
Abstract
Background:
Anterior cruciate ligament (ACL) rupture is one of the most common injuries afflicting soccer players and requires a lengthy recovery processes after reconstructive surgery. The impact of ACL reconstruction (ACLR) on return to play (RTP) time and player performance in professional soccer players remains poorly studied.
Purpose/Hypothesis:
To determine player performance and RTP rate and time after ACLR in elite professional soccer players with a retrospective matched-cohort analysis. We expected that the RTP time and rate will be similar to those of other professional-level athletes.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Included were 51 players from 1 of the 5 elite Union of European Football Associations (UEFA) soccer leagues who suffered a complete ACL rupture between 1999 and 2019. These athletes were matched by position, age, season of injury, seasons played, and height and compared to uninjured control players. Change in performance metrics for the 4 years after the season of injury were compared with metrics 1 season before injury. Univariate 2-group comparisons were performed using independent 2-group t tests; Wilcoxon rank-sum tests were used when normality of distributions was violated.
Results:
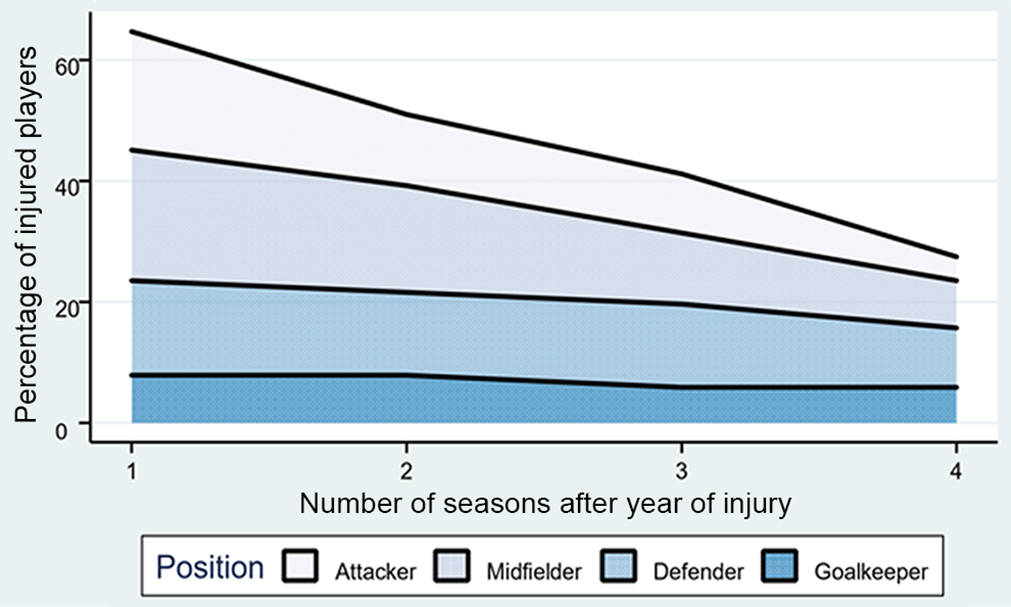
Overall, 41 players (80%) returned to play after ACL rupture, with 6 (12%) experiencing a subsequent ipsilateral or contralateral ACL tear. The mean (±SD) RTP time for soccer players after ACLR was 216 ± 109 days (26 ± 18 games). Injured athletes played significantly fewer games and minutes per season and recorded inferior performances for 2 seasons after their injury (P < .001). However, the game performance of injured players equaled or exceeded that of their matched controls by season 3 after injury, with the exception of attackers, who demonstrated a continued decline in performance (P < .001).
Conclusion:
Results indicated that the mean RTP time for soccer players after ACLR is short in comparison with other major sports leagues (216 days). However, RTP rates were high, and rerupture rates were comparable with those of other sports. With the exception of attackers, player performance largely equaled or exceeded that of matched controls by the third postinjury season.
Keywords
Soccer is the most popular sport in the world, with an estimated 270 million people, or 4% of the world’s population, currently playing. 9,11 Inherent to the sport is a high risk of injury to the anterior cruciate ligament (ACL). Most ACL tears in soccer players are noncontact in nature. 38 Soccer requires its players to make cutting movements combined with deceleration, land from a jump, and pivot on a knee in near full extension, which are all movements associated with ACL injuries. 1,16 ACL rupture is not only one of the most common injuries afflicting soccer players, but it also requires one of the longest recovery processes after reconstructive surgery. Consequently, ACL injuries result in long periods of lost play for athletes, as well as lost productivity and profitability for teams. 35
ACL reconstruction (ACLR) in the professional soccer athlete has been the subject of many recent investigations aimed at elucidating the time to return to play (RTP), rates of return to competitive play, factors associated with injury, and optimal surgical and rehabilitation protocols. 3,5,7,34,37,39,40 Several recent studies have emphasized time to RTP as well as RTP rates and have found time to RTP to be between 186 and 310 days, with excellent RTP rates in the range of 77% to 95%. 4,13,37,39 Furthermore, in a matched-cohort analysis of American soccer players, Erickson et al 13 found no difference in performance and survival in Major League Soccer (MLS) athletes after ACLR compared with controls. 13
However, the question that remains largely unanswered is whether the most elite soccer players return to the level of play and performance after ACL rupture that they had achieved before injury and, if so, on what timeline. Thus, the purpose of this matched-cohort analysis was to establish the time to RTP, RTP rates, and player performance after ACLR in high-level soccer players across the 5 elite Union of European Football Associations (UEFA) leagues, which are widely regarded as the top soccer leagues in the world (English Premier League, Bundesliga, Serie A, La Liga, Ligue 1). 35 We expected the RTP time and the rate of RTP to be similar to those of other professional-level athletes.
Methods
We conducted a retrospective matched-cohort study of male soccer players with a complete ACL rupture while playing on 1 of the 5 elite UEFA leagues between 1999 and 2019. All included players were identified using a publicly available database via methods established in previous investigations. 14,15,23,25,27 –31,33 Sources for injury reports included transfermarkt.co.uk, uefa.com, fifa.com, official team websites, injury reports, official team press releases, personal websites, and professional statistical websites. Injuries and player performance data were manually cross-referenced by 2 authors (E.M.F. and O.Z.L.-G.) via official league injury reports. The database utilized did not detail concomitant injuries.
A player was included in the injured cohort if he was drafted or signed to a team in the elite UEFA leagues, participated in at least 1 game before sustaining a complete ACL rupture, and had a minimum of 1-year follow-up after injury. Players were excluded if their ACL injury was unable to be identified as a complete rupture. Demographic data for each player including age, height, position, and number of seasons played were recorded. Injury and return to play data were documented including date of injury, days/games missed, date of return to play, and subsequent injuries as has been performed in previous investigations on professional soccer athletes. 4,7,13,37,39 Finally, performance metrics including games played, minutes played per game/season, goals scored, assists, shutouts, and conceded goals were collected.
A representative group of soccer players who had not sustained a complete ACL rupture was identified and matched to injured players in a 3:1 fashion (ie, 3 controls for each injury case) using the optimized matching methodology of King et al. 12,14,17,19,23,30,31 Players with any other lower extremity injury were excluded from the control group. Players were matched by position, height, ±2 years of age, ±1 season year, and ±1 year of seasons played within the league. 18,19 Further matching techniques (eg, minutes per season) compromised the number of available matches. A matched-cohort analysis was completed to compare performance metrics of injured players to their uninjured matched controls.
Change in performance metrics for 1, 2, and 3 years after the index year were compared with metrics 1 season before the index year. Injured players who did not RTP in 1 of 5 studied soccer leagues were excluded from performance analysis. Athletes who returned to play were only included in the performance analysis if they were actively participating in the mentioned leagues. Comparison of metrics with those of the previous year minimized the confounding effect of missed game time on season performance in the injured cohort. Performance changes at the various postinjury timepoints were compared between the injured and matched control group by position to account for the differing roles of player positions on the field. Injury history data were summarized as means ± SD. All other continuous data were summarized as median and interquartile range. Univariate 2-group comparisons were performed using independent 2-group t tests and Wilcoxon rank-sum tests when normality distributions were violated. Chi-square tests were used to compare categorical data. All analyses were performed using R Studio software Version 3.6.2 (R Foundation for Statistical Computing). Statistical significance was set at P < .05.
Results
Demographics and Return to Play
We identified 51 soccer players (mean age, 24.9 ± 4.1 years) who suffered a complete ACL rupture between 1999 and 2019. Demographic and return to sport characteristics for injured and uninjured controls are presented in Table 1. There were no significant differences in height, age, calendar year of season, or total years played in the league between the injured and uninjured control players (P > .05).
Cohort Characteristics a

a Data are reported as No. of players or mean ± SD. ACL, anterior cruciate ligament.
The percentage of injured players who returned to play is presented in Figure 1. Overall, 41 players (80%) returned to play in the elite UEFA leagues after ACLR. The majority (71%) of these players returned the year after their injury, with an additional 5% and 4% returning to play at 2 and 3 years after injury, respectively. Of the 51 players undergoing ACLR, 6 (12%) experienced a subsequent ipsilateral or contralateral ACL tear at some point in their career (Table 2).
Percentage of injured players who returned to play at least 1 game in the elite Union of European Football Associations leagues.
Return-to-Play Metrics for the Injured Players a

a Data are reported as mean ± SD or No. of players (%). ACL, anterior cruciate ligament.
Attackers
Nineteen attackers (37.3%; mean age, 25.9 ± 3.6 years) were identified as having suffered a complete ACL rupture. Unsurprisingly, injured attackers played fewer games, minutes, and minutes per game in the year of their injury compared with their matched controls (Table 3). The number of games and minutes played per season for the injured cohort remained significantly less until 3 years after the injury. By the 4-year time point, the injured cohort was playing significantly more games per season than their matched controls (P < .001). Interestingly, injured players continued to play fewer minutes per game than their controls all 4 years after their injury, though this difference was only statistically significant at the 1- and 2-year postinjury periods.
Attacker Metrics Compared With 1 Year Before Index Year a

a Data are reported as mean ± SD. Bolding indicates a statistically significant difference between groups. ACL, anterior cruciate ligament.
b Change in player performance metric as compared with 1 year before index year (ie, time of injury for players with complete ACL tear and index year for matched controls).
With respect to player performance, injured attackers scored significantly fewer goals 2 and 4 years after injury (P < .001), made significantly fewer assists 2 (P < .001) and 3 (P < .05) years after injury and accumulated significantly fewer points per game 2 years after injury (P < .001) compared with their matched controls. At 4 years after injury, injured players scored significantly fewer goals per season (P < .001), made a similar number of assists (P = .156), and scored more points per game (P < .05) than controls.
Midfielders
Midfielders accounted for 14 players (27.5%) suffering complete ACL rupture (mean age, 23.4 ± 4.1 years). Unlike injured attackers, midfielders played significantly more minutes (P < .05) but fewer games (P < .001) the season of their injury than their matched controls (Table 4). While injured midfielders played significantly less the year after their injury, this trend was reversed by their third and fourth postinjury year, when they played significantly more games (P < .001) and minutes (P < .05) than their matched controls.
Midfielder Metrics Compared With 1 Year Before Index Year a

a Data are reported as mean ± SD. Bolding indicates a statistically significant difference between groups. ACL, anterior cruciate ligament.
b Change in player performance metric as compared with 1 year before index year (ie, time of injury for players with a complete ACL tear and index year for matched controls).
Midfielders performed inferiorly with respect to goals 2 years after injury (P < .001), assists 1 year after injury (P < .001), and points per game 2 and 4 years after injury (P < .001, P < .05, respectively) compared with their matched controls. However, injured midfielders actually scored more goals and made more assists in the third and fourth postinjury season than matched controls. Interestingly, while injured midfielders scored similar points per game in the third year after injury, they scored fewer points per game in their fourth year after injury (P < .05).
Defenders
Sixteen defenders (31.4%) with a complete ACL rupture were identified (mean age, 24.4 ± 3.5 years). Like attackers, injured defenders played significantly fewer games (P < .001) and minutes (P < .05) during the season of their injury (Table 5). While injured defenders played fewer minutes per game than controls their season of injury, this difference was not significant (P = .976). Injured defenders continued to play significantly fewer games per season (P < .001), minutes per season (P < .05), and minutes per game (P < .05) for the 2 years after their injury. At 3 years after their injury, this difference was no longer significant, and at 4 years after injury, injured defenders played significantly more games (P < .001) and minutes (P < .05) than their matched controls.
Defender Metrics Compared With 1 Year Before Index Year a

a Data are reported as mean ± SD. Bolding indicates statistically significant difference between groups. ACL, anterior cruciate ligament.
b Change in player performance metric as compared with 1 year before index year (ie, time of injury for players with a complete ACL tear and index year for matched controls).
Performance metrics for injured defenders followed a similar timeline: these players performed inferiorly with respect to goals, assists, and points per game during the season of injury and the subsequent 2 seasons, with the exception of points per game, which was significantly greater in the injured cohort 2 years after injury. At 3 years after injury, injured defenders matched their controls in goals scored (P = .089) and points per game (P = .236). With respect to assists, injured players continued to make significantly fewer assists during their third postinjury year (P < .05) but matched their controls during their fourth postinjury season (P = .156).
Goalkeepers
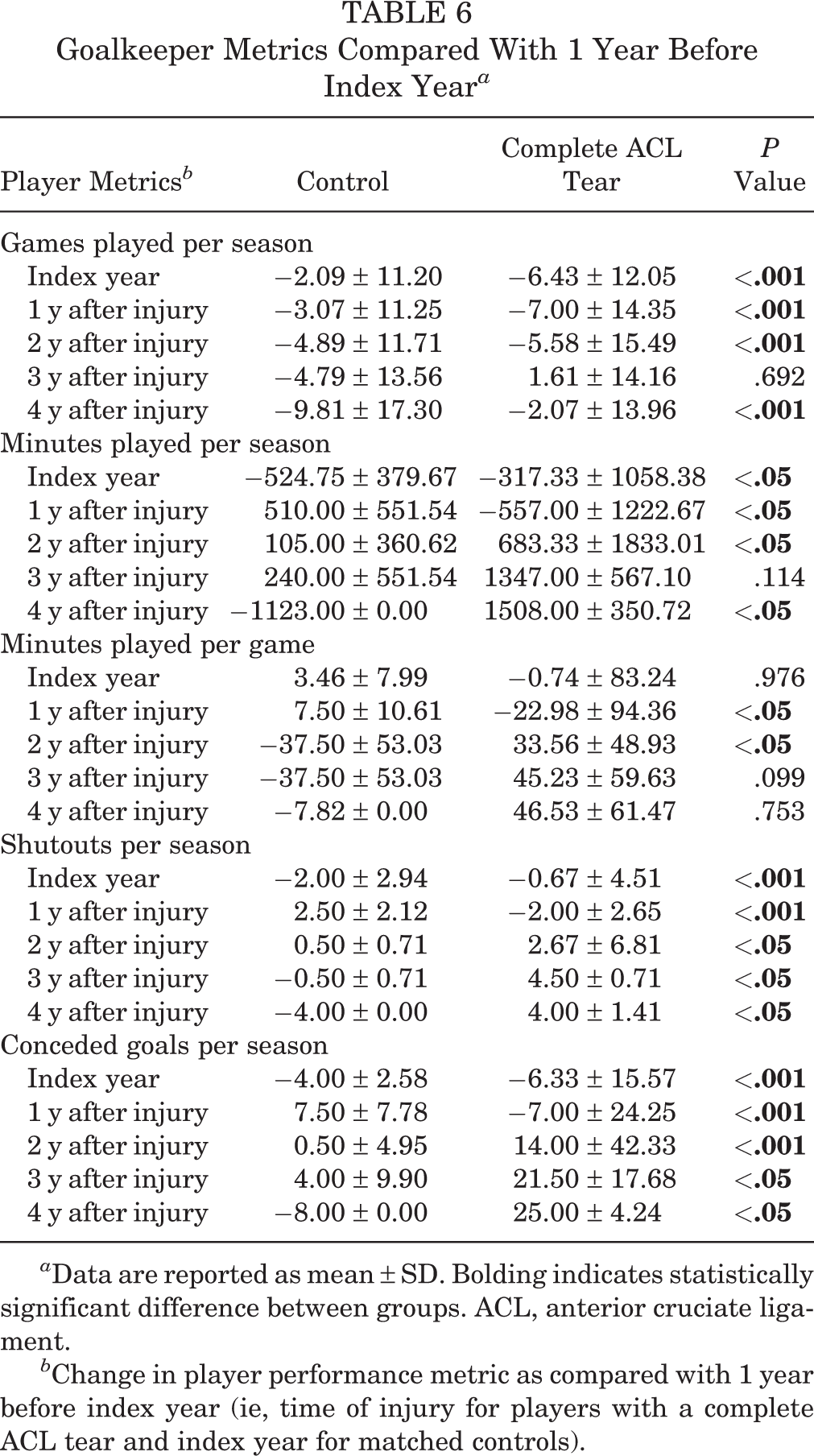
Five goalkeepers (9.8%; mean age, 27.2 ± 7.4 years) were identified as having a complete ACL rupture. Like injured midfielders, goalkeepers played significantly more minutes but fewer games the season of their injury than their matched controls (Table 6). However, at 3 years after their injury, injured goalkeepers matched their controls in games (P = .692) and minutes played (P = .114). In fact, injured goalkeepers played significantly more games (P < .001) and minutes (P < .05) per season than controls in their fourth postinjury season. Injured goalkeepers played more minutes per game than controls in their fourth postinjury year, but this difference was not significant (P = .753).
Goalkeeper Metrics Compared With 1 Year Before Index Year a
a Data are reported as mean ± SD. Bolding indicates statistically significant difference between groups. ACL, anterior cruciate ligament.
b Change in player performance metric as compared with 1 year before index year (ie, time of injury for players with a complete ACL tear and index year for matched controls).
Goalkeepers with an ACL tear achieved fewer shutouts per season in the year immediately after their injury compared with controls (P < .001). Interestingly at 2, 3, and 4 years after injury, injured goalkeepers logged significantly more shutouts (P < .05), but also conceded more goals per season (P < .05) than their matched controls.
Discussion
ACL rupture is one of the most common injuries suffered by professional soccer players and is associated with one of the longest absences. 35 Thus, a better understanding of the true rate of RTP and player performance after ACL rupture is imperative to guide expectations of athletes and clinicians. The present study performed a matched-cohort analysis of RTP rates and player performance in 51 elite UEFA league players who underwent ACLR. The principal findings were that (1) within 3 years, 80% of players sustaining ACL rupture return to play at the same league level as before ACLR and (2) player performance suffers in the 2 seasons after injury but, with the exception of attackers, largely equals or exceeds that of their matched controls by the third postinjury season. To date, this is the first study to perform a matched-cohort analysis of player performance for soccer players with an ACL rupture.
We found the mean RTP time to be 216 days with a resulting mean of 26 missed games for those who returned to play. This finding is supported by previous studies that have reported RTP to average 186 to 310 days for professional soccer players. 4,35,39 Interestingly, this RTP is significantly shorter than the 9 to 12 months currently recommended by evidence-based practice guidelines. 34 Of note, the mean RTP in professional European soccer appears to be significantly shorter than the National Hockey League (258 days), National Football League (370 days), Major League Baseball (418 days), and National Basketball Association (424 days). 24
Of the total 80% of players that returned to play at the same league level, 88% returned the season after their injury, with an additional 7% and 5% returning 2 and 3 seasons after injury, respectively. These findings are consistent with prior investigations, 4,7,13,21,28,39 of which Brophy et al 7 report a return to sport rate of 72%, specifically after ACLR. 7 Niederer et al 29 found a stark difference between rates of RTP between playing levels, with 98.2% of professional soccer players sustaining ACL rupture returning to any level of play but only 59.4% returning to the same league level. Similar to our results, Erickson et al 13 demonstrated a rate of 77% of American soccer players returning to the same playing level within the MLS organization, most of whom returned 1 season after injury. 13 Of those experiencing a subsequent ACL injury, our presently reported rate of 12% is consistent with prior investigations. Brophy et al 7 reported a retear rate of 12% while Erickson et al 13 reported a retear rate of 10% among American soccer players. Evidently, while a majority of soccer players return to play in the same league level during the following playing season, ACL rupture does result in loss of a significant number of players from returning to the league with a notable rate of reinjury.
The mean age of injured players is 25.9, 23.4, and 24.4 years for attackers, midfielders, and defenders, respectively. Interestingly, Dendir 10 found the age of peak performance for these positions to be 25, 25 to 27, and 27, respectively. Thus, this investigation finds attackers experience ACL injuries after their peak performance age, whereas defenders and midfielders injure themselves, on average, before their age of peak performance. Bloomfield et al 6 demonstrated that among professional soccer players, attackers undertake the most maximal sprints, perform significantly more shuffling and explosive movements, endure more physical contact at high intensity, and undertake more high intensity activity relative to midfielders and defenders. These activities demand physical capabilities from attackers that have likely deteriorated after their age of peak performance, making them more susceptible to injury. While less physically demanding, the role of the defenders and midfielders relies more on experience, which increases with age. 10 Consistent with this theory, we found these players to injure themselves more frequently before their age of peak performance.
In terms of player performance after RTP, we observed that athletes with ACL rupture played fewer games, fewer minutes (per season and per game), and scored less in the 2 seasons after injury compared with their matched cohort. By the third postinjury season, injured players (with the exception of attackers) had a similar performance to noninjured players. This is consistent with the current literature that has found soccer players start fewer games and score fewer goals per game at 3 seasons after injury. 4 Similarly, Niederer et al 29 found that ACL injury negatively affected both player performance and career duration. These data suggest that while a soccer player may be medically cleared to RTP, they likely have not returned to their preinjury fitness level.
Current management approaches heavily weigh standardized protocols and timelines with a relative lack of emphasis on individualized assessment. Although some players do return to their preinjury level, the timeline of 3 seasons after injury leaves considerable room for improvement. Almeida et al 2 found aerobic fitness to be significantly reduced in professional soccer players up to 6 months after ACLR compared with controls, while van Melick et al 36 found movement quality while fatigued to be more negatively affected in players having undergone ACLR. Given the intense physical and biomechanical demands unique to the elite soccer player, these nuanced postinjury deficits may explain the decrease in performance after ACL injury. Rehabilitation protocols that specifically address and monitor these deficits in elite soccer athletes may provide clinicians and players with more pointed feedback to help guide a more successful and expeditious recovery.
Limitations
An important limitation to consider when interpreting the presented results includes the use of public data sources in generating the ACL rupture player cohort. This lends the possibility of a selection bias toward players with publicly reported injuries while not capturing information on injuries players sustain that remain undisclosed to the public. This limitation is minimized in the context of investigating ACL ruptures due to the prolonged rehabilitation necessary after injury, and thus low likelihood of a player’s reason for absence remaining undisclosed to the public. Additionally, it was not possible to determine individual players’ differences in concomitant knee injuries, treatment, rehabilitation, and patient-reported outcomes without access to official medical record documentation which may affect RTP rates and time to RTP. Nonetheless, optimal medical management after ACL rupture in professional athletes has been well-established to include both surgical intervention and rehabilitation exercises focused on mobility and strengthening. 8,20,32,34 Of note, the management of ACL injures has evolved over the 20-year period studied. Importantly, the RTP levels may be even greater than 80% due to players joining other professional leagues for more prominent team roles, as our methodology did not capture these players.
Finally, creating matched cohorts for elite athletes poses the challenge of maximizing similarities in player characteristics within the restriction of a relatively small and fixed number of players from which to select. Prior investigations have relied on either manual selection of players or matching of calculated propensity scores to generate matched cohorts. Manual matching imparts a significantly elevated risk of selection bias whereas use of an aggregated propensity score imparts the significant limitation of generating higher levels of imbalance thus skewing and potentially masking effects of statistical models calculated. 18,19,22,26 To minimize these potential risks of bias associated with matching, we used a matching method that optimizes the matching solution for a given data set and thus minimizes the imbalances within each group that are otherwise unaccounted for with manual and propensity score matching. The matching method did not control for baseline performance metrics between groups, including minutes played per season and goals scored per season. It is also worth noting that the relatively small sample size of injured players may limit the application of the study findings; however, elite soccer players represent a small population, making high power analysis difficult. By including injuries from 2016 to 2019, players’ performance at 2 to 4 years was not captured in every player.
Conclusion
The average RTP time for elite UEFA league soccer players after ACLR is less than other major sports leagues (216 days). However, RTP rates are high (80%) and rerupture rates are comparable with those of other sports at 12%. With the exception of attackers, player performance largely equals or exceeds that of matched controls by the third postinjury season (P < .05).
Footnotes
Final revision submitted November 23, 2020; accepted January 4, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.F. has received consulting fees and hospitality payments from Stryker Corp, grants from Arthrex and Stryker Corp, education payments from Medwest, personal fees from Elsevier and Stryker Corp, and research support from Smith & Nephew; and he has stock in Jace Medical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.