 900 young baseball pitchers. However, that study found no association between height and shoulder pain occurrence. We believe that taller baseball players are likely to have longer arms, which are likely to weigh more than shorter arms, with motion maintained by shoulder joints during pitching. Taller baseball players exert more torque through the arm in throwing motion and increased pitching velocity as a sequel to a longer lever arm. 1,4 Our findings implicate height as a physical characteristic related to shoulder and elbow health conditions in young baseball players.
Earlier studies demonstrated a relation between developmental factors and throwing-related shoulder or elbow pain in youth baseball pitchers. 8,33 Yukutake et al 33 retrospectively investigated risk factors for elbow pain during the prior year for 392 Little League baseball players aged 6 to 12 years, with emphasis on developmental factors. They reported greater height (OR, 1.10; 95% CI, 1.03-1.17) and increased height of >6.3 cm per year (OR, 1.16; 95% CI, 1.00-1.34) as risk factors related to throwing elbow pain after adjustment for demographic, developmental, and other baseball-related factors. Greenberg et al 8 examined the association between physical characteristics related to growth and shoulder performance, baseball exposure, and throwing-related shoulder and elbow pain in 84 young baseball players in a case-control study. Their results revealed player height as the most predictive of throwing-related arm pain, with a 1-inch (2.54-cm) increase in height resulting in a 77% increased risk of pain (OR, 1.77; 95% CI, 1.17-2.66). In our study, the mean amount of increased height of the participants with throwing-related shoulder or elbow pain was 6.4 cm per year, which is similar to data reported by Yukutake et al. Gill and Micheli 7 reported that bone growth engenders muscle-tendon imbalance around the shoulder and elbow joints, caused by increased muscle tension with the decreased flexibility in skeletally immature athletes. These findings between musculoskeletal growth and shoulder and elbow pain in baseball players are important in order to educate parents and coaches. This awareness may prevent throwing-related pain.
In our study, shoulder pain during the 2016 season was associated with the 1-year change in dominant-side elbow extension ROM (OR, 1.12; 95% CI, 1.02-1.24; P = .02). An improvement in dominant-side elbow extension appeared to have a protective effect on the rest of the shoulder, resulting in better condition of the elbow joint in young baseball players. We also noted that in univariate analysis, the 1-year change in hip ER of the nondominant side was significantly larger in players with versus without shoulder pain (OR, 1.04; 95% CI, 1.01-1.08; P = .02)
Excess hip ER of the lead leg (nondominant side) during arm acceleration through ball release may cause early pelvic rotation, attenuating force production and transfer, as well as decreasing the ability of the lower extremities to absorb the forces in the kinematic chain of throwing motion. The inability of the lower extremities to absorb force will cause the rotator cuff to contract eccentrically to absorb those forces in order to decelerate the arm, which may cause stress at the glenohumeral joint. 2,5,25,26 Contrary to our hypothesis, this result implies that excess hip ER on the lead leg may be related to throwing shoulder pain in adolescent baseball players. Further research is needed to elucidate the relationship between throwing-related pain and anthropometric conditions of the nondominant side in adolescent baseball players.
Another distinguishing characteristic of our results is that elbow pain in the 2016 season was associated with increased weight. Lyman et al 17 demonstrated increased weight as a risk factor for elbow pain among skeletally immature baseball players. Heavier baseball players are likely to have heavier arms, resulting in more weight being maintained by the elbow joint during pitching motion. 17 This might generate a greater moment of inertia, resulting in higher torque on the elbow joint. None of the preseason variables for 2016 were associated with elbow pain (Appendix Table A3); however, in univariate analysis, the changes in height and weight during 1 year were related to elbow pain (Appendix Table A4). This suggests that rapid growth during a season is an important risk factor for elbow pain.
In the univariate analysis, we found that the hip flexion ratio (dominant/nondominant side) of the 2016 preseason tended to be related with elbow pain in the 2016 season, but the tendency was not significant. Saito et al 22 demonstrated the hip flexion ROM of the bilateral side in the elbow pain group to be significantly smaller than those in the no elbow pain group in 122 adolescent baseball players. Throwing motions are accomplished through activation of a kinetic chain involving individual body parts such as the leg, pelvis, trunk, and arm—all coordinated in their movements by muscle activity and body positions to generate, combine, and transfer force through the body into the arm. 12,13 In the pitching motion, proper plant-leg positioning when the foot is planted (a closed-shoulder position) allows for integral rotation of the hips, pelvis, and trunk, thereby providing increased speed and power in both hips after flexion through the kinetic chain. 5,6 Achieving this position during the cocking phase of the throwing motion requires sufficient hip ROM to allow IR of the trailing leg. Restrictions of hip ROM inhibit proper trunk rotation. 34 As hypothesized, hip flexion loss was associated with elbow pain, although this was not significant. This finding may be used to encourage coaches to check the hip flexion ROM of players to prevent elbow pain. Additional studies should be conducted to elucidate the association between the throwing-related pain and the conditioning of the core musculature and lower extremities in adolescent baseball players.
In this study, 1-year elbow extension ROM deficits in the participants with throwing-related pain were significantly larger than those in participants without throwing-related pain. Sakata et al 23 performed a prospective investigation of physical risk factors for a medial elbow injury within junior baseball players (aged 6-12 years). In their results, a side-to-side elbow extension deficit of ≥5° was significantly associated with medial elbow injury. These findings suggest that early identification of elbow extension deficits may prevent throwing-related pain and injury. It may be important for coaches and parents to check for early signs of throwing-related injury in order to intervene before the onset of pain.
Our study presents several limitations. First, we defined “shoulder and elbow symptoms” as a condition caused directly by throwing that caused participation loss for at least 1 week during 1 year. However, we could not objectively confirm the exact pathology of throwing-related pain and evaluate the duration and severity of shoulder and elbow pain. Second, the cumulative pitch count and hours of training and position, which have been reported as risk factors for shoulder and elbow pain in earlier studies, were not associated with the throwing-related pain. 3,8,9,14,16 –19 These data were influenced by each participant’s recall bias. Third, we did not analyze several risk factors of elbow injury that have been described in earlier reports of the relevant literature, including pitching mechanics, pitches per game or day, innings pitched per season, games per year, pitch type, and pitch velocity. Fourth, we could not evaluate the effect of shoulder pain on the elbow joint in pitching from the viewpoint of the kinetic chain. The scapula, which makes up the shoulder joint, is key in facilitating this energy transfer distally to the hand. 12 Scapular dysfunction that may cause the shoulder pain prohibits optimal energy transfer and may influence the elbow joint condition during the throwing motion. 12,20 Future research is needed to further identify the association of shoulder pain and elbow pain with failure of any links in the kinetic chain in young baseball players.
Conclusion
Our results indicate that adolescent baseball players who are taller in the preseason and those with an increase in height over 1 year face significant risks for developing throwing-related shoulder or elbow pain. Our findings suggest that a preseason or in-season medical checkup of hip and elbow ROM may be an important strategy to prevent and discover earlier throwing-related shoulder and elbow pain and injuries for adolescent baseball players. We recommend that coaches and parents monitor closely the throwing-related pain in taller and heavier baseball players and that they check the height and weight development, reduce throwing volumes, and devote due attention to the establishment of training programs for players with rapid growth to prevent throwing-related injuries.
Footnotes
Authors
Tsuyoshi Tajika, MD, PhD (Gunma University Graduate School of Medicine Department of Orthopaedic Surgery, Maebashi, Gunma, Japan); Noboru Oya, MD, PhD (Gunma University Graduate School of Medicine Department of Orthopaedic Surgery, Maebashi, Gunma, Japan); Takuro Kuboi, MD (Gunma University Graduate School of Medicine Department of Orthopaedic Surgery, Maebashi, Gunma, Japan); Fumitaka Endo, MD (Gunma University Graduate School of Medicine Department of Orthopaedic Surgery, Maebashi, Gunma, Japan); Tsuyoshi Ichinose, MD, PhD (Gunma University Graduate School of Medicine Department of Orthopaedic Surgery, Maebashi, Gunma, Japan); Daisuke Shimoyama, MD (Gunma University Graduate School of Medicine Department of Orthopaedic Surgery, Maebashi, Gunma, Japan); Tsuyoshi Sasaki, MD, PhD (Gunma University Graduate School of Medicine Department of Orthopaedic Surgery, Maebashi, Gunma, Japan); Noritaka Hamano, MD, PhD (Gunma University Graduate School of Medicine Department of Orthopaedic Surgery, Maebashi, Gunma, Japan); Takuya Omodaka, MD, PhD (Gunma University Graduate School of Medicine Department of Orthopaedic Surgery, Maebashi, Gunma, Japan); Hiroki Kobayashi, MD (Gunma University Graduate School of Medicine Department of Orthopaedic Surgery, Maebashi, Gunma, Japan); Tokue Mieda, MD, PhD (Gunma University Graduate School of Medicine Department of Orthopaedic Surgery, Maebashi, Gunma, Japan); Koichi Okamura, MD, PhD (Gunma University Graduate School of Medicine Department of Orthopaedic Surgery, Maebashi, Gunma, Japan); Hitoshi Shitara, MD, PhD (Gunma University Graduate School of Medicine Department of Orthopaedic Surgery, Maebashi, Gunma, Japan); Yoichi Iizuka, MD, PhD (Gunma University Graduate School of Medicine Department of Orthopaedic Surgery, Maebashi, Gunma, Japan); Atsushi Yamamoto, MD, PhD (Gunma Sports Orthopaedics, Maebashi, Gunma, Japan); Ichiro Nakajima, MD (Saiseikai Maebashi Hospital Department of Orthopaedic Surgery, Maebashi, Gunma, Japan); Tsutomu Kobayashi, MD, PhD (Takasaki University of Health and Welfare Department of Physical Therapy, Takasaki, Gunma, Japan); Masaaki Sakamoto, RPT, PhD (Graduate School of Health Sciences, Gunma University, Maebashi, Gunma, Japan); Kenji Takagishi, MD, PhD (Sada Hospital Department of Orthopaedic Surgery, Fukuoka, Fukuoka, Japan); and Hirotaka Chikuda, MD, PhD (Gunma University Graduate School of Medicine Department of Orthopaedic Surgery, Maebashi, Gunma, Japan).
Acknowledgment
The authors thank the staff of the Department of Orthopaedic Surgery, Gunma University Graduate School of Medicine and Gunma Sports Rehabilitation Society, for their assistance with medical checkups and the young baseball players, their parents, coaches, and staff members of the regional baseball association, as well as medical staff members.
Final revision submitted December 18, 2020; accepted January 25, 2021.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Gunma University Graduate School of Medicine (ID No. 1003).
Notes
APPENDIX
Change in Variables for Shoulder and/or Elbow Pain From 2016 to 2017 a

| Amount of Change | Without Pain (n = 94) | With Pain (n = 70) | Odds Ratio (95% CI) b | P |
|---|---|---|---|---|
| Δheight, cm | 5.5 ± 2.2 | 6.4 ± 2.4 | 1.18 (1.01-1.36) |
|
| Δweight, kg | 3.8 ± 2.2 | 4.4 ± 3.2 | 1.10 (0.98-1.24) | .11 |
| Elbow extension, deg | ||||
| Δdominant | –0.46 ± 4.9 | –1.2 ± 4.2 | 1.08 (1.01-1.15) |
|
| Δnondominant | –1.1 ± 4.8 | –1.0 ± 4.5 | 0.99 (0.93-1.05) | .74 |
| Elbow flexion, deg | ||||
| Δdominant | 0.3 ± 6.0 | –0.5 ± 5.9 | 0.98 (0.93-1.03) | .40 |
| Δnondominant | –1.2 ± 5.2 | –1.9 ± 5.9 | 0.98 (0.92-1.03) | .39 |
| Shoulder ABER | ||||
| Δdominant | –1.5 ± 10.6 | –4.0 ± 12.3 | 0.98 (0.95-1.00) | .16 |
| Δnondominant | –2.7 ± 11.1 | –4.2 ± 11.0 | 0.99 (0.96-1.02) | .38 |
| Shoulder ABIR | ||||
| Δdominant | –0.7 ± 16.3 | –0.1 ± 13.8 | 1.002 (0.98-1.02) | .82 |
| Δnondominant | –3.6 ± 18.0 | –6.2 ± 14.6 | 0.99 (0.98-1.01) | .33 |
| Shoulder HF, deg | ||||
| Δdominant | –7.1 ± 14.7 | –11.0 ± 15.9 | 0.98 (0.96-1.00) | .11 |
| Δnondominant | –8.0 ± 21.4 | –12.2 ± 20.2 | 0.99 (0.98-1.01) | .21 |
| Hip flexion, deg | ||||
| Δdominant | –1.2 ± 14.0 | –1.2 ± 13.5 | 1.0001 (0.98-1.02) | .99 |
| Δnondominant | –1.0 ± 13.5 | –3.1 ± 8.1 | 0.98 (0.96-1.01) | .25 |
| Hip ER, deg | ||||
| Δdominant | –2.8 ± 13.3 | –1.2 ± 12.6 | 1.01 (0.99-1.03) | .41 |
| Δnondominant | –1.4 ± 13.3 | 0.3 ± 12.9 | 1.01 (0.99-1.03) | .41 |
| Hip IR, deg | ||||
| Δdominant | –0.3 ± 9.5 | –2.1 ± 8.0 | 0.98 (0.94-1.01) | .20 |
| Δnondominant | –3.2 ± 11.2 | –1.5 ± 9.8 | 1.02 (0.99-1.05) | .29 |
| SLR, deg | ||||
| Δdominant | –1.9 ± 9.9 | –2.6 ± 9.8 | 0.99 (0.96-1.02) | .64 |
| Δnondominant | –2.8 ± 9.9 | –4.6 ± 10.9 | 0.98 (0.95-1.01) | .26 |
a Data are reported as mean ± SD unless otherwise indicated. Bolded P values indicate statistical significance (P < .05). ABER, abducted external rotation; ABIR, abducted internal rotation; HF, horizontal flexion; ER, external rotation; IR, internal rotation; SLR, straight-leg raise.
b Odds ratios were calculated using univariate analysis. A 1-unit change in the explanatory variable increases the odds of having shoulder pain by a factor of the odds ratio.