
Abstract
Background:
Anterior cruciate ligament (ACL) reconstruction can be performed with different techniques for independent and transtibial (TT) drilling of femoral tunnels, but there is still no consensus on which approach leads to the best outcome.
Purpose:
To assess whether the independent or TT drilling approach for ACL reconstruction leads to the best functional outcomes.
Study Design:
Systematic review; Level of evidence, 2.
Methods:
A systematic literature search was conducted on July 1, 2020, using the PubMed, Web of Science, Cochrane Library, and Scopus databases. The influence of different femoral drilling techniques was analyzed through a meta-analysis in terms of patient-reported outcome measure scores, risk of complications, range of motion limitations, graft failure, and differential laxity. Subanalyses were performed to compare the different independent drilling techniques considered. Linear metaregression was performed to evaluate if the year of study publication influenced the results. The risk of bias and quality of evidence were assessed following the Cochrane guidelines.
Results:
A total of 22 randomized controlled trials including 1658 patients were included in the meta-analysis. Both International Knee Documentation Committee (IKDC) subjective score and Lysholm score were higher with the independent drilling approach (mean difference [MD], 1.24 [P = .02] and 0.55 [P = .005], respectively). No difference was documented in terms of the risk of reinjury, but independent drilling led to reduced KT-1000 arthrometer–assessed anterior tibial translation (MD, 0.23; P = .01) and a higher probability of a negative postoperative pivot-shift test finding (risk ratio, 1.13; P = .04). There were no significant differences in IKDC objective or Tegner scores. A P value of .07 was found for the association between the year of the study and IKDC objective scores.
Conclusion:
Independent femoral tunnel drilling provided better results than the TT approach, although the difference was not clinically significant. No difference was observed in the risk of reinjury. Increasingly better results were seen among surgical procedures performed in more recent years. Among the independent drilling options, the anteromedial portal technique seemed to provide the most favorable outcomes. The lack of clinically significant differences and the promising outcomes reported with new modified TT techniques suggest the importance of correct placement, rather than the tunnel drilling approach, to optimize the results of ACL reconstruction.
Anterior cruciate ligament (ACL) reconstruction is one of the most common orthopaedic surgical procedures in the world, with more than 100,000 patients treated per year in the United States alone. 15,28,31,47 Despite its general good results in terms of stability, subjective outcomes, and return to sport, between 3.2% and 11.1% 30 of patients experience reruptures or require a revision procedure. Moreover, postoperative osteoarthritis is a common finding reported after ACL reconstruction, with a reported prevalence of 11.3%. 9 One of the main technical aspects influencing the biomechanics of ACL reconstruction, which is believed to be responsible for failures and poor outcomes, is incorrect femoral tunnel graft placement. 20 This has led to the most current approach to ACL surgery, which aims to obtain graft placement as close as possible to the native anatomy. 33 Numerous biomechanical and cadaveric studies have been performed trying to identify the best available technique to place the ACL graft within the native anatomic footprint. 25
Despite the lack of a universally accepted definition of “anatomic ACL reconstruction” and acknowledging the controversies in the definition of the ACL anatomy, most authors agree that the anatomic insertion of the ACL lies in the inferior segment of the intercondylar notch extending between 9 o’clock and 11 o’clock. 2,27,37 Stated another way, the optimal graft placement from an anatomic and biomechanical point of view is believed to be aiming toward the center of the ACL native footprint. 52 The pursuit of restoring the ACL anatomy by placing the graft in a “central” position creates technical challenges, as this position has been demonstrated to be more difficult to achieve by classic transtibial (TT) drilling. This approach can lead to less anatomic placement in the intercondylar notch, making TT drilling a suboptimal technique to perform anatomic ACL reconstruction. In fact, the common consequence of TT drilling is an anterior position of the graft in the lateral view and a more vertical orientation of the tunnel in the coronal plane. 3,8,20,27 This has convinced some surgeons to abandon the TT approach in favor of independent drilling using either the anteromedial (AM) portal, outside-in, or all-inside technique. However, controversial findings have been reported in terms of advantages and disadvantages, and therefore, a consensus on the most suitable approach for tunnel placement is still lacking. Both independent and TT drilling have been alternately linked to a higher incidence of graft failure and poorer clinical outcomes, with opposing findings according to the specific study considered, as the literature is often contradictory over which technique results in the best functional outcomes. 8,12,42 Previous attempts to analyze the available literature have presented several limitations because of either the inclusion of low-level or ex vivo studies or being dated and thus failing to include in the analysis the growing body of high-level trials addressing this key issue in ACL reconstruction. 8,44
The aim of this meta-analysis was to quantitatively analyze the best available literature evidence by including only randomized controlled trials (RCTs) comparing the techniques of independent versus TT drilling of the femoral tunnel in ACL reconstruction. The hypothesis was that independent drilling would lead to better clinical results compared with the TT approach, with a similar rate of graft failure.
Methods
Search Strategy and Article Selection
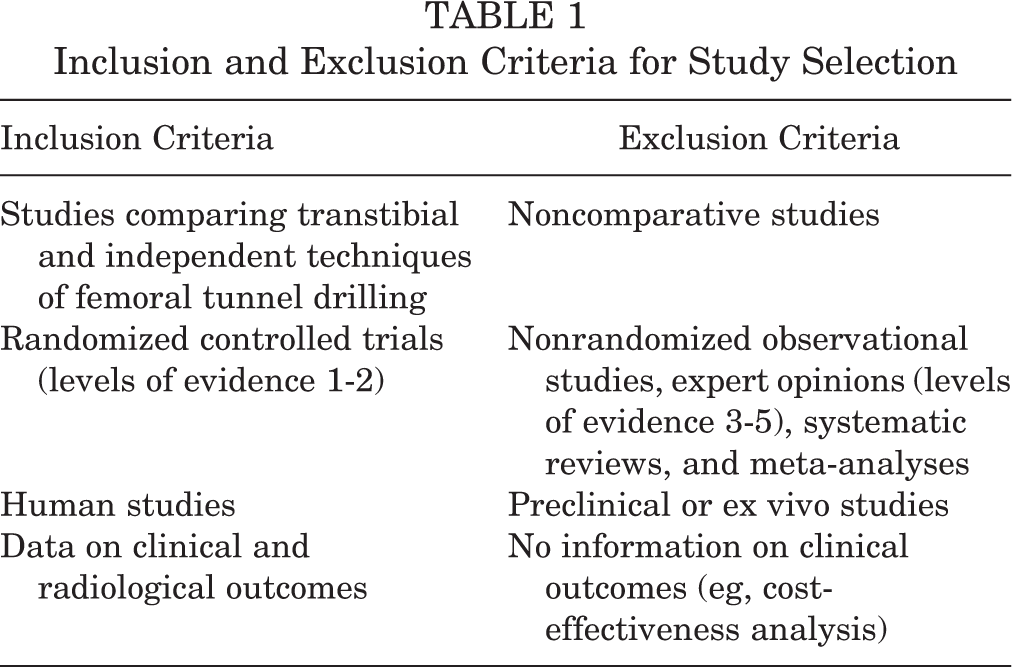
A systematic literature search was conducted on July 1, 2020, using the PubMed, Web of Science, Cochrane Library, and Scopus databases with the following keywords: (anterior cruciate ligament OR ACL) AND (ACL reconstruction) AND (outside-in OR transtibial OR anteromedial OR all-inside OR retrograde drilling OR independent drilling OR anatomic reconstruction). First, all duplicates were removed, and then all records were controlled for eligibility by title and abstract, with a full-text evaluation when needed. Inclusion/exclusion criteria are described in Table 1. The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines were used. 36 The article selection process was independently performed by 2 authors (M.C., D.P.), with disagreements resolved by a consensus or by the intervention of a third author (M.D.). The protocol for this study was registered on PROSPERO (CRD42019156301).
Inclusion and Exclusion Criteria for Study Selection
Data Extraction, Synthesis, and Measurement of Outcomes
Data were independently extracted by 2 authors (M.C., D.P.) from the full-text version or supplementary information of the included articles using a previously structured table according to the Cochrane Collaboration. Information on study methodology included the following: level of evidence, study design (randomization technique, data origin), inclusion/exclusion criteria, ACL femoral tunnel drilling technique, graft source, ACL reconstruction timing (time from injury to surgery), other associated surgical treatments, presurgical rehabilitation, postsurgical rehabilitation, and follow-up length. Patient characteristics and the clinical outcomes of treatments were also considered: number of patients screened, included, and assessed at follow-up; patient sex, age, and body mass index; cause of injuries; associated lesions; preoperative and postoperative patient-reported outcome measure (PROM) scores (International Knee Documentation Committee [IKDC] subjective and objective forms, Lysholm scale, Tegner activity scale, Knee injury and Osteoarthritis Outcome Score); Lachman, pivot-shift, and single-leg hop test results; rate of retears; rate of complications; differential laxity between the index and uninjured knees; residual deficits in flexion; and tunnel length, position, and obliquity. Missing information was requested by contacting the corresponding author.
Assessment of the Risk of Bias and Quality of Evidence
The risk of bias was evaluated using the revised risk of bias tool for randomized trials (RoB 2.0) approved by the Cochrane Collaboration. 18 The overall quality of evidence for each outcome was rated according to the Grading of Recommendations Assessment, Development and Evaluation guidelines. 46
Statistical Analysis
To determine the best technique for femoral tunnel drilling, analyses of different clinical outcomes (IKDC subjective and objective, Lysholm, and Tegner scores; retears; differential laxity; positive Lachman and pivot-shift test results) were performed. The main analysis included all the trials reporting results with a follow-up longer than 6 months. When data from the same study population were available at different follow-ups or in different studies, those closest to 6-month follow-up were selected. The 6-month cutoff for follow-up analysis was chosen because no clinically significant improvement in the selected outcomes has been seen beyond that time. 1 We also performed an assessment of radiological outcomes in terms of femoral tunnel length and position (depth and height) according to Bernard et al. 5
Subanalyses were conducted according to the independent drilling technique used. Subanalyses based on the TT drilling technique were not possible because of the low number of studies reporting on a modified TT technique. However, a sensitivity analysis excluding RCTs using a modified TT approach was also conducted to avoid possible confounding bias due to more anatomic placement of the graft achieved with this approach. The difference between results of the considered outcomes was assessed through the Mantel-Haenszel test and was expressed as risk ratios (RRs) for dichotomous variables (independent vs TT drilling), whereas the inverse variance method, with results expressed as mean differences (MDs), was used for continuous variables. Heterogeneity was tested using the Cochran Q statistic and I 2 statistic and was considered significant when I 2 > 25%. A fixed-effects model was favored in the absence of significant heterogeneity; otherwise, a random-effects model was employed. A P value of .05 was set as the level of significance for all analyses.
Linear metaregression was performed to evaluate if the year of study publication influenced the results, with a P value of .05 for statistical significance. When means and standard deviations were not available from the full-text articles, they were estimated from medians and ranges using the formula of Hozo et al 21 following the Cochrane guidelines. 19 Analyses were performed using RevMan 5.3 software (Cochrane Collaboration).
Results
Article Selection and Patient Characteristics
The PRISMA flowchart of the article selection process is presented in Figure 1. Of the 5089 records extracted, 22 RCTs were included in the quantitative synthesis. Considering the different treatment arms, the TT approach was compared in 13 studies with the AM portal technique, ¶ 6 with the outside-in technique, 14,32,37,40,43,50 and 3 with the all-inside technique. 4,41,45 Moreover, 15 of the studies selected a hamstring tendon graft, # 5 opted for a bone–patellar tendon–bone graft, 13,14,40,41,43 while 3 chose a frozen Achilles tendon allograft. 17,39,51 Further study characteristics are provided in Table S1 of the Supplemental Material.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart of the article selection process.
Overall, 1658 patients were included in this meta-analysis: 840 in the independent drilling group and 818 in the TT drilling group. Among these, 1566 patients were assessed at a minimum 6-month follow-up. The male-to-female ratio was 3 to 1, and the mean age was 28 years. The time from injury to surgery was reported in 11 studies, ** with a mean of 14.1 months ranging from early reconstruction, performed within 3 weeks, to late surgery, performed up to 47 months after the index injury. No significant differences in baseline characteristics were found between the 2 treatment approaches in all included studies. Further patient characteristics are provided in Supplemental Table S1.
Outcomes of Independent Versus TT Drilling
Subjective Outcomes
The meta-analysis of PROMs favored independent drilling, with statistically significant differences in IKDC subjective score (12 RCTs †† : MD, 1.24; P = .02) and Lysholm score (14 RCTs ‡‡ : MD, 0.55; P = .005) (Figures 2 and 3) but not in terms of Tegner score (10 RCTs §§ : MD, 0.11; P = .36) (Supplemental Figure S1).

Forest plot for the International Knee Documentation Committee (IKDC) subjective score. IV, inverse variance.

Forest plot for the Lysholm score. IV, inverse variance.
Knee Laxity
Significantly higher postoperative anteroposterior laxity, measured with KT-1000 and KT-2000 arthrometers, was found in patients in whom the TT technique was used (Δlaxity; 14 RCTs ∥∥ : MD, 0.23; P = .01) (Figure 4); a similar finding was reported for the pivot-shift test as well (14 RCTs ¶¶ : RR, 1.13; P = .04) (Supplemental Figure S2). No significant differences were found for the Lachman test (10 RCTs ## : RR, 1.05; P = .25) (Supplemental Figure S3).

Forest plot for differential laxity between the index and uninjured knees. IV, inverse invariance.
Objective Outcomes and Failure
No significant differences were found for the rate of normal/quasinormal IKDC objective scores (14 RCTs a : RR, 1.02; P = .21) (Supplemental Figure S4) or the risk of retears (7 RCTs 16,22,32,34,35,40,50 : RR, 0.96; P = .91) (Figure 5).

Forest plot for the risk of retears. M-H, Mantel-Haenszel.
Radiological Outcomes
Independently drilled tunnels were significantly shorter (6 RCTs 14,16,34,37,39,51 : MD, 8.72; P = .001) and were placed closer to the native ACL footprint. These results were strengthened by the sensitivity analysis excluding the studies of Han et al 17 and Hussin et al, 23 which used a modified TT technique (Supplemental Figure S5).
Linear Metaregression
A P value of .07 was found for the association between the year of the ACL reconstruction study and the IKDC objective score. No association was found between the other PROM scores and the year of the ACL reconstruction study, as they were not reported in the older RCTs.
Outcomes of Different Independent Drilling Techniques
Subanalyses evaluating the best technique among the different independent drilling approaches showed that the AM portal technique had the highest Lysholm score (11 RCTs b : MD, 0.68; P = .001) and Tegner score (6 RCTs 6,13,17,35,39,51 : MD, 0.27; P = .004) versus the TT approach, while statistical significance was not reached with the IKDC subjective (8 RCTs 6,13,16,17,22,23,34,51 : MD, 1.03; P = .08) or IKDC objective (8 RCTs 6,16,22,23,29,35,39,51 : RR, 1.04; P = .08) scores. Also, the AM portal technique was better in terms of residual laxity (8 RCTs 6,13,17,22,29,35,39,53 : MD, 0.28; P = .007), and a tendency toward favoring the AM portal technique was seen for the results of both the Lachman and pivot-shift tests (P = .08 and .09, respectively). The sensitivity analysis excluding the 2 RCTs 17,23 with a modified TT technique confirmed all the previous differences, and both the Lachman and pivot-shift tests reached statistical significance in favor of the AM portal technique (P = .03 and .04, respectively).
Risk of Bias and Quality of Evidence
The risk of bias was low in 19 RCTs, c and there were some concerns in 3 of the studies. 43,45,49 In particular, the lack of blinding for patients and assessors and the unclear method of randomization and allocation were the main issues that raised concerns over their methodological quality. Details on the risk of bias assessment are presented in Figure 6. The quality of evidence in the overall analysis as well as the subanalyses of the different independent drilling techniques was high for the IKDC subjective score, IKDC objective score, and differential laxity between the index and uninjured legs, whereas it was moderate for the Lysholm score, Tegner score, risk of retears, and Lachman and pivot-shift tests. The quality of evidence was low for all radiological outcomes. In the follow-up analysis, the level of evidence was still high for the IKDC subjective score, IKDC objective score, and differential laxity; it was low for all other outcomes. In particular, no level of evidence was downgraded for the risk of bias, indirectness, and publication bias. Regarding imprecision, there was a downgrade of 1 level for the Tegner score, risk of retears, Lachman test, and radiological outcomes. Finally, there was a downgrade of 1 level for the Lysholm score and all the radiological outcomes in the overall analysis because of inconsistency.

Risk of bias of included randomized controlled trials. Green = low risk, yellow = moderate risk, and red = high risk. Risk of bias items: 1 = randomization process; 2 = effect of assignment to intervention; 3 = effect of adhering to intervention; 4 = risk of bias related to missing data; 5 = risk in the measurement of the outcome; 6 = risk in the selection of the reported results; 7 = overall.
Discussion
The main finding of this meta-analysis was that independent drilling of the femoral tunnel in ACL reconstruction produced better PROM scores with a similar rate of reinjures compared with TT drilling. Moreover, independent drilling resulted in reduced postoperative laxity, better pivot-shift test findings, and higher radiological outcomes. This meta-analysis described clear outcomes that could seem statistically compelling in terms of the treatment choice and expected benefits. However, despite a statistical significance, the documented advantages of independent drilling in terms of PROM scores are possibly not clinically relevant. In fact, the resulting overall improvement was lower than what is considered the minimal clinically important difference. 11 Accordingly, because of the limited magnitude of treatment effects, these differences should be considered with caution and interpreted in a more critical light in terms of clinical relevance. From a clinical point of view, results look less compelling for the choice of a femoral drilling approach. In this perspective, a more balanced conclusion could be that, given the well-controlled experimental setting of these RCTs, the outcomes of ACL reconstruction were substantially similar, with some evidence of a benefit leaning toward the AM portal technique.
These conclusions contrast with those of the previous literature and represent important findings that shed new light on a controversial technical issue in the field of ACL surgery. As such, a great paradox has risen from recent evidence related to femoral tunnel drilling techniques. Considering the strong biomechanical rationale for central anatomic ACL reconstruction through the independent drilling approach, 25 improved outcomes in terms of failure would have been expected. On the contrary, 3 different studies evaluating almost 20,000 patients identified the AM portal technique as having an increased risk of revision, ranging from 1.4 to 2.0 times that of the TT approach. 9,10,42 There are several possible explanations for this unexpected finding. First of all, considering the inherent nature of studies in which multiple surgeons with heterogeneous surgical skills are involved, the surgeons’ learning curve as well as their personal opinion regarding tunnel placement could have contributed to the higher revision rate of the AM portal technique. Supporting this is the fact that patients operated on in the first years during the learning curve before popularization of the AM portal technique 42 and those with nonanatomic graft placement 7 had the worst outcomes within those who underwent reconstruction with an independent drilling approach. A second issue is related to fixation methods, as a higher revision risk was reported using suspensory fixation, which is typical of the AM portal technique, as opposed to the cross-pin and interference screws usually used in the TT drilling approach. 48 Third, a recent single-surgeon case series of 1480 patients by Clatworthy et al 10 identified a higher risk of failure when the AM portal technique was used compared with the TT approach. However, the different drilling techniques coincided with different graft placement: a “central” footprint position was in fact achieved with the AM portal, while an “eccentric” position within the native footprint, close to the insertion of the ACL direct fibers, was obtained with the TT technique. 26 As such, the TT approach may be associated with a different joint response to physical stress.
The ACL direct insertion consists of dense collagen fibers in the anterior part of the footprint, connecting it to a bony depression immediately posterior to the lateral intercondylar ridge. The indirect insertion is made up of lighter fibers that extend posteriorly to mingle with the articular cartilage of the lateral femoral condyle. This difference in the histological composition suggests how these regions also have different roles in load bearing. Kawaguchi et al 24 and Nawabi et al 38 showed how 80% of the load during stability testing is taken by the AM region of the native ACL footprint and is more isometric during knee flexion than posterior fibers. In fact, registry results have implied that a central or posterolateral position of the tunnel in the native ACL footprint results in a less isometric graft and higher failure rates. 42 These data suggest that the increased failures reported in the registry were more likely an issue of tunnel placement rather than the learning curve or drilling technique. An analysis of precise graft positioning within the footprint was not possible in the current meta-analysis, as data on this subject were missing or very heterogeneous.
Still, the latter considerations give important insight in light of the findings of the present meta-analysis. The main characteristic of the studies included in the present meta-analysis was the strict experimental and controlled setting, with well-defined inclusion criteria, accurate descriptions of the surgical techniques, and clear outcome evaluations. Unlike registry studies, in the RCTs included in this meta-analysis, it was often the same surgeon who performed ACL reconstruction using different drilling techniques, as we tried to standardize as much as possible the other confounding variables such as operators, graft placement, and fixation methods. Thus, both reconstructions with the TT or independent drilling technique are believed to be performed trying to pursue the same graft position and within the personal interpretation of ACL anatomy. In this light, because of the lack of standardization of graft placement within the studies included in this meta-analysis, as well as the inconsistent postoperative evaluations of effective graft positioning, it is impossible to offer any firm recommendation regarding the effect of graft positioning with the different drilling techniques.
We suggest that the findings of the present meta-analysis be interpreted as follows: When performed in a controlled setting by the same surgeon, the outcomes of ACL reconstruction are less dependent on the femoral tunnel drilling technique than previously reported, and the lack of a clear definition of graft placement could be an important factor explaining the heterogeneous literature findings. As an example, Clatworthy et al 10 reported an increased failure rate after switching from an “eccentric” graft with TT drilling to a “central” graft with AM portal drilling. However, they reported that they reverted to the previous failure rate after returning to “eccentric” placement but with the AM portal approach. Given this, the interest should shift from how the tunnel is placed to where it is placed, disrupting the belief in the connection between nonanatomic placement and TT drilling as well as between anatomic placement and independent drilling. Keeping in mind the variable and somewhat subjective nature of the ACL anatomy, now, it is clear that anatomic graft placement could be obtained with modified TT drilling, while nonanatomic placement could be achieved even with independent drilling if the ACL anatomy is not strictly respected. In fact, thanks to a deeper knowledge of the ACL anatomy, many more recent reports describing the use of the TT technique include modifications to the tibial tunnel to allow more anatomic graft placement at the femur by improving better access to the footprint with a less vertical and more oblique tibial tunnel. Thus, vertical graft placement, performed by many in the 1990s, has recently been discouraged and practically abandoned.
The previous literature has relied on low-level studies or attempts to analyze combined data, leading to level 3 to 4 meta-analyses. In particular, because of the lack of high-level clinical studies, cadaveric and nonrandomized observational studies were also included, with clear methodological faults. Furthermore, the previously published meta-analyses did not consider all the different techniques of independent drilling. The study of Riboh et al 44 was the only one comparing the TT approach and more than 1 independent drilling technique (AM portal and outside-in), but the authors could not find any statistically significant difference between the 2 independent drilling techniques, having included only 5 RCTs. The present meta-analysis takes advantage of a larger number of high-level trials to provide the first quantitative synthesis of the literature considering only RCTs, showing both the overall benefits of the independent drilling approach as well as the most suitable technique of independent drilling. The most recent literature comprised several important studies, leading to the possibility of surpassing previous literature limitations and having stronger elements to discuss the most suitable independent drilling approach. On the other hand, other questions still remain unanswered. To surpass TT drilling limitations, some modifications were made to this approach to achieve more anatomic tunnels: the knee was flexed to 60°, and a varus force along with internal rotation on the proximal tibia was applied. The sensitivity analysis excluding those RCTs 17,23 with this modified TT technique strengthened the results of the overall analysis, suggesting how a modified TT approach could offer better results than the classic TT technique. However, whether this can be a valid alternative to attain an anatomic position of the graft and, in the end, better results still needs to be confirmed by more RCTs.
The available literature also presents other limitations. First of all, it must be considered that the minimal clinically important difference should be used to evaluate the relevance of an improvement for a single patient rather than to evaluate the clinical significance of an improvement for a group. Thus, more data are needed to understand the clinical relevance of these findings. Further trials comparing independent and TT drilling in terms of the number of patients achieving a clinically significant improvement will help to clarify if the statistically significant advantage of independent drilling documented in this meta-analysis is relevant for clinical practice. Furthermore, even if many outcomes were considered, the activity level and the time to return to sport are 2 key aspects, especially in competitive athletes, but they could not be properly assessed because of the lack of specific data. Finally, even if a direct comparison goes beyond the main aim of this study, the subanalyses pointed out the AM portal to be the technique of choice, showing superior results in terms of laxity and PROM scores and even allowing patients to perform at higher levels of activity. However, data comparing these techniques are supported by an indirect comparison and thus should be confirmed by specific RCTs to provide a definite conclusion.
Overall, both approaches led to positive outcomes, and the findings of this meta-analysis suggest that further RCTs should be conducted to examine different graft placement approaches rather than to study the mere technical aspects of tunnel drilling. Moreover, patients’ activity levels should be better evaluated to understand if there might be different results and indications according to the specific requirements. Despite the publication of new RCTs, some of the outcomes were reported only in few trials, some required an estimate of the standard deviation, and their quality of evidence was still low. A certain degree of heterogeneity in the rehabilitation protocols has also been observed. Even though all modern accelerated rehabilitation protocols are reported to be valid, this could introduce a bias in the results while summarizing the overall literature. Finally, follow-ups were very heterogeneous, and long-term outcomes, with a radiological evaluation for the development of osteoarthritis, were lacking, all factors that should be considered in future trials aimed at improving the technique and outcomes of ACL reconstruction.
Conclusion
This meta-analysis of RCTs demonstrated that independent femoral tunnel drilling provided better results than the TT approach, although the difference was not clinically significant. No difference was observed in the risk of reinjury. In addition, there were increasingly better results with surgery performed in more recent years. Among the independent drilling options, the AM portal technique seemed to provide the most favorable outcomes. The lack of clinically significant differences and the promising outcomes reported with new modified TT techniques suggest the importance of correct placement, rather than the tunnel drilling approach, to optimize the results of ACL reconstruction.
Supplemental material for this article is available at http://journals.sagepub.com/doi/suppl/10.1177/23259671211015616.
Supplemental Material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671211015616 - Independent Versus Transtibial Drilling in Anterior Cruciate Ligament Reconstruction: A Meta-analysis With Meta-regression
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671211015616 for Independent Versus Transtibial Drilling in Anterior Cruciate Ligament Reconstruction: A Meta-analysis With Meta-regression by Marco Cuzzolin, Davide Previtali, Marco Delcogliano, Giuseppe Filardo, Christian Candrian and Alberto Grassi in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted November 3, 2020; accepted December 2, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: G.F. has received institutional support from Finceramica Faenza, Fidia Farmaceutici, CartiHeal, EON Medical, IGEA Clinical Biophysics, Biomet, and Kensey Nash outside the submitted work. C.C. has received grants from Medacta, Johnson & Johnson, Lima, Zimmer Biomet, and OPED outside the submitted work. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.