
Abstract
Background:
Cheese-wiring, the suture that cuts through the meniscus, is a well-known issue in meniscal repair. So far, contributing factors are neither fully understood nor sufficiently studied.
Hypothesis/Purpose:
To investigate whether the construct stiffness of repair sutures and devices correlates with suture cut-through (cheese-wiring) during load-to-failure testing.
Study Design:
Controlled laboratory study.
Methods:
In 131 porcine menisci, longitudinal bucket-handle tears were repaired using either inside-out sutures (n = 66; No. 0 Ultrabraid, 2-0 Orthocord, 2-0 FiberWire, and 2-0 Ethibond) or all-inside devices (n = 65; FastFix360, Omnispan, and Meniscal Cinch). After cyclic loading, load-to-failure testing was performed. The mode of failure and construct stiffness were recorded. A receiver operating characteristic curve analysis was performed to define the optimal stiffness threshold for predicting meniscal repair failure by cheese-wiring. The 2-tailed t test and analysis of variance were used to test significance.
Results:
Loss of suture fixation was the most common mode of failure in all specimens (58%), except for the Omnispan, which failed most commonly because of anchor pull-through. The Omnispan demonstrated the highest construct stiffness (30.8 ± 3.5 N/mm), whereas the Meniscal Cinch (18.0 ± 8.8 N/mm) and Ethibond (19.4 ± 7.8 N/mm) demonstrated the lowest construct stiffness. The Omnispan showed significantly higher stiffness compared with the Meniscal Cinch (P < .001) and Ethibond (P = .02), whereas the stiffness of the Meniscal Cinch was significantly lower compared with that of the FiberWire (P = .01), Ultrabraid (P = .04), and FastFix360 (P = .03). While meniscal repair with a high construct stiffness more often failed by cheese-wiring, meniscal repair with a lower stiffness failed by loss of suture fixation, knot slippage, or anchor pull-through. Meniscal repair with a stiffness >26.5 N/mm had a 3.6 times higher risk of failure due to cheese-wiring during load-to-failure testing (95% CI, 1.4-8.2; P < .0001).
Conclusion:
Meniscal repair using inside-out sutures and all-inside devices with a higher construct stiffness (>26.5 N/mm) was more likely to fail through suture cut-through (cheese-wiring) than that with a lower stiffness (≤26.5 N/mm).
Clinical Relevance:
This is the first study investigating the impact of construct stiffness on meniscal repair failure by suture cut-through (cheese-wiring).
Menisci are essential for normal knee function, as they contribute significantly to tibiofemoral joint congruity, knee stabilization, shock absorption, proprioception, and joint lubrication. 16,20 Meniscal tears are a common cause of disability in young, physically active patients, 27 with a reported incidence of 61 in 100,000 per year. 24 Whenever possible, meniscal repair should be attempted for acute traumatic tears to prevent premature femorotibial osteoarthritis, which has been directly associated with meniscectomy. 19,26
Furthermore, supporting the clinical benefit of meniscal repair, recently published studies 25,35,41,43 have shown that meniscal repair resulted in better long-term patient-reported outcomes, higher activity levels, and less radiological degeneration compared with partial meniscectomy. Traditionally, inside-out suture repair has been considered the standard treatment for meniscal tears in the posterior horn and midportion, 14 although it is known that this method bears an increased risk for injuries to neurovascular structures and is associated with increased perioperative morbidity. 6,32 Hence, to overcome these complications, the first all-inside meniscal repair procedure was performed in 1991 by Morgan, 33 and this technique has rapidly developed since then. Likewise, several devices have been developed over the past years with the aim of improving surgical handling and the outcomes of meniscal repair. 1,5,13,17,18,22,32,37 Regardless of the chosen repair technique, several factors that determine successful outcomes after meniscal repair must be considered. For example, tear location, patient age, chronicity, size, and smoking habits have all been reported to influence the success rate of meniscal repair. 42
However, above all, the main requirement of meniscal repair is to provide secure and stable fixation of the torn meniscal margins, especially when considering the current trend of accelerated postoperative rehabilitation. 3,29 The biomechanical performance of the available devices has been broadly investigated, focusing mainly on pull-out strength and stiffness of meniscal repair. 11,12,44,45 In this context, construct stiffness represents stability of the fixation site, in particular, the ability of the repair to resist deformation. As previously described, high stiffness with relatively minimal displacement or gapping during the early rehabilitation period is considered essential for tissue healing. 9 However, the relationship between construct stiffness and the mode of failure under cyclic loading conditions has not yet been investigated.
The aims of this biomechanical study were to analyze the construct stiffness of meniscal repair for bucket-handle tears using different inside-out sutures and all-inside devices and to investigate whether construct stiffness was associated with cheese-wiring during load-to-failure testing. We hypothesized that different meniscal repair sutures and devices would show different values of construct stiffness, which, as a consequence, could be associated with different modes of failure.
Methods
Meniscal Preparation and Repair
A total of 131 fresh-frozen porcine menisci (63 lateral and 68 medial) were used for the present biomechanical analysis. All porcine samples were collected from a local slaughterhouse, and all animals had been slaughtered for meat production and not for study purposes. The porcine menisci used in this study would have been otherwise disposed; hence, no approval by the local Institutional Animal Care and Use Committee or institutional review board was necessary. After collection, the menisci were immediately frozen and then thawed for 5 hours at room temperature before testing. All menisci were isolated in matched pairs (medial and lateral) and were randomly assigned to different repair groups, and each meniscus was used for only 1 type of repair technique. A longitudinal tear was created with a No. 11 surgical blade approximately 3 mm from the peripheral capsular rim and then extended through the anterior and posterior horns to complete the bucket-handle tear. Vertical meniscal repair was performed in the center of the meniscus at the midpoint of the pars intermedia with a single passage of the suture through the meniscus, simulating a worst-case scenario.
The menisci were randomly assigned to 2 main groups; meniscal repair was conducted with inside-out sutures in 66 menisci using either the No. 0 Ultrabraid (Smith & Nephew; n = 26), 2-0 Orthocord (DePuy Synthes; n = 13), 2-0 FiberWire (Arthrex; n = 20), or 2-0 Ethibond (Ethicon; n = 7). In the second group, meniscal repair was performed with an all-inside device in 65 menisci using either the FastFix360 (Smith & Nephew; n = 31), Omnispan (DePuy Synthes; n = 14), or Meniscal Cinch (Arthrex; n = 20).
Experimental Setup
The biomechanical tests were conducted according to a previously validated and published protocol 38 using a servohydraulic universal testing machine (type LFV-5-PA ECD 120 hydropulse testing device; 5-kN static and 4-kN dynamic test load cells; Walter+Bai AG Testing Machines) and DionPro software (Version 4.43; Walter+Bai AG Testing Machines) at a sampling rate of 50 Hz. The menisci were fixed perpendicular to the testing machine using custom-made steel clamps (Figure 1). Testing was performed at room temperature, and the menisci were continuously moistened with 0.9% saline solution to simulate near physiological conditions and prevent changes in meniscal biomechanical properties.

Meniscal repair and fixation. (A) Femoral view: The meniscus repaired with Ultrabraid suture (arrow). (B) Fixation of the meniscus (red arrows) in custom-made steel clamps (white stars). Meniscal parts are kept together solely by the repair construct (black arrow). For further images, see Rosso et al. 37,38
Cyclic Loading and Load-to-Failure Testing
Cyclic loading was continuously performed in a sinusoidal load-controlled route between 5 and 20 N at a frequency of 2 Hz for 10,000 cycles. Displacement was recorded at a load of 5 N using a calibrated high-resolution digital camera (EOS DSLR D60; Canon) with an 18-megapixel Advanced Photo System type C complementary metal-oxide semiconductor sensor equipped with an EF 100mm f/2.8 L macro image stabilization ultrasonic motor lens (Canon). Displacement was measured by previously determined markers adjacent to the repair site using open-source software (ImageJ; National Institutes of Health) as previously published. 38
After 10,000 cycles, load-to-failure testing was conducted at a speed of 3.15 mm/s by applying forces exceeding 20 N until repair failure occurred. The mode of failure and construct stiffness were recorded.
Determination of Construct Stiffness
Construct stiffness was defined as the slope of the load-displacement curve, where the applied tensile load was plotted versus the measured displacement on the testing machine. A linear regression model was used to define the best-fit line for the linear portion of the curve. Because some of the specimens underwent stress relaxation before they reached ultimate failure, the linear region was determined from the initial area of the elastic range up to approximately 60% of each specimen’s failure force.
Definition of Construct Failure
Construct failure was defined as sudden loss of fixation (suture failure), knot slippage, suture cut-through (also known as cheese-wiring; tissue failure), and anchor pull-through. Knot slippage was not considered a mode of failure for the all-inside devices; likewise, anchor pull-through was not considered a mode of failure for the inside-out sutures.
Statistical Analysis
Descriptive statistics used the mean, standard deviation, and range to describe continuous data, whereas frequencies and percentages were used to present ordinary data. The 2-tailed t test was applied to identify a potential difference in stiffness of the inside-out sutures and all-inside devices. The 1-way analysis of variance, followed by the Bonferroni post hoc analysis, was used to investigate whether a significant difference in stiffness was present between meniscal repair techniques with a different mode of failure. A receiver operating characteristic (ROC) curve analysis was performed to define the optimal stiffness threshold for predicting meniscal repair failure by cheese-wiring. The Youden index 30 was utilized to determine the ideal threshold with the highest sensitivity and specificity. Based on the calculated threshold, a logistic regression analysis was applied to evaluate the relationship between construct stiffness and cheese-wiring. A post hoc power analysis was performed to estimate the statistical power (1 – β), with a large effect size (f = 0.4) and alpha of .05 using free statistical software (G*Power Version 3.1). All statistical analyses were performed using SPSS Version 21 (IBM). Statistical significance was set at P < .05.
Results
Load-to-Failure Testing
All specimens underwent load-to-failure testing after cyclic loading of 10,000 cycles (Table 1). Detailed results from load-to-failure testing and displacement after cyclic loading have been previously published. 37,38 Ultimately, 76 (58%) menisci demonstrated a loss of suture fixation, 5 (4%) demonstrated knot slippage, 29 (22%) demonstrated cheese-wiring (suture cut-through), and 21 (16%) demonstrated anchor pull-through (Figure 2). The overall mean stiffness of all menisci that underwent load-to-failure testing was 24.4 ± 8.1 N/mm.
Modes of Failure During Load-to-Failure Testing a

a Data are presented as numbers. Dashes indicate no failures for that category.
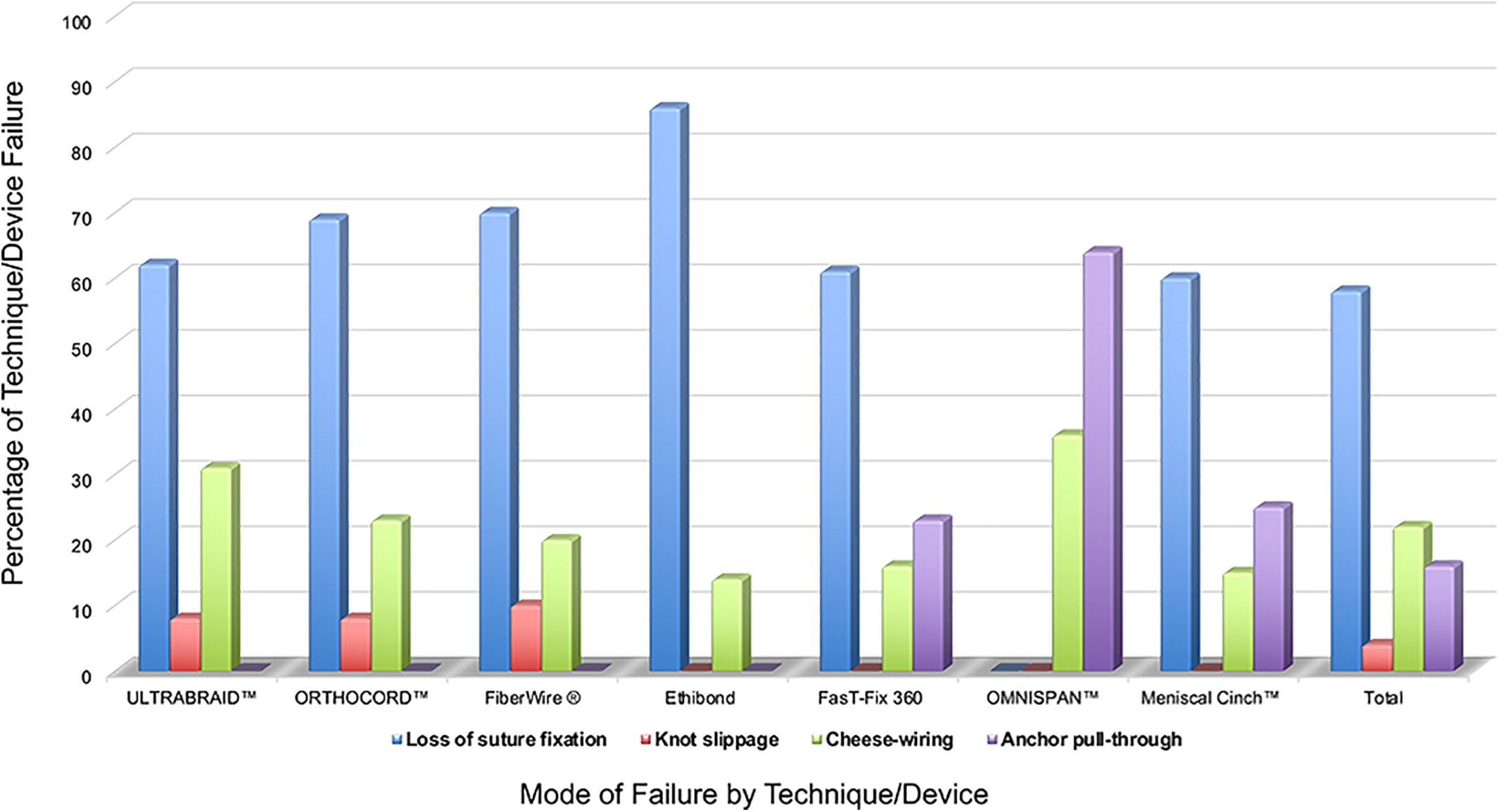
Summary of the mode of failure according to the meniscal repair suture/device. The data are illustrated as a percentage of the failure mode according to the suture/device.
A detailed analysis after load-to-failure testing revealed a construct stiffness with loss of suture fixation of 22.7 ± 7.0 N/mm, with knot slippage of 23.0 ± 3.7 N/mm, cheese-wiring of 29.2 ± 10.1 N/mm, and anchor pull-through of 24.5 ± 7.0 N/mm (Table 2).
Construct Stiffness According to the Mode of Failure

a Significantly different from suture cut-through (P < .01).
The mean stiffness of meniscal repair using inside-out sutures was 25.1 ± 10.2 N/mm for the Ultrabraid, 26.3 ± 3.1 N/mm for the Orthocord, 26.4 ± 7.3 N/mm for the FiberWire, and 19.4 ± 7.8 N/mm for the Ethibond, whereas the mean stiffness of meniscal repair using all-inside devices was 24.9 ± 4.8 N/mm for the FastFix360, 30.8 ± 3.5 N/mm for the Omnispan, and 18.0 ± 8.8 N/mm for the Meniscal Cinch (Table 3). The statistical power in detecting a difference in stiffness between sutures/devices for a total sample size of 131 menisci and 7 subgroups was 94%.
Construct Stiffness of Inside-Out Sutures and All-Inside Devices

a Significantly different from the Meniscal Cinch (P < .001) and Ethibond (P = .02).
b
Significantly different from the FiberWire (P = .01), Ultrabraid (P = .04), and FastFix
No significant difference in construct stiffness was observed between inside-out sutures and all-inside devices when categorized into 2 main groups (Table 3). The analysis of variance demonstrated a significant difference between the stiffness of meniscal repair performed with the Meniscal Cinch and Omnispan (mean difference, 12.8 N/mm; P < .001), Meniscal Cinch and FiberWire (mean difference, 8.4 N/mm; P = .01), Ethibond and Omnispan (mean difference, 11.4 N/mm; P = .02), FastFix360 and Meniscal Cinch (mean difference, 6.9 N/mm; P = .03), and Meniscal Cinch and Ultrabraid (mean difference, 7.1 N/mm; P = .04).
ROC Curve Analysis and Logistic Regression Analysis
The ROC curve analysis demonstrated that a construct stiffness threshold of 26.5 N/mm yielded a sensitivity of 66% and specificity of 65% for predicting meniscal repair failure by cheese-wiring during load-to-failure testing (Figure 3). Overall, 60% of menisci with a stiffness >26.5 N/mm failed because of cheese-wiring compared with only 22% that showed a stiffness of ≤26.5 N/mm. The logistic regression analysis demonstrated that meniscal repair with a stiffness >26.5 N/mm had a 3.6 times increased risk of failure due to cheese-wiring during load-to-failure testing (odds ratio, 3.6 [95% CI, 1.4-8.2]; P < .0001) compared with meniscal repair with a stiffness ≤26.5 N/mm.

A receiver operating characteristic curve analysis was performed to determine the optimal stiffness threshold for predicting meniscal repair failure by suture cut-through or anchor pull-through. A threshold of 26.5 N/mm (asterisk) for construct stiffness yielded a sensitivity of 66% and specificity of 65% for a significantly increased risk of meniscal repair failure due to suture cut-through or anchor pull-through in the present study. AUC, area under the curve.
Discussion
The most important finding of the present study is that we showed that the construct stiffness of meniscal repair was associated with cheese-wiring. While the overall mean construct stiffness of all repaired menisci in this study was 24.4 ± 8.1 N/mm, meniscal repair with a higher construct stiffness (>26.5 N/mm) was more likely to fail by cheese-wiring, whereas meniscal repair with a lower stiffness (≤26.5 N/mm) more commonly failed because of loss of suture fixation, knot slippage, or anchor pull-through. The detailed analysis after load-to-failure testing revealed a construct stiffness with loss of suture fixation of 22.7 ± 7.0 N/mm, with knot slippage of 23.0 ± 3.7 N/mm, with cheese-wiring of 29.2 ± 10.1 N/mm, and with anchor pull-through of 24.5 ± 7.0 N/mm (Table 2).
Different modes of failure of meniscal repair have been reported using inside-out sutures and all-inside devices. Lee et al 23 described that inside-out meniscal repair (n = 8 porcine menisci) failed because of suture failure, whereas meniscal repair with all-inside devices (Sequent; n = 8) failed because of implant dislodgement during load-to-failure testing. Beamer et al 7 reported that 78% of inside-out meniscal repair constructs for longitudinal tears failed because of cheese-wiring and 22% because of suture failure, whereas meniscal repair with an all-inside device (Novostitch) failed most commonly because of suture failure (75%) and less frequently because of cheese-wiring (19%) or knot slippage (6%). However, in a recent investigation by the same study group, Masoudi et al 31 reported no difference in the modes of failure between inside-out repair and all-inside repair, with suture failure being the predominant mode of failure (78% for inside-out technique, 89% for the Novostitch, and 100% for the FastFix360).
This is in accordance with the present biomechanical analysis in which loss of suture fixation was the most common mode of failure for all the specimens, except the Omnispan, which failed most commonly because of anchor pull-through (Figure 2). These data might suggest that although the predominant mode of failure for inside-out meniscal repair techniques is suture failure, different all-inside devices might demonstrate different failure modes. A possible explanation for the observed variability in the mode of failure could be the different mechanical properties of the materials used, 40 which might have resulted in different friction coefficients.
Furthermore, the thickness of the sutures may play a role in repair failure, as weaker suture materials showed more distinct gapping at the repair site. 39 However, in this study, sutures with comparable strength and thickness as the all-inside devices were chosen to address this potential confounder.
The construct stiffness of several inside-out sutures and all-inside devices has been previously reported in the literature. In particular, Beamer et al 7 reported a higher stiffness with the Novostitch all-inside device compared with the horizontal inside-out suture (2-0 Force Fiber UHMWPE suture) for the repair of radial meniscal tears in 36 porcine menisci. On the other hand, Lee et al 23 could not find significant differences in construct stiffness comparing an all-inside device (Sequent) and a 2-0 polyester inside-out suture in 16 porcine meniscal tears. Likewise, Masoudi et al 31 compared the biomechanical properties of 2 all-inside devices (Novostitch and FastFix360) with an inside-out suture for the repair of longitudinal meniscal tears in 36 porcine menisci during cyclic loading (maximum of 500 cycles) and load-to-failure testing and reported no significant differences.
This finding was confirmed in our biomechanical analysis in which we could not find significant differences in the overall construct stiffness between inside-out repair and all-inside repair. However, a subgroup analysis revealed significantly different stiffness values among the inside-out sutures and all-inside devices (Table 3). The highest construct stiffness was observed for the Omnispan (all-inside; 30.8 ± 3.5 N/mm), followed by the FiberWire and Orthocord (inside-out; 26.4 ± 7.3 and 26.3 ± 3.1 N/mm, respectively), whereas the lowest stiffness was observed for the Meniscal Cinch (all-inside; 18.0 ± 8.8 N/mm) and Ethibond (inside-out; 19.4 ± 7.8 N/mm). Contrary to our results, Barber et al 4 reported no significant differences in stiffness among several meniscal repair techniques (Orthocord, Ethibond, FastFix360, Omnispan, Meniscal Cinch) in 70 adult human menisci, which might be attributed to the utilization of older human cadaveric menisci that may demonstrate less consistent biomechanical properties due to degeneration than porcine menisci 36 and to the different experimental setup, as they performed only 200 loading cycles between 5 N and 50 N.
It is estimated that meniscal repair with a higher stiffness could lead to suture cut-through (cheese-wiring) compared with meniscal repair with a lower stiffness. Lambrechts et al 21 reported a greater cut-through distance in 16 human cadaveric supraspinatus tendons if repaired with sutures that showed a higher stiffness (FiberWire) compared with sutures with a lower stiffness (Orthocord). This is corroborated by Rosso et al 37 and Barber et al, 5 who both reported that meniscal repair with a higher stiffness had a higher percentage of cheese-wiring.
This is confirmed by our findings: 60% of meniscal repair cases with a stiffness >26.5 N/mm failed because of cheese-wiring in contrast to only 22% of meniscal repair cases with a stiffness ≤26.5 N/mm. Furthermore, meniscal repair with a stiffness >26.5 N/mm showed a 3.6 times increased risk of failure by cheese-wiring during load-to-failure testing compared with meniscal repair with a stiffness ≤26.5 N/mm (95% CI, 1.4-8.2; P < .0001).
The present study should be interpreted in light of its potential limitations. The main drawback was the use of porcine menisci instead of human menisci. However, the relative scarcity of human menisci from young donors makes it impractical to perform biomechanical investigations on human tissue, at least in numbers necessary to obtain statistically significant results. The use of porcine menisci ensures a comparable composition and tissue quality without meniscal degeneration, which is a common finding in human cadaveric menisci obtained from elderly donors. Furthermore, healthy porcine menisci are known to have a similar collagen fiber orientation to human menisci 2 and have demonstrated similar biomechanical properties to those of young adult human menisci. 4,36
While medial and lateral menisci are both wedge-shaped and semilunar, the lateral meniscus has a greater variety in size, shape, and thickness with a smaller maximal and mean thickness compared with the medial meniscus. 10,28 However, no differences in collagen or extracellular matrix composition or tensile strength have been described comparing the medial and lateral menisci. 15,28 In our study, menisci were randomly assigned to the repair groups, and no further differentiation between medial and lateral samples was made, which is common practice in other studies as well. 7,23,31,34
Because this is a biomechanical evaluation of a worst-case scenario simulating a perpendicular load on single-passage vertical meniscal repair, the results might not be unconditionally transferred to actual patients, bearing in mind complex knee kinematics including rotational and shear forces. 8 On the other hand, a particular strength of this work is that, to the best of our knowledge, the present study is the only available report investigating a potential relationship between construct stiffness and cheese-wiring under cyclic loading conditions.
Conclusion
Meniscal repair with a high construct stiffness (>26.5 N/mm) had a 3.6 times higher risk of failure by suture cut-through (cheese-wiring), whereas meniscal repair with a low construct stiffness (≤26.5 N/mm) was more likely to fail by loss of suture fixation, knot slippage, or anchor pull-through. While cheese-wiring is an issue that all knee surgeons face, so far, little evidence about triggering factors exists. This study provides evidence that a high construct stiffness was associated with a higher risk of meniscal repair failure due to cheese-wiring and therefore expands surgeons’ knowledge of the biomechanical properties of different meniscal repair techniques as well as their modes of failure. The results could thus be helpful in decision-making and finding the best repair technique to improve the stability and healing probability of meniscal repair.
Footnotes
Acknowledgment
The authors thank DePuy Synthes, Arthrex, and Smith & Nephew for providing the all-inside devices and inside-out sutures.
Final revision submitted March 21, 2021; accepted April 14, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: The all-inside devices and inside-out sutures used in this study were provided by DePuy Synthes, Arthrex, and Smith & Nephew. C.R. has received consulting fees from LIMA and DePuy Synthes and research support from Stryker, Zimmer, LIMA, Arthrex, DePuy Synthes, Smith & Nephew, and IBSA. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.