
Abstract
Background:
Residual posterior sagging may occur after posterior cruciate ligament (PCL) reconstruction (PCLR), yet when it mainly occurs is not fully understood.
Purpose:
To elucidate sequential changes in radiographic posterior tibial translation (PTT) after PCLR.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
The authors retrospectively investigated the radiographic findings from 22 patients who underwent bisocket double-bundle PCLR for isolated PCL injury with at least 2 years of follow-up (mean, 4.5 years; range, 2-10 years). Injury severity was assessed using PTT on lateral radiographs with gravity sag views and was stratified according to side-to-side difference in the tibial-femoral stepoff: grade 1 (<5 mm), grade 2 (5 to <10 mm), or grade 3 (≥10 mm). Measurements were taken preoperatively and then immediately, 3 months, 6 months, 1 year, and ≥2 years postoperatively. The authors also investigated the risk factors for residual posterior sagging, indicated when PTT was ≥5 mm (grade ≥2) at the minimum 2-year follow-up.
Results:
Preoperatively, 13 patients had a grade 2 injury, and 9 had grade 3 injury. The PTT, restored immediately after PCLR, significantly increased at 3 months (P < .001) but remained unchanged thereafter ≥2 years. There were 7 cases of postoperative PTT ≥5 mm on radiographs. Patients with residual posterior sagging had significantly larger mean PTT than did those without residual posterior sagging at all time points except for immediately postoperatively (preoperatively, 9.1 ± 1.6 vs 12.2 ± 2.3 mm; 3-month follow-up, 2.7 ± 1.6 vs 7.0 ± 1.8 mm; ≥2-year follow-up, 3.4 ± 1.0 vs 6.5 ± 1.4 mm; P < .001 for all). Multivariate logistic regression analysis showed that preoperative grade 3 injury was independently associated with residual posterior sagging (OR, 26.809; 95% CI, 1.257-571.963; P < .001).
Conclusion:
The initially reduced postoperative PTT significantly increased within 3 months using conventional rehabilitation protocols, but no progression was observed up to 4.5 years after PCLR. Preoperative grade 3 injury was independently associated with residual posterior sagging.
Keywords
Posterior cruciate ligament (PCL) reconstruction (PCLR) is performed to improve subjective knee instability and restore normal knee laxity. Time-zero biomechanical studies have demonstrated that some PCLR techniques successfully restore the normal kinematics of the knee joint, 7,22,46 but clinical studies have reported that the postoperative recurrence of posterior laxity or posterior tibial translation (PTT) is common. 1,47 An abnormal posterior tibial position caused by PCL injury can increase the contact pressure in the medial tibiofemoral compartment 42 and patellofemoral compartment 43 and raise the risk of osteoarthritis in the future. 39,45 However, at what time point the PTT recurs postoperatively and what factors significantly contribute to the recurrence of PTT have not been fully elucidated. The current study therefore aimed to investigate sequential changes in the radiographic PTT through PCLR and analyze the risk factors that influence the onset of postoperative residual posterior sagging. It was hypothesized that the PTT would recur in the early postoperative period but not proceed thereafter and that some risk factors, such as a smaller posterior tibial slope, 11,12 could affect the postoperative residual PTT.
Methods
This retrospective study protocol was approved by our institutional review board. Between January 2007 and December 2016, 49 patients who underwent PCLR for isolated unilateral PCL injury were included in this study. All study participants had experienced persistent posterior instability or pain during daily or sporting activities despite receiving >3 months of nonoperative treatment including quadriceps exercise without bracing by physical therapists and/or use of nonsteroidal anti-inflammatory drugs at our institution or another clinic. Informed consent was performed with all the patients.
Of the 49 patients, 27 were excluded for the following reasons: lost to follow-up (n = 6), additional surgery such as hardware removal with second-look arthroscopy (mean, 10 months postoperatively; range, 6-15 months) (n = 12), and did not agree to further outpatient follow-up after the expiration of liability insurance and workers’ compensation insurance around 1 year (n = 9). Thus, 22 patients (18 men and 4 women) who were available for postoperative radiographic evaluation for at least 2 years after their operation (mean, 4.5 years; range, 2-10 years) were evaluated. The mean patient age at the time of surgery was 41 years (range, 20-64 years), and the reasons for surgery included sports-related injuries (n = 5), work-related injuries (n = 2), and traffic accidents (n = 15).
PCL injury grade was assessed using PTT, stratifying the side-to-side difference of the tibial-femoral stepoff as grade 1 (<5 mm), grade 2 (5 to <10 mm), and grade 3 (≥10 mm). 3 Isolated PCL injury was diagnosed based on negative findings after Lachman, varus, valgus, and dial tests and the absence of concomitant ligamentous injuries (posterolateral/posteromedial [PM] corner injuries) on magnetic resonance imaging scans. Thirteen patients had grade 2 PCL injury (≥5 to <10 mm PTT), and 9 had grade 3 PCL injury (≥10-mm PTT). Patient characteristics and preoperative and interoperative characteristics are presented in Table 1.
Patient Characteristics (N = 22) a

a Data are reported as n or mean ± SD (range). AL, anterolateral; BMI, body mass index; CSA, cross-sectional area; LFC, lateral femoral condyle; LTP, lateral tibial plateau; MFC, medial femoral condyle; MTP, medial tibial plateau; NA, not available; PCL, posterior cruciate ligament; PM, posteromedial; PTT, posterior tibial translation.
b Based on the grading system of Shino et al, 38 where 0 = normal; 1 = superficial fibrillation or surface flaking; 2 = fissuring or fibrillation less than one-half the thickness of the articular cartilage; 3 = fasciculation, fragmentation, or degeneration greater than one-half the thickness of the articular cartilage; and 4 = erosion to subchondral bone.
Surgical Techniques
All surgical procedures were performed by 2 orthopaedic surgeons (S.H. and Y. Tanaka) at the same institution. All patients were subjected to bisocket double-bundle PCLR in this study. Each patient was placed in a supine position, and an arthroscopic diagnosis was made via standard anteromedial and anterolateral (AL) portals. For femoral tunnel creation, we cleared the soft tissue, including the remnants of the torn PCL, using a mechanical shaver and visualized the anatomic landmarks for the PCL femoral footprint. 8 Two 2.4-mm k-wires were separately inserted into the center of the AL and PM bundles of the PCL footprints in an inside-out manner with the knee flexed to 100° to 110°. Matching the graft diameter, two 15- to 20-mm sockets were created by overdrilling the k-wires, with diameters of 6.5 to 8.0 mm for the AL tunnel and 5.0 to 6.5 mm for the PM tunnel, respectively.
For tibial tunnel creation, we again cleared the remnants of the torn PCL using a mechanical shaver through the PM portal and clearly visualized the anatomic landmarks for the PCL tibial footprint. 2 Viewing through the PM portal, two 2.4-mm k-wires were inserted using an outside-in manner from the medial tibial cortex to the center of footprint using a tibial tip aimer (Smith & Nephew Endoscopy). After checking the location of the tips of k-wires on frontal/lateral radiographs, the k-wires were overdrilled using a 7.0- to 11.0-mm drill, matching the graft diameter.
The autogenous semitendinosus and gracilis tendons were harvested and made into tripled grafts 80 to 85 mm in length. The semitendinosus tendon was used for the AL graft, and the gracilis tendon was used for the PM graft. Both ends of the grafts were unified and sutured using 2 No. 2 polyethylene sutures (Arthrex). After the passage of the grafts, 2 Endobuttons (Smith & Nephew Endoscopy) were set on the cortex of the medial femoral condyle and unified using sutures. Subsequently, the graft sutures for the tibial side were connected using 2 Double-Spike Plates (MEIRA Corp), and the creep of the construct was removed through repetitive manual pulling. Finally, these grafts were fixed to the tibia under a total initial tension of 10 N (5 N for the AL graft and 5 N for the PM graft) with the knee in 0° of flexion. 21 The graft tensions were applied and monitored by tensioners via the tensioning sutures, distally connected to Double-Spike Plates.
Postoperative Rehabilitation
For postoperative management, knees were immobilized in extension via braces for 3 weeks to reduce the acute inflammatory response such as pain and swelling and to protect the tendon-bone healing in the early postoperative term. 32 Conventional protocols such as range of motion exercises and partial weightbearing without a functional PCL brace were started at 3 weeks postoperatively, and full weightbearing began at 5 weeks postoperatively. Jogging and running were respectively allowed at 4 and 7 months postoperatively. Patients were allowed to return to their previous activity levels around 10 months postoperatively.
Radiographic Measurement
For the evaluation of PTT, lateral radiographs with gravity sag views 37 were collected. The patients were placed in a supine position along a long axis of the table with both hips flexed to 45° and both knees kept upright at 90° of flexion and were instructed to relax their muscles while the radiographs were obtained. First, the posterior tibial axis was defined as a line parallel to the posterior cortex that had started passing through a point 15 cm from the joint line on the posterior cortex. 19 Second, the tibial line was defined as a line parallel to the posterior tibial axis and across the anterior border of the tibial plateau, whereas the femoral line was defined as a line parallel to the posterior tibial axis and across the middle point between the distal borders of the lateral and medial condyles. The tibial-femoral stepoff was measured as the interval between the tibial and femoral lines. Then, the PTT was defined as the side-to-side difference of the tibial-femoral stepoff (Figure 1). The plain radiographs were taken bilaterally to adjust the tibial rotation and knee flexion angles, which potentially affected the tibial-femoral stepoff value. Immediately postoperatively (intraoperatively, just after graft fixation), only the plain radiograph of the affected side was obtained, and the PTT was calculated by comparing the tibial-femoral stepoff with that of the contralateral intact side at the preoperative time point. The PTT was sequentially evaluated preoperatively and then immediately, 3 and 6 months, and 1 and ≥2 years (final follow-up) postoperatively.

Evaluation of the gravity sag view of lateral radiographs. The side-to-side difference of the tibial-femoral stepoff, which was the interval between the tibial and femoral lines, was defined as the posterior tibial translation. FL, femoral line; PTA, posterior tibial axis; TL, tibial line.
In addition, the posterior tibial slope was measured according to a previously validated method. 5,41 First, 4 points were marked at 5 and 15 cm distal to the joint line on the anterior and posterior tibial cortices. Second, 2 midpoints were marked at 5 and 15 cm. Then, a proximal tibial anatomic axis was drawn to intersect both midpoints. The degree of the posterior slope was then measured as the angle derived from the posterior inclination of the medial and lateral tibial plateaus, and a perpendicular line was subsequently drawn with respect to the proximal tibial anatomic axis. The slopes of the medial and lateral tibial plateaus were averaged to produce a final calculated tibial slope value. PTT ≥5 mm (grade ≥2) at the minimum 2-year follow-up was radiographically regarded as residual posterior sagging.
The intraobserver intraclass correlation coefficient (ICC) of the PTT has been assessed previously. 40 For the assessment of intraobserver reliability in this study, a single orthopaedic surgeon (Y. Tachibana) measured the PTT in all patients 3 times, with an interval of 14 days between measurements, by considering all lateral plain radiographs at all time points; ultimately, the intraobserver ICC of the PTT was 0.975. For the assessment of interobserver reliability, 2 other orthopaedic surgeons (Y. Tanaka and K.K.) independently measured the PTT on each lateral radiograph of each studied patient at each time point; here, the interobserver ICC was 0.874. For the calculation of both the intra- and interobserver ICCs, the examiners repetitively measured the PTT on the same images on separate occasions to decrease the patient’s radiation exposure.
Statistical Analysis
All statistical analyses were conducted using the JMP software (JMP Pro Version 15.1.0; SAS Institute). Power analysis indicated that a sample size of 11 participants was required for valid comparisons (power, 0.8; α = .05; detectable change in the mean PTT from immediately postoperative time point to 3-month postoperative time point, 5.2 ± 2.6 mm). Potential risk factors included sex, age, interval from injury to surgery, body mass index (BMI), meniscal injury, severe chondral damage greater than grade 3, 14 posterior tibial slope, femoral AL/PM tunnel diameter, tibial tunnel diameter, total cross-sectional area of the PCL graft, and preoperative injury grade. The null hypothesis of normal distribution of the data obtained in this study (ie, the PTT at ≥2 years postoperatively in the 2 patient groups with and without residual posterior sagging) was tested and denied by the Shapiro-Wilk test (P = .079-.437). To compare patients with and those without residual posterior sagging, Fisher exact test was used for sex, chondral injury, meniscal injuries, and preoperative injury grade, while the independent t test was used for the other parameters. In addition, multivariate logistic regression analyses were used to identify significant risk factors and odds ratios (ORs) and 95% confidence intervals (CIs) were also calculated. Moreover, for the most predictive factor, receiver operating characteristic (ROC) curve analysis was performed to identify the optimal cutoff point for residual posterior sagging between subgroups. Statistical significance was indicated as P < .1 for the comparison of patient data between the groups and as P < .05 for all other comparisons.
Results
Sequential Changes in the PTT
The mean PTT was 10.1 ± 2.3 mm preoperatively and was reduced significantly to −0.8 ± 1.2 mm immediately after surgery (P < .001). Subsequently, the PTT was significantly increased by 4.9 ± 2.7 mm up to 4.1 ± 2.7 mm at 3 months postoperatively (P < .001). Then, no significant changes at 6 months (4.1 ± 2.5 mm), 1 year (4.4 ± 2.1 mm), and ≥2 years (4.4 ± 1.9 mm) postoperatively were observed. Significant improvement was seen at all time points compared with preoperative values (Figures 2 and 3).
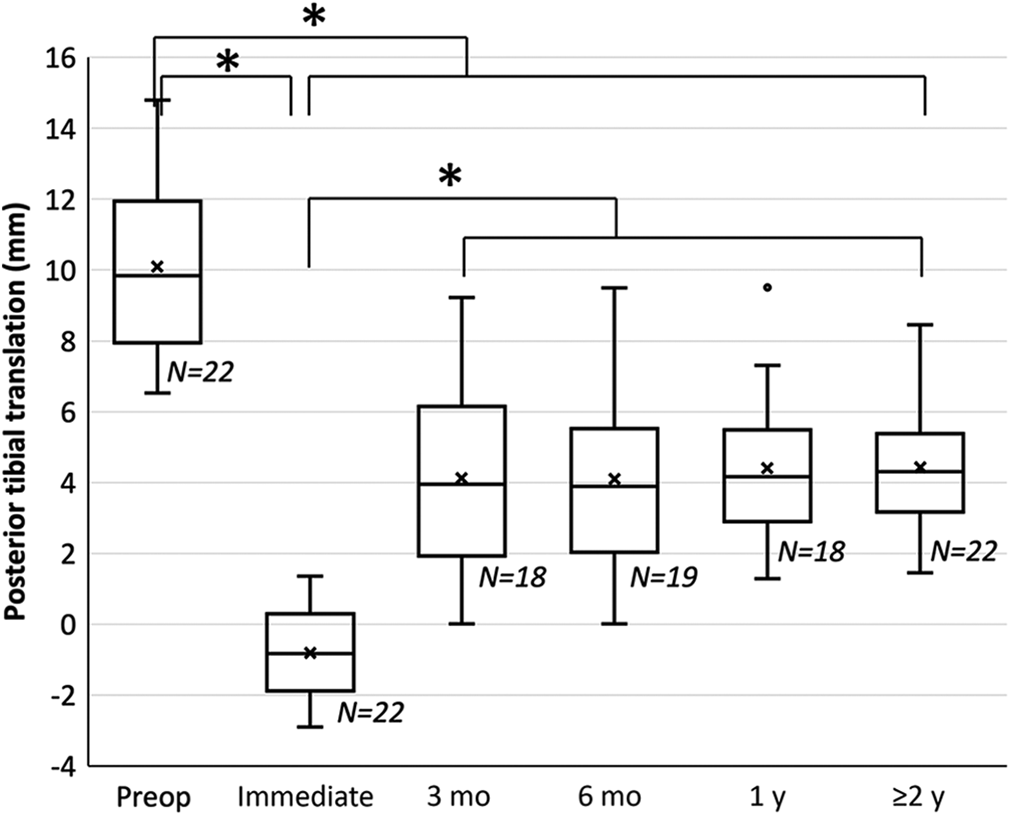
Sequential changes in posterior tibial translation before and after posterior cruciate ligament reconstruction. A positive value indicates that the tibia in the affected knee was posteriorly displaced compared with that in the contralateral healthy knee. *P < .05. Immediate, immediately postoperative; Preop, preoperative.

Sequential changes in lateral radiographs with gravity sag views: a representative case (a 42-year-old man injured in a traffic accident). Immediate, immediately postoperative; Preop, preoperative.
Residual Posterior Sagging
Seven cases of residual PTT with grade 2 injury at ≥2 years after PCLR were identified. No patient underwent revision PCLR because of subjective recurrent instability, and no instance of grade 3 injury persisted to the final follow-up. When comparing the patient data between the 2 groups, those with and those without residual posterior sagging, the preoperative PCL injury grade (preoperative PTT) was significantly larger in the patient group with residual PTT. BMI and femoral PM tunnel diameter also tended to be larger but did not reach significance (Table 2).
Comparison of Patient Data Between Those With and Those Without Residual Posterior Sagging a

a Data are reported as n, n (%), or mean ± SD (range) unless otherwise indicated. AL, anterolateral; BMI, body mass index; CSA, cross-sectional area; LM, lateral meniscus; MM, medial meniscus; PCL, posterior cruciate ligament; PM, posteromedial; PTT, posterior tibial translation.
b Fisher exact test was used for sex, meniscal injury, chondral injury, and preoperative grade, while the independent t test was used for other parameters.
c Statistically significant difference (P < .1).
d Statistically significant difference (P < .05).
The sequential change in PTT through PCLR was similar in both the group with and the group without residual posterior sagging. Preoperatively, the mean PTT was 12.2 ± 2.3 mm and 9.1 ± 1.6 mm among patients with and those without residual posterior sagging, respectively (P = .008). Furthermore, there was no significant difference between the 2 groups concerning the PTT immediately after PCLR (with vs without residual posterior sagging; −0.8 ± 0.8 vs −0.8 ± 1.3 mm; P = .948). At 3 months postoperatively, the PTT increased to 2.7 ± 1.6 mm in the group without residual posterior sagging but was 7.0 ± 1.8 mm in the group with residual posterior sagging (P < .001). Thereafter, no significant changes in either group occurred, and the PTT at ≥2 years was 3.4 ± 1.0 mm in the patients without residual posterior sagging and 6.5 ± 1.4 mm in those with residual posterior sagging (P < .001) (Figure 4). In sum, the PTT in patients with residual posterior sagging was significantly larger than that in patients without residual posterior sagging at all time points except for immediately postoperatively. In the multivariate logistic regression analysis, a preoperative grade 3 injury was independently associated with residual posterior sagging (OR, 26.809; 95% CI, 1.257-571.963; P = .0035) (Table 3). Meanwhile, the ROC analysis highlighted a cutoff value of 12.64 mm for the preoperative PTT as the optimal threshold for differentiating the 2 groups, those with and those without residual posterior sagging (sensitivity, 71.4%; specificity, 100.0%) (Figure 5).

Sequential comparison of the posterior tibial translation before and after posterior cruciate ligament reconstruction between the 2 patient groups with or without residual posterior sagging. Positive values indicate that the tibia in the affected knee was posteriorly displaced relative to that in the contralateral healthy knee. *Statistically significant difference between the 2 groups (P < .05). Immediate, immediately postoperative; Preop, preoperative.
Multivariate Logistic Regression Analysis of Risk Factors for Residual Posterior Sagging a

a Bolded text indicates statistical significance. BMI, body mass index; OR, odds ratio; PCL, posterior cruciate ligament; PM, posteromedial.

Receiver operating characteristic (ROC) curve of preoperative posterior tibial translation. The area under the ROC curve was 0.857 (P = .020; 95% CI, 0.458-0.975; SE, 0.115), and the cutoff point value was 12.64 mm (sensitivity, 0.714; specificity, 1.000).
Discussion
The major findings in the present study can be summed up as follows: (1) after PCLR, the initially reduced PTT significantly increased within 3 months postoperatively but did not progress thereafter to at least 2 years postoperatively; and (2) preoperative grade 3 injury was a significant independent risk factor for residual posterior sagging (OR, 26.809).
Adachi et al 1 serially measured the joint stability of 29 patients before and after PCLR (at 6, 12, 18, 24, and 42 months postoperatively) for isolated PCL injury using stress radiography and reported that an improvement in joint stability was observed at 6 months postoperatively and maintained for at least 2 years after PCLR, despite the posterior stability in the reconstructed knee not being identical to that in the contralateral normal knee. The serial changes in their study were compatible with our findings, but these authors did not evaluate the serial changes in the earlier postoperative term after PCLR. In the current study, the mean PTT significantly improved from 10.1 ± 2.3 mm (preoperatively) to −0.8 ± 1.2 mm (immediately after surgery), indicating that our PCLR procedure successfully reduced the tibia under a posterior drawer because of the gravity of the patient’s tibia. However, the PTT increased again at 3 months postoperatively, although it did not change thereafter for ≥2 years postoperatively, with a final value of 4.4 ± 1.9 mm (Figure 2).
The PCL graft is susceptible to high mechanical stress during postoperative rehabilitation, including the gravity of the patient’s shank weight, 37,47 knee flexion, or hamstring contraction. 18,28 Moreover, between the PCL graft and tunnel wall at the tunnel aperture, it is likely that high mechanical stress occurs on both the femoral side (the critical bending angle) 15,23 and the tibial side (killer turn). 26,27,29 These mechanical factors may facilitate larger graft elongation, tunnel enlargement, and consequently greater postoperative increases in the PTT in the early postoperative term. Meanwhile, no progressive incremental increase in the PTT was observed from 3 months to up to 4.5 years after PCLR in the current study. Bosch and Kasperczyk 6 investigated the healing of bone–patellar tendon–bone autografts after PCLR using a sheep model and found that the maximum load and stiffness of the graft gradually increased 8 weeks after surgery. That healing process of a transplanted graft in an animal model may support the absence of a further incremental increase in the PTT past 3 months after PCLR.
We divided patients into those with and those without residual posterior sagging and demonstrated that preoperative grade 3 PCL injury (≥10-mm PTT) was the most dominant risk factor. In the comparison of the sequential change between the 2 groups, the tibial position was restored immediately after PCLR regardless of the preoperative grade. However, interestingly, the PTT in patients with residual posterior sagging increased up to approximately 7 mm at 3 months postoperatively possibly because the PCL graft was loosened or stretched in the early postoperative period.
Some cadaveric studies have demonstrated that significant posterior laxity or a PTT of ≥10 mm could be combined with collateral ligamentous or capsular injuries. For the medial aspect of the knee joint, Ogata and McCarthy 30 demonstrated that additional cutting of the medial collateral ligament in the PCL-deficient knee significantly increased the PTT under a 30-N posterior drawer from 0° to 90°. Petersen et al 33 also reported that the posterior oblique ligament and PM capsule had a significant role in the prevention of additional PTT in the knee with PCL injury. For the lateral aspect of the knee joint, Sekiya et al 36 indicated that grade 3 PCL injury with a PTT >10 mm was correlated with the presence of a posterolateral corner injury and complete disruption of the PCL. Vogrin et al 44 showed that the in situ force of the PCL under a 134-N posterior tibial load was increased in the posterolateral corner–deficient condition. In this case series, all patients were treated as having isolated PCL injuries based on the negative findings of varus, valgus, and dial tests and lack of concomitant ligamentous injuries on magnetic resonance imaging scans. However, Pacheco et al 31 warned that a correct diagnosis of the posterolateral corner injury is made only 50% of the time at the point of referral to a specialist knee clinic, and magnetic resonance imaging correctly identified only approximately 25% of cases if the examination was performed >12 weeks after the injury. In this case series, the mean time from injury to surgery as well as the mean time from initial injury to preoperative magnetic resonance imaging was approximately 5 years. Thus, unaddressed or unrecognized disruption of secondary posterior restraints, including minor PM/posterolateral capsular injuries/stretching, 13,30,36 may have existed in our patients with large preoperative PTTs and, subsequently, residual posterior sagging. In addition, the patient group with residual posterior sagging tended to have a higher BMI without reaching significance. The characteristics of the gravity sag view, on which posterior tibial loads are generated by individual patients’ shank weights, potentially affected the current result. Thus, the patients with high body weights might be instructed to avoid range of motion exercises in a supine position and kneeling.
Some previous clinical studies have similarly investigated the PTT with gravity sag view before and after double-bundle PCLR using autogenous hamstring tendon grafts. Kimura et al 24 reported that the PTT was significantly reduced from 12.0 ± 1.7 mm preoperatively to 2.3 ± 1.8 mm at 2 years after surgery; in their study, both the AL and the PM grafts were fixed at 90° of knee flexion, applying a manual anterior tibial load, and a hard knee brace was worn for 6 months. Meanwhile, Deie et al 9 reported that the PTT was improved from 8 to 14.5 mm preoperatively to 2.6 mm at >10 years postoperatively. These patients also wore PCL braces for 6 months in the postoperative period. The mean 4.5-year postoperative PTT finding in the present study was 4.4 ± 1.9 mm, which appears inferior to the results of previous studies reporting a smaller PTT correction of approximately 6 mm, even if the PTT could be reduced immediately after PCLR. In the present study, conventional postoperative rehabilitation protocols such as range of motion exercises and partial weightbearing without a functional PCL brace were started at 3 weeks. However, a recent systematic review 35 recommended that range of motion exercises should be started in a passive prone position to prevent hamstring activation 18,28 and a dynamic anterior drawer brace 17,20,25 should be worn at all times for up to 6 months postoperatively. Given the increased PTT during the first 3 months, the results of the current study indicated that protective postoperative management for the transplanted PCL graft was warranted, especially in the early postoperative period, as follows: attending to instructions regarding daily activities, avoiding isolated hamstring contractions or kneeling, practicing controlled range of motion exercises, and using the functional PCL brace with a dynamic anterior drawer.
There remains controversy concerning the optimal knee flexion angle at the time of graft fixation. Here, both grafts were fixed at 0° of knee flexion with a small initial tension because the tibiofemoral relationship in the PCL-deficient knee was in a reduction position at 0°. 21 However, Harner et al 16 warned that the in situ force of the AL graft is highly elevated under a 134-N posterior drawer when fixed at knee extension. Kennedy et al 22 recommended that, to avoid excessive graft force, the PM graft should be fixed at 0° and the AL graft should be fixed at 90° of knee flexion. Accordingly, we plan to conduct a comparative study in the near future investigating the effect of these modifications for protecting the transplanted PCL graft on postoperative outcomes such as the PTT. In summary, the clinical relevance of the current study is that clinicians should take meticulous care, especially in the early postoperative period, to protect the transplanted PCL graft, such as by providing instruction for daily activities and prescribing functional PCL brace use although the PTT could be successfully reduced immediately after PCLR.
Contrary to the hypothesis, no significant correlation was detected between the posterior tibial slope and mean 4.5-year postoperative PTT result. Biomechanical studies have shown that a decrease in the posterior tibial slope can increase the PCL graft force 4 and the PTT in the PCL-deficient knee under a posterior drawer. 10,34 However, it is controversial in clinical settings; Bernhardson et al 5 demonstrated that the postoperative PTT was not influenced by a decreased posterior tibial slope after double-bundle PCLR at 18.5 months postoperatively. Conversely, in a single linear regression analysis after single-bundle PCLR, Gwinner et al 12 showed that the flattening of the posterior tibial slope was associated with a significantly greater persistent PTT at a longer follow-up point of 103 months, where sex and the number of operated ligaments were not considered. The mean posterior tibial slope in the current study was 6.8° ± 2.3° (range, 3.0°-13.0°) and was pretty much average compared with the previous data (from 5.9° to 8.0°). 5,12 This could indicate that only extreme flattening of the posterior tibial slope affected the PTT. However, future studies might be warranted to investigate the effect of the posterior tibial slope after double-bundle PCLR with a longer follow-up period.
Our study has several limitations. First, it evaluated only radiographic PTT because clinical outcomes scores, such as the Lysholm or Western Ontario and McMaster Universities Osteoarthritis Index score, were not fully available in several cases from the medical records. Second, the PTT was evaluated only in the gravity sag view without comparing a stress radiograph using a Telos device (Telos GmbH) 11,12 or with a kneeling technique 19 or comparing the posterior laxity with the KT knee arthrometer (MEDmetric) 1,48 ; notably, the posterior tibial load in the gravity sag view, generated by individual patients’ shank weights, could be smaller than those on stress radiographs. A higher BMI with a higher shank weight was also potentially associated with the nonsignificantly larger postoperative PTT. However, the gravity sag view is advantageous because the PTT immediately after PCLR can be safely evaluated without using any special stress device. Third, not all patients were available for 3-month, 6-month, and 1-year postoperative radiography. Fourth, postoperative magnetic resonance imaging scans were not obtained to assess the medial/lateral tibiofemoral relationship. Fifth, we investigated the PTT after only a bisocket PCLR procedure using autogenous hamstring tendon grafts, and the results might be different with other surgical techniques, graft materials, fixation methods, and so forth. Sixth, the small sample size might lead to type 2 error for some analyses.
Conclusion
The initially reduced postoperative PTT significantly increased within 3 months through conventional rehabilitation protocols, while no further progression was observed up to 4.5 years after PCLR. A preoperative grade 3 injury was independently associated with postoperative residual posterior sagging with a PTT ≥5 mm.
Footnotes
Final revision submitted November 26, 2020; accepted January 5, 2021.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Osaka Rosai Hospital.