
Abstract
Background:
Anterior cruciate ligament (ACL) injuries are occurring with increasing frequency in the adolescent population. Outcomes after ACL reconstruction (ACLR) are inconsistently reported in homogeneous patient populations.
Purpose/Hypothesis:
To evaluate outcomes after bone–patellar tendon–bone (BTB) autograft ACLR in competitive high school–aged athletes by examining return to sport (RTS), patient satisfaction, and reinjury rates. Our hypothesis was that RTS rates and satisfaction will be high and reinjury rates will be low.
Study Design:
Case series; Level of evidence, 4.
Methods:
An institutional ACL registry was utilized to identify competitive high school–aged athletes (14-18 years old) who underwent primary ACLR using BTB autograft with a minimum 2-year follow-up. A postoperative questionnaire was administered to determine rates and types of RTS, quality of sports performance, reinjury, and satisfaction. Uni- and multivariable analyses were used to identify demographic, sport-specific, and clinical factors related to RTS.
Results:
A total of 53 patients were included (mean ± SD age at the time of surgery, 16.6 ± 1.34 years). Mean follow-up was 3.78 ± 0.70 years (range, 2.60-4.94 years). The overall ipsilateral ACL retear rate was 7.5% (n = 4). There were 10 subsequent ACL tears to the contralateral knee (19%). Forty-four (83%) patients successfully returned to at least their prior level of sport at a mean 10.5 ± 8.7 months (range, 3-48 months). Overall satisfaction was high, with 91% of patients very satisfied with the outcome. Higher confidence levels regarding performance of the reconstructed knee were associated with increased probability of RTS on multivariate analysis.
Conclusion:
BTB autograft ACLR results in high rates of RTS and satisfaction and low rates of subsequent ipsilateral ACL injuries in competitive high school–aged athletes. Patients with higher confidence in performance of the reconstructed knee are more likely to return to at least their prior level of sport.
Keywords
Anterior cruciate ligament (ACL) injuries and ACL reconstruction (ACLR) are occurring with increasing frequency in adolescent athletes. 10,31 A rise in organized athletic competition among children and adolescents, in addition to early sport specialization, higher awareness of ACL injuries, and year-round training, has resulted in a growing number of ACL injuries in this population. 13,15,31 As these rates of injury have risen, recent investigations have noted a nearly 3-fold increase in rate of ACLR in patients aged ≤20 years. 10,13
Revision rates among adolescent patients after ACLR are substantially higher than adults. 14,15,17,34 Several studies have shown that adolescent females are at particularly high risk for revision, with revision rates in teenage female soccer players as high as 22%. 1,15 Multiple studies have demonstrated autograft to be superior to allograft when performing ACLR in adolescent populations 11,12,16 ; however, the optimal autograft choice in adolescent athletes has yet to be determined. While several studies have demonstrated lower revision rates for bone–patellar tendon–bone (BTB) ACLR than for hamstring autograft ACLR, 20,27 several studies have also shown no difference in revision rates. 2,17 Consideration of the growth plates must be made for younger patients; however, after 14 years in boys and 12 to 13 years in girls, there is minimal growth remaining around the knee (<1 cm in each limb segment). 18 Transphyseal reconstruction using BTB autograft has been shown to have minimal risk for leg-length discrepancy or angular deformity in adolescents who are approaching skeletal maturity. 19,30
The outcomes of orthopaedic interventions are increasingly being determined by patient-reported factors. With regard to ACLR, return to sport (RTS) and patient satisfaction are critical parameters by which to judge success of the operation. Furthermore, revision rates are important to consider, particularly in an at-risk athletic adolescent population. A heterogeneous grouping of patient age, graft type, and competitive level of the athlete compromises the ability to draw strong conclusions for many studies examining ACLR. 9,21,23,29
RTS, reinjury rates, and patient satisfaction after BTB ACLR in competitive high school–aged athletes have not been defined. Our hypothesis was that rates of RTS and satisfaction will be high and reinjury rates will be low after BTB ACLR in competitive high school–aged athletes.
Methods
Patients in this study had been prospectively enrolled in an institutional ACL registry at the Hospital for Special Surgery between 2009 and 2013. As part of the registry, demographic and patient-reported outcome measures are recorded preoperatively as well as at 6 months, 1 year, and 2 years postoperatively. Patient age, sex, race/ethnicity, body mass index (BMI), and sports activity are also recorded, as are the following clinical variables: mechanism of injury, presence and location of any concomitant meniscal injury, and graft type. Patient-reported outcome measures captured within the registry include the International Knee Documentation Committee (IKDC) Subjective Knee Evaluation, Lysholm Scale, Tegner Scale, Marx Activity Scale, and 12-Item Short Form Health Survey (SF-12) physical and mental component summaries.
At our institution, graft selection is accomplished on a case-by-case basis through an informed decision-making process between the patient and surgeon. All patients in this investigation underwent ACLR using a BTB autograft. In addition, intraoperative data, including concomitant injuries and procedures, were provided by the treating surgeons at the time of surgery. During the study period, 24 surgeons from the institution’s sports medicine department contributed cases to the registry. We obtained institutional review board approval to query the registry to identify eligible patients.
Inclusion criteria were competitive athletes aged 14 to 18 years at the time of surgery undergoing BTB ACLR with minimum 2-year follow-up. Perioperative radiographs were examined to assess skeletal maturity. Status as a competitive athlete was determined by the patient’s self-report that he or she played competitive soccer, basketball, lacrosse, football, tennis, or skiing and that the patient had a maximum score on the Marx Activity Scale preoperatively. 22 Exclusion criteria were multiligament knee injuries and concomitant lateral extra-articular tenodesis. After screening criteria were applied, 53 patients were identified as eligible for the study.
A nonvalidated RTS survey, similar to that utilized by the Multicenter Orthopaedic Outcomes Network (MOON) group, 23 was administered by mail or telephone postoperatively by a single research coordinator who did not have prior involvement in the clinical care of the patients. This was administered at a minimum of 2 years after surgery. If patients were unable to be reached by phone, a voicemail was left, and a minimum of 3 attempts were made to contact patients via telephone. Additionally, for patients unable to be reached by phone, the survey was mailed to their last known address. This process was conducted similarly to those in previous investigations pertaining to RTS after ACLR. 23,24
Patients were asked questions to determine their satisfaction, return to sport, date of return, repeat injury, and factors influencing their ability or inability to RTS, including confidence levels with the reconstructed knee. To determine if patients were able to return to play at the same level as before the initial injury, patients were asked the level of competitive sport before and after ACLR (recreational, high school, amateur, college, semiprofessional, or professional). Within this survey, patients were assessed for quality of return to play as determined by sports experience questions related to effort, performance, and pain during participation. If patients were unable to RTS, they were asked if the reason was related to fear or physical limits or was unrelated to the knee. Patient satisfaction was determined using an ordinal satisfaction scale, with possible responses limited to very satisfied, somewhat satisfied, neither satisfied nor dissatisfied, somewhat dissatisfied, and very dissatisfied.
Uni- and multivariate analyses were performed to assess demographic and clinical factors associated with RTS. Demographic variables were age, BMI, sex, and race/ethnicity. Clinical variables were primary sport played (basketball, football, lacrosse, skiing, or soccer), mechanism of injury (contact, noncontact, or unknown), and presence or absence of concomitant meniscal injury (medial, lateral, or combined). Additionally, correlation was performed between RTS and 3 confidence questions (confidence that one can perform well, that one can perform at the prior level, and that the knee will not give way). Patients rated their confidence for each question on a scale of 0 to 10, with 10 being the most confident. Statistical significance was set at P < .05. Analyses were performed using SAS Version 9.3 (SAS institute).
Results
A total of 2106 primary ACLRs were performed and included in our institution’s ACL registry during the study period. Screening for patients aged 14 to 18 years who had no other ligament injury requiring surgery and were active athletes (maximum Marx scores) yielded 270 patients. Further screening based on ACLR with BTB autograft led to 143 eligible patients for the study. Of these, 53 patients had a minimum 2-year follow-up (37% follow-up rate) (Figure 1).

Flowchart of inclusion and exclusion criteria. ACLR, anterior cruciate ligament reconstruction; BTB, bone–patellar tendon–bone.
Demographics and preoperative patient-reported outcome scores were compared between the groups with and without follow-up (Table 1). There was no difference in age, race/ethnicity, preoperative SF-12 physical or mental component score, or Lysholm score between the groups. There was also no difference in mechanism of injury (contact vs noncontact) or presence of meniscal injuries. The group with 2-year follow-up had a higher percentage of females (71.7% vs 51.1%; P = .008), a slightly lower BMI (22.3 vs 23.3; P = .043), a lower preoperative IKDC (50.0 vs 55.8; P = .022), and a higher percentage of patients with soccer as their primary sport (49.1% vs 32.2%; P = .046).
Comparison of Baseline Data for Patients With and Without Follow-up a
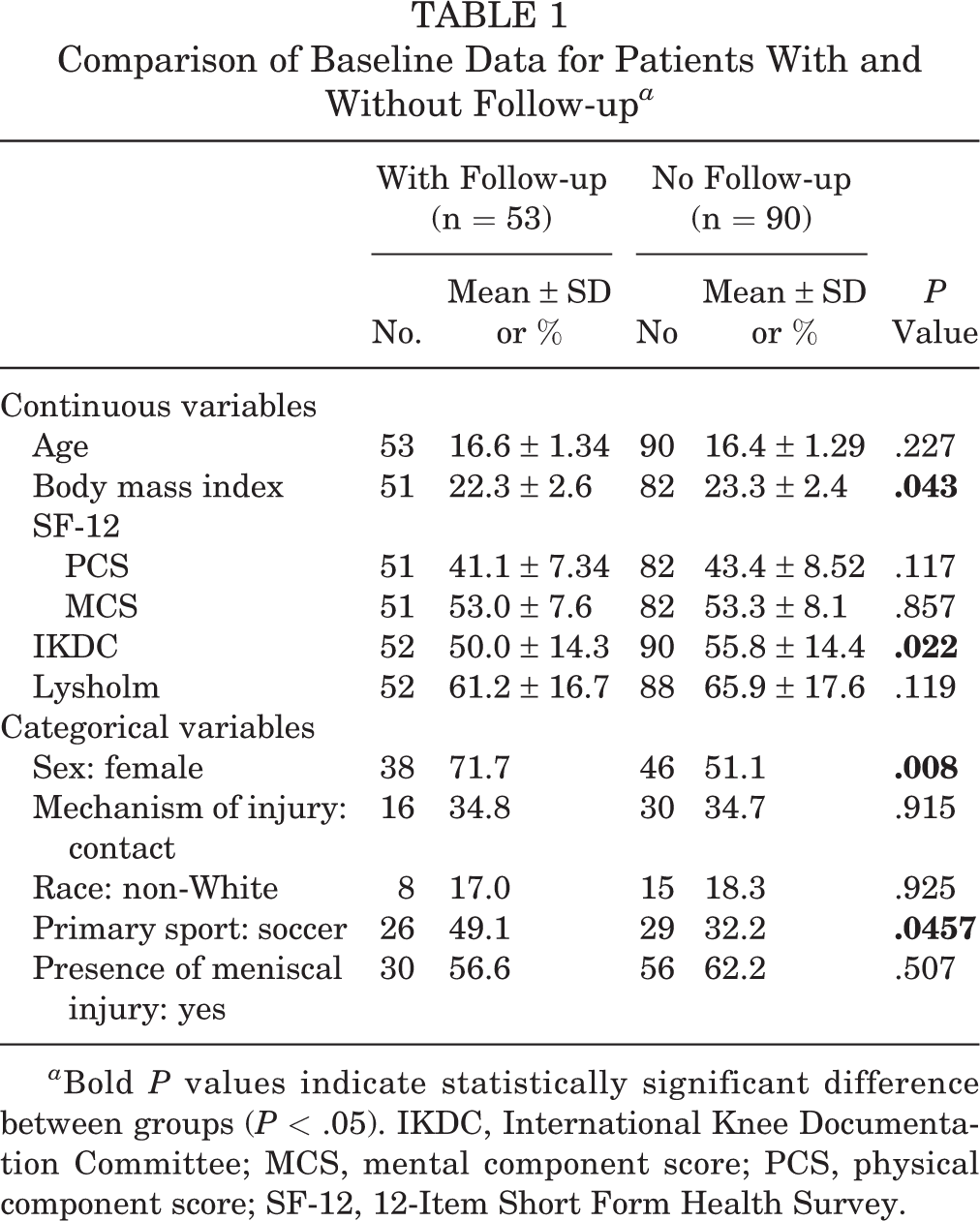
a Bold P values indicate statistically significant difference between groups (P < .05). IKDC, International Knee Documentation Committee; MCS, mental component score; PCS, physical component score; SF-12, 12-Item Short Form Health Survey.
Patient Demographic and Clinical Characteristics
The mean ± SD age at the time of surgery was 16.6 ± 1.34 years (range, 14.2-18.7), with a mean follow-up of 3.78 ± 0.70 years (range, 2.60-4.94 years); 38 (72%) patients were female while 15 were male (28%). The majority of patients had closed or almost closed physes (n = 46; 87%) at the time of surgery. Almost closed physes were defined as when there was not complete closure of the physes but there was no longer a continuous line in the distal femoral or proximal tibial physes on radiographs and magnetic resonance imaging (MRI). Based on an MRI study, physeal maturation occurs uniformly throughout the distal femur and proximal tibia; therefore, once any discontinuous line is present at the physis, the risk of growth or angular disturbance with transphyseal drilling is minimal. 21
Four patients (7.5%) had approximately 50% of their distal femoral and proximal tibial physes open at the time of surgery, and 3 (5.6%) did not have perioperative radiographs available for review. There were no clinically significant leg-length discrepancies or angular deformities at follow-up, and no patients underwent procedures to correct deformities.
Regarding concomitant injuries, 30 (56.6%) patients had a meniscal tear. Five patients (9.4%) had recurvatum on preoperative physical examination. Fourteen surgeons performed the 53 BTB ACLRs, and interference fixation was used on the femur and tibia in all cases. The most common mechanism of injury was noncontact (30 patients; 56.6%). Soccer was the most common sport (26 patients; 49.1%), followed by lacrosse (11 patients; 20.8%), basketball and football (6 patients each; 11.3% each), and skiing (4 patients; 7.5%) (Table 2).
Demographic and Clinical Characteristics of Study Population (N = 53)

a Values are presented as No. (%) unless noted otherwise.
Return to Play and Satisfaction
A total of 44 patients (83%) reported a successful return to at least their prior level of sport at final follow-up. Of the 9 (17%) patients who did not return to prior level of play, 5 had aged out of high school athletics at the time of their follow-up. Of the 44 patients who returned to play, the mean time to return was 10.5 ± 8.7 months (range, 3-48 months). The 9 patients who indicated being unable to return to prior level of sport cited the following reasons: physical limits attributed to the knee (5 patients; 56%), fear of reinjury or injury to the other knee (3 patients; 33%), and not knee related (1 patient; 11%). Of the 47 patients who indicated satisfaction with knee surgery, 43 (91%) felt very satisfied and 4 (9%) satisfied. When reporting on sports experience after surgical intervention, just under half of respondents (23 of 51 patients; 45%) cited unlimited effort and performance without pain (Table 3). Visual analog scale (VAS) scores were completed by 52 patients with regard to confidence in their reconstructed knee, with higher scores indicating more confidence. When asked if they could perform well at their sports, patients scored a mean VAS of 8.27 ± 2.57 (range, 0-10). When asked if they could perform at their previous levels of sport participation, they scored a mean VAS of 7.71 ± 3.11 (range, 0-10). Finally, when asked their confidence that their knees would not give way by playing their sports, they scored a mean VAS of 8.1 ± 2.76 (range, 0-10).
Results of Return to Play and Patient Satisfaction
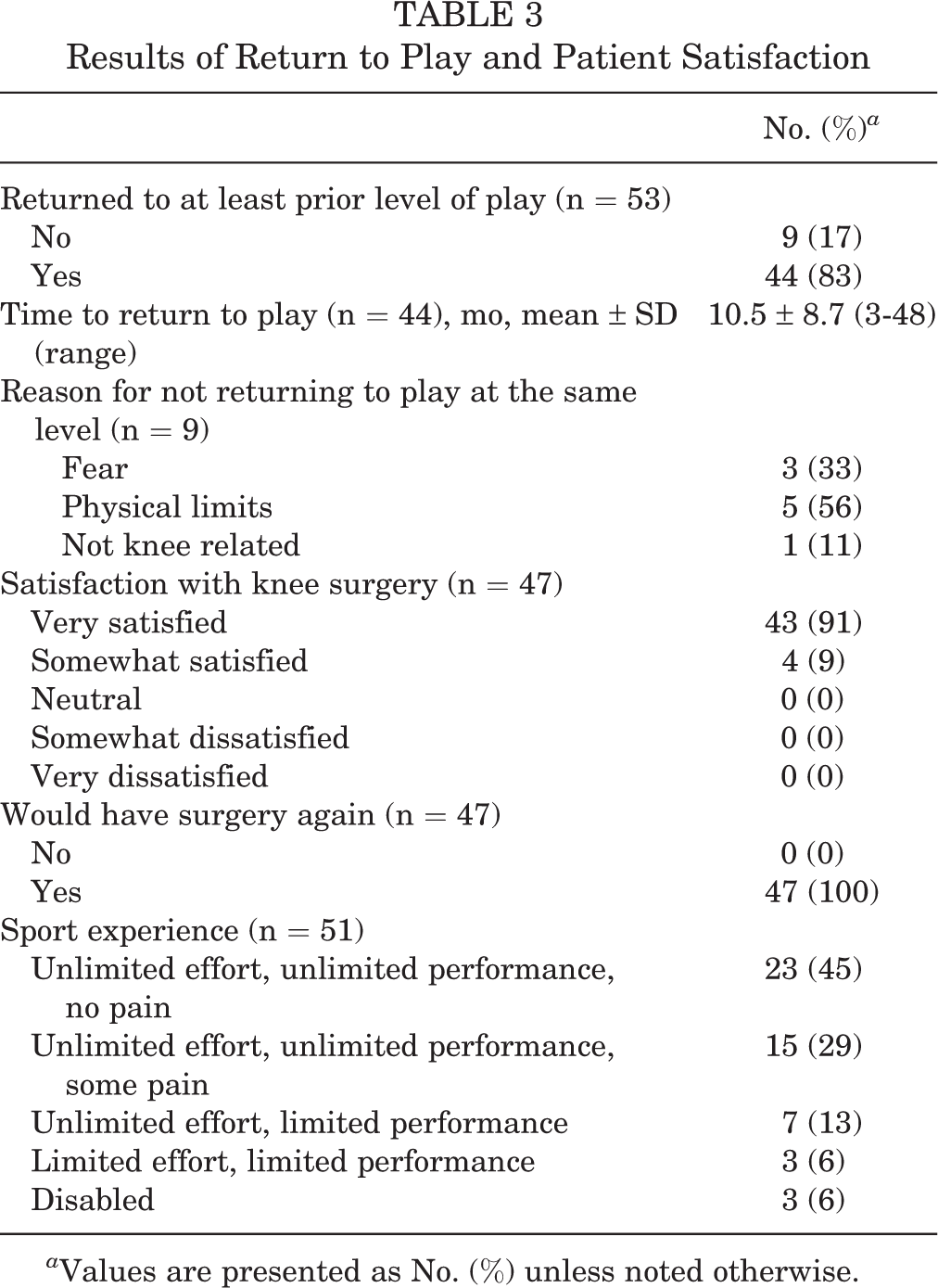
a Values are presented as No. (%) unless noted otherwise.
There were 14 subsequent ACL tears in 13 patients (25%). There were 4 ipsilateral ACL graft tears (7.5%) and 10 contralateral ACL tears (19%). One patient sustained subsequent bilateral ACL injuries to the reconstructed knee and the contralateral, previously nonoperated, knee. Mean time to subsequent ipsilateral ACL injury was 15 ± 11 months (range, 8-28 months). Mean time to contralateral ACL injury was 27 ± 8.7 months (range, 17-41 months) (Table 4). The patient who sustained subsequent bilateral ACL tears first tore the contralateral ACL 28 months after the index operation and then his ipsilateral ACL graft 40 months after the index operation. Three of the 4 ipsilateral reinjuries were in female athletes. Of the 10 subsequent contralateral ACL injuries, 9 were in females. The overall incidence of subsequent ipsilateral or contralateral ACL injuries in our cohort was 29% for female patients (n = 11) and 13% for male patients (n = 2). Of the patients with recurvatum at the time of ACLR, none sustained an ipsilateral ACL reinjury, and 1 had a subsequent contralateral ACL tear.
Subsequent ACL Tears a
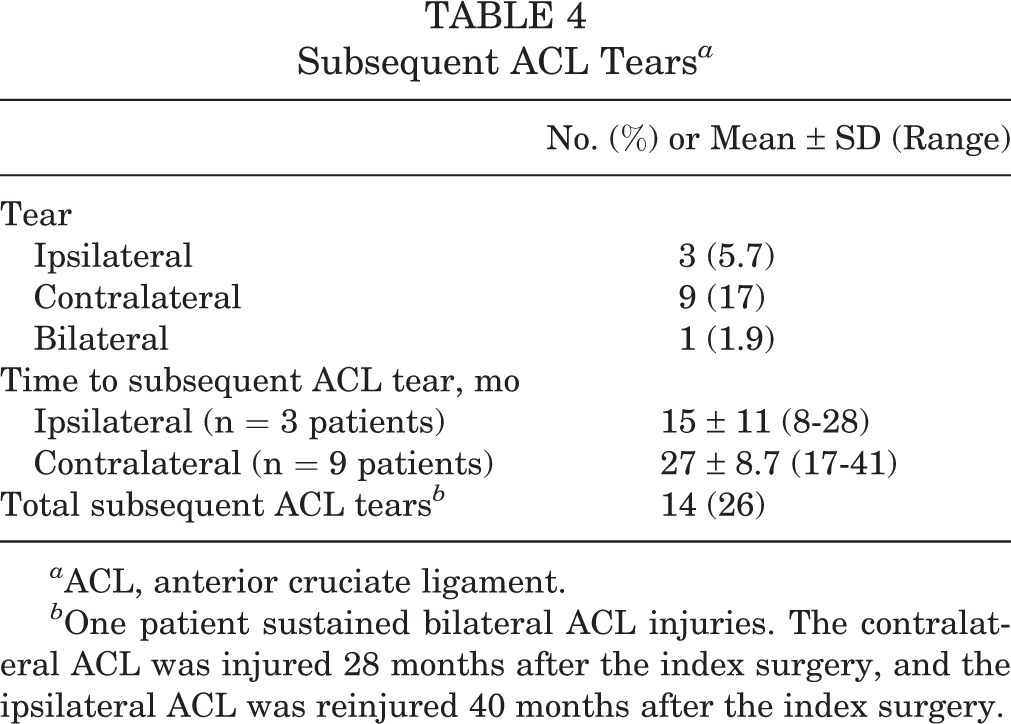
a ACL, anterior cruciate ligament.
b One patient sustained bilateral ACL injuries. The contralateral ACL was injured 28 months after the index surgery, and the ipsilateral ACL was reinjured 40 months after the index surgery.
An analysis of sport-specific measures (Table 5) revealed that all football players in our cohort were able to RTS (6/6 players; 100%) at a mean 8 ± 2 months (range, 5-10 months) without any subsequent ACL injuries. Lacrosse players had an RTS rate of 91% (10/11 players) at a mean 9.7 ± 7.7 months (range, 4.5-29 months) with 2 (18%) of these patients experiencing subsequent ipsilateral ACL tears and another 2 (18%) contralateral ACL tears. Of the basketball players, 83% (5/6 patients) returned to sport at a mean 6.8 ± 0.84 months (range, 6-8 months), with 3 patients (50%) experiencing contralateral ACL tears and no patients having a subsequent ipsilateral ACL injury. Among skiers, 75% were able to RTS (3/4 patients) at a mean 7 ± 1.5 months (range, 6-9 months) with 1 patient (25%) having an ipsilateral ACL tear. Finally, soccer players returned to sport at a rate of 77% (20/26 patients) at a mean 13 ± 12 months (range, 4.5-48 months) with 1 patient (4%) experiencing subsequent bilateral ACL tears and 4 (15%) having a subsequent isolated contralateral ACL tear.
Sport-Specific General Characteristics a

a Data are reported as No. (%) unless otherwise indicated. ACL, anterior cruciate ligament.
b One soccer player sustained subsequent bilateral ACL tears.
Examining RTS by sex demonstrated that 13 of 15 males (87%) returned to at least their prior levels of play. Of 38 females, 31 (82%) returned to at least their prior levels of play. Of 7 males, 6 (86%) returned to play soccer at their prior levels or higher, as compared with 14 of 19 female soccer players (74%).
Uni- and Multivariate Analysis
Univariate analysis was performed for age, BMI, sex, sport (soccer vs nonsoccer), mechanism of injury, meniscal tear, and the 3 confidence questions. There was no association between age, BMI, sex, sport, mechanism of injury, or meniscal tear and RTS. However, increased confidence for each confidence question was associated with RTS. On multivariate analysis, only increasing confidence that one can perform well at one’s sport was correlated with RTS (P = .02) (Table 6).
Logistic Regression Results of Probability of Returning to Sport at the Same Level a

a Bold P values indicate statistical significance (P < .05). aOR, adjusted odds ratio; OR, odds ratio.
Discussion
In this study, we found high rates of RTS and patient satisfaction for competitive high school–aged athletes after ACLR with BTB autograft. Patients reporting higher subjective confidence levels in their reconstructed knees were more likely to RTS. The overall ipsilateral retear rate was 7.5%.
The majority of patients (83%) returned to sport at their previous levels, which is consistent with or higher than most rates in the literature. The mean time for RTS was 10.4 months. Despite a high rate of return to the previous level of sport, only 45% of patients were able to play their sports with unlimited effort, unlimited performance, and no pain. This information is useful when counseling competitive high school–aged athletes undergoing BTB autograft ACLR. The MOON group analyzed RTS in a cohort of high school football players who underwent ACLR with BTB or hamstring autograft and found that just 45% were able to return to their prior levels of sport. 23 Dekker et al 9 reported the results of 112 patients <18 years old undergoing ACLR using autograft with a variety of techniques. The patients in their study had an age range of 6 to 17 years, and 84% returned to the same sport; however, the level of RTS was not noted. A 2014 systematic review and meta-analysis by Ardern et al 4 analyzed 69 studies of 7556 participants with a mean age of 25.8 years and found that 55% of patients undergoing ACLR returned to their prior competitive levels. The authors also noted that BTB autograft slightly favored return to preinjury level of sport. 4 Nwachukwu et al 24 cited an 87% rate of return to play among patients with a mean age of 26.7 years at the time of surgery. The authors noted that use of BTB autograft was associated with an increased likelihood of returning to play.
Another consideration is the time to return to play and its effect on returning to prior level of sport and subsequent ACL injury. Dekker et al 9 demonstrated earlier RTS as a risk factor for a second ACL injury in a cohort of patients <18 years old. Our time of return to play (mean, 10.4 months) is consistent with other studies. 7,9 Historically, there was a movement toward accelerated rehabilitation and earlier return to play, but this was based largely on lower-level evidence. DeFrancesco et al 8 proposed that enhanced rehabilitation, which includes additional neuromuscular training, advanced testing, and follow-up physician visits as compared with standard rehabilitation, is cost-effective based on a reduction in subsequent ACL injuries. To date, the optimal method of determining an athlete’s readiness to RTS is unknown and should be based on a patient’s physical function and the biologic factors that affect graft healing.
An additional important finding from our study is the high levels of patient satisfaction. There is increasing interest in determining patient satisfaction after elective orthopaedic procedures, but it is still an underreported outcome after ACLR. To our knowledge, our investigation is the first to report on RTS and satisfaction levels related to competitive high school–aged athletes after ACLR using the same graft choice in all patients (BTB autograft).
While rates of ACL injuries in younger populations are on the rise, rates of reinjury after ACLR have been shown to be higher in younger patients than in adults. In a cohort study of the Danish registry, there was a significantly increased risk of ipsilateral revision ACLR in patients aged 13 to 15 years (6.7%) and 15 to 20 years (4.9%) as compared with those aged >20 years (2.0%). 15 Dekker et al 9 cited a 32% incidence of secondary ACL injuries in a cohort of patients <18 years old who underwent ACLR. The investigators noted a 19% rate of ipsilateral ACL graft failure, a 13% rate of contralateral ACL injury, and a 1% rate of bilateral ACL injury. 9 Notably, 73% of the ACLRs in their cohort were performed with hamstring autograft. In our cohort of competitive high school–aged athletes, 13 patients (25%) sustained subsequent ACL injuries, with 9 (17%) occurring in the contralateral knee, 3 (5.7%) in the ipsilateral knee, and 1 (2%) in both knees (subsequent bilateral ACL tears).
There is a high rate of contralateral ACL injuries in our cohort (19%). A systematic review and meta-analysis of 2026 patients (mean age, 23.4 years; 67% male) cited rates of contralateral ACL injuries from 8.2% to 16% at 5-year follow-up. 32 However, when examining a cohort similar to ours, we find comparable contralateral injury rates. Paterno et al 26 studied rates of subsequent ipsilateral and contralateral ACL injuries in a predominately female cohort (75% female) with a mean age of 17 years. They noted that 20.5% of patients sustained a contralateral ACL injury and 9.0% incurred a retear of the ipsilateral graft within 2 years. 26 Additionally, our rate of contralateral injury could appear higher than stated given the limited number of patients. Regardless, contralateral injuries are important to consider when determining the time to return to play for a high-level high school–aged athlete.
Another potential risk factor for subsequent ipsilateral or contralateral injury is female sex. The incidence of subsequent ipsilateral or contralateral ACL injuries in our cohort was 29% for female patients (n = 11) and 13% for male patients (n = 2). While multiple studies have shown female sex to be a risk factor for a native ACL injury, it has not been demonstrated to be a risk factor for ipsilateral reinjury or contralateral ACL injury. 2,17,27,28 Several studies have indicated higher absolute risk for contralateral ACL injuries in female patients, but it does not reach statistical significance. 28,33
In addition to young age, our cohort comprised patients with the highest possible Marx activity scores, and a previous study demonstrated that increasing Marx scores raised the risk of subsequent ipsilateral and contralateral ACL injury after ACLR. 17 These patients are at a high risk of reinjury, and the ipsilateral retear rate is 7.5% using BTB autograft in this patient population.
Notably, our investigation found correlation between an athlete’s confidence in the reconstructed knee and the rate of RTS. Of the 9 patients who were unable to RTS, 33% (3 patients) cited fear as a reason. A recent systematic review noted that the fear of reinjury was the most common impediment to return to play. 25 Furthermore, investigations by Ardern et al 3,5,6 revealed that psychological readiness to RTS and recreational activity are strongly associated with rates of return. Those investigators have advocated for interventions aimed at addressing psychological recovery during postoperative recovery. Our investigation validates the implication of psychological factors in RTS rates and provides support for further research into these interventions.
The strengths of this study are that it provides outcomes after ACLR in a relatively homogeneous patient population using 1 graft type. Additionally, by including patients from 14 surgeons, the generalizability of the findings is higher. The results of this study are helpful when counseling this subset of patients who are at high risk of ACL injury and reinjury. Limitations of this investigation include the lack of a comparison or control group, such as recreational athletes, or comparisons of differing graft choice. Additionally, the postoperative survey was similar to those conducted in previous studies 23,24 ; however, it is not a validated tool for assessing RTS or satisfaction after ACLR. Our cohort consisted of patients whose inclusion as a competitive athlete was defined per the self-reported activity level, which has the potential for misclassification. In addition to the benefit of raising the generalizability of our findings, the limitation of including 53 patients from 14 surgeons can be the differences in surgical technique or postoperative rehabilitation protocols, which increases the heterogeneity of our study. A potential limitation specific to an investigation of high school athletes is that our RTS rates may be underestimating true values, as patients who aged out of high school but did not compete at the college level were considered unable to RTS at the same level. Additionally, the rate of contralateral ACL injuries may be higher than the true injury rate, as a result of the small sample size and higher likelihood of patients following up if they have subsequent injuries. An additional limitation of our study is the 37% follow-up rate. The demographics, mechanism of injury, and presence of meniscal pathology were similar between the groups with and without follow-up, but the patients were more likely to be female, have a lower baseline IKDC score, and play soccer as their primary sport.
Conclusion
Competitive high school athletes treated with BTB autograft ACLR reported high rates of RTS, high satisfaction, and a retear rate of 7.5%. The contralateral ACL injury rate was 19%, indicating that further evaluation must be performed when assessing these high-risk athletes and their readiness to RTS. Confidence levels were correlated with RTS rates in uni- and multivariate analyses. Our results support the use of BTB autograft for ACLR in competitive high school–aged athletes.
Footnotes
HSS ACL REGISTRY GROUP
Andrew Pearle, MD; Answorth Allen, MD; Beth Shubin Stein, MD; David Dines, MD; Anil Ranawat, MD; Anne Kelly, MD; Bryan Kelly, MD; Howard Rose, MD; Michael Maynard, MD; Sabrina Strickland, MD; Struan Coleman, MD; Jo Hannafin, MD, PhD; John MacGillivray, MD; Robert Marx, MD; Russell Warren, MD; Scott Rodeo, MD; Stephen Fealy, MD; Stephen O’Brien, MD; and Thomas Wickiewicz, MD (Department of Orthopedic Surgery, Hospital for Special Surgery, New York, New York, USA).
Final revision submitted December 5, 2020; accepted January 12, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.U.N. has received grants and education payments from Arthrex; education payments from Smith & Nephew; hospitality payments from Stryker, Wright Medical, and Zimmer Biomet Holdings; and royalties from Remote Health. R.J.W. has received research support from Histogenics; consulting fees from Arthrex, JRF Ortho, and Lipogems; royalties from Arthrex; and hospitality payments from Stryker. R.J.W. also has stock or stock options in BICMD, Cymedica, Engage Surgical, Gramercy Extremity Orthopedics, Pristine Surgical, and RecoverX. J.S.D. has received research support and nonconsulting fees from Arthrex; consulting fees from Arthrex, Linvatec, Merck Sharp & Dohme, Trice Medical, and Wright Medical; and royalties from Linvatec, Thieme, and Wolters Kluwer Health–Lippincott Williams & Wilkins. D.W.A. has received consulting fees from Stryker Corp and hospitality payments from Arthrex. A.P. has received education payments from Arthrex; consulting fees from Exactech, Zimmer Biomet, and Stryker; nonconsulting fees from Smith & Nephew; and royalties Zimmer Biomet. A.A. has received consulting fees from Arthrex. D.D. has received consulting fees and royalties from Zimmer Biomet. A.R. has received nonconsulting fees from Arthrex and Smith & Nephew; education payments from Arthrex; consulting fees from Arthrex, Smith & Nephew, Stryker, and Flexion; and royalties from ConforMIS. A.K. has received education payments from Arthrex. B.K. has received consulting fees, nonconsulting fees, and royalties from Arthrex and faculty/speaker fees from Synthes GmbH. M.M. has received education payments from Arthrex. S.S. has received consulting fees from Flexion Therapeutics, Vericel, DePuy, and Pfizer and honoraria from Vericel and JRF Ortho. J.H. has received hospitality payments from Smith & Nephew. S.C. has received consulting fees and royalties from Stryker Corp, nonconsulting fees from Smith & Nephew, and education payments from Pinnacle. R.W. has received royalties from Arthrex and Zimmer Biomet and nonconsulting fees from Arthrex. S.R. has received consulting fees from Flexion Therapeutics, nonconsulting fees from Smith & Nephew, honoraria from Fidia Pharma, and royalties from Zimmer Biomet and is a paid associate editor for The American Journal of Sports Medicine. S.F. has received royalty payments from Encore. T.W. has royalty payments from Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Hospital of Special Surgery (study No. 2018-1565).