
Abstract
Background:
Different techniques are used for the remplissage procedure, including the double-pulley and mattress suture techniques. Both techniques have shown good results; however, it is unclear if one technique is superior.
Hypothesis:
The remplissage procedure using the double-pulley technique with 2 anchors would have superior functional and radiological outcomes compared with the mattress suture technique with a single anchor.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This study included patients with anterior shoulder instability who were treated using arthroscopic Bankart repair combined with remplissage between 2012 and 2017. A structured questionnaire was used to gather information on the following metrics: Instability Severity Index Score, hyperlaxity, Sugaya index, presence of a Hill-Sachs defect, number of dislocations before surgery, sports participation, radiological measurement of the Hill-Sachs lesion, postoperative range of motion in both shoulders, Rowe score, Walch-Duplay score, American Shoulder and Elbow Surgeons score, and Filling Index Score of Remplissage grade according to magnetic resonance imaging scans at the last follow-up.
Results:
There were 41 patients included with a mean age of 30 ± 7 years who underwent the Hill-Sachs remplissage procedure using the double-pulley technique with 2 anchors (n = 21; group DA) or the mattress suture technique with a single anchor (n = 20; group SA). At the final follow-up, there were no significant differences between the groups regarding the Instability Severity Index Score (P = .134), the Sugaya index (P = .538), sports participation (P = .41), the radiological measurement of the Hill-Sachs lesion (P = .803), or the Rowe score (P = .182). However, there were significant differences between the groups in the Walch-Duplay score (P = .012), American Shoulder and Elbow Surgeons score (P = .005), and Filling Index Score of Remplissage grade (P = .015), favoring group DA, as well as differences in external rotation in a neutral position (external rotation loss: 9° ± 3° [group SA] vs 12° ± 3° [group DA]; P = .003) and at 90° of abduction (external rotation loss: 8° ± 3° [group SA] vs 11° ± 3° [group DA]; P = .006), favoring group SA.
Conclusion:
In the remplissage procedure, the double-pulley technique provided better filling of the lesion and improvement in functional scores, but external rotation was limited compared with the mattress suture technique.
Hill-Sachs lesions were defined in 1940 as one of the most important causes of recurrent glenohumeral instability and occur because of impaction of the cancellous humeral head on the harder anterior-inferior glenoid rim. 21 This lesion is present in 40% to 70% of first-time traumatic shoulder dislocations and up to 90% of recurrent shoulder dislocations. 30,38,45 Defects greater than one-third of the humeral head and parallel to the glenoid axis are important for prognosis and play an important role in recurrent instability. On the other hand, in the presence of lateralized, nonengaging, and small Hill-Sachs defects, if there is no glenoid bone loss, good results can be achieved using only Bankart repair. 2,5 “Engaging” Hill-Sachs lesions, as described by Burkhart and De Beer, 7 refer to lesions that engage the humeral head to the glenoid in abduction and external rotation. Failure to identify an engaging Hill-Sachs lesion during Bankart repair has been associated with recurrent instability. 6,7,14,32
The remplissage procedure, which means “to fill in” in French, was first described by Purchase et al 31 as advancement of the posterior capsule and infraspinatus tendon to prevent the glenoid rim from engaging into the Hill-Sachs lesion. The purpose of this procedure is to transform an intra-articular Hill-Sachs defect into an extra-articular defect, thereby preventing engagement. This technique was presented as an alternative treatment to the Latarjet procedure, 25 humeral head resurfacing, 1,19 rotational osteotomy, 42 defect filling using allografts, 24 and transhumeral impaction grafting. 33 The remplissage procedure has been highlighted because of its arthroscopic approach and reduced operative duration, good functional results, shorter rehabilitation time, and avoidance of complications associated with bone grafting. 17 Different techniques are used for the remplissage procedure, including the double-pulley and mattress suture techniques. 4,10,11,23 These 2 techniques differ from each other in the number and location of anchors inserted at the defect and in cleaning of the subacromial space before capsulotenodesis. Both techniques have shown good results; however, it is unclear if 1 technique is superior. 14,26
The purpose of this study was to compare the functional and radiological outcomes of the double-pulley technique using 2 anchors and the mattress suture technique using a single anchor in the Hill-Sachs remplissage procedure. It was hypothesized that the double-pulley technique would provide better filling of the lesion with less instability but limit shoulder range of motion (ROM) compared with the mattress suture technique.
Methods
Study Design
This 2-center, retrospective, comparative study was conducted at Bezmialem Vakif University and Medline Adana Hospital in Turkey between 2012 and 2017. The study protocol received institutional review board approval. The procedures were performed arthroscopically using 2 different techniques by 2 senior orthopaedic surgeons (S.A. and K.B.). Each surgeon used only 1 of these techniques. Patients participated in the study voluntarily after receiving an explanation of the risks and benefits and were required to sign an informed consent form before enrollment. A structured questionnaire was used to gather information on the following patient metrics: descriptive data, number of dislocations before surgery, sports participation, Instability Severity Index Score, 2 and preoperative and postoperative follow-up times.
Patient Selection
Patients with recurrent traumatic anterior shoulder dislocations were included in the study, as the approach in our practice is to treat first-time dislocations in a nonoperative manner. Inclusion criteria were a deep and medialized Hill-Sachs lesion that engaged over the anterior glenoid rim in abduction–external rotation at the time of arthroscopic surgery before Bankart repair and bone loss of <15% of the glenoid surface. The Instability Severity Index Score for all patients was ≥3, and all patients had a minimum follow-up of 2 years. These criteria were based on evidence showing that “subcritical” glenoid bone loss of >15% and an engaging Hill-Sachs lesion are associated with a significantly higher risk of recurrent instability and that patients with an Instability Severity Index Score of ≥3 are at an unacceptably high risk (>10%) of recurrent instability after isolated arthroscopic Bankart repair. 5,44
Patients were excluded from the study if they had concomitant injuries including frozen shoulder (n = 1), superior labrum anterior to posterior lesions (n = 2), posterior labral tears (n = 1), rotator cuff tears (n = 1), glenohumeral arthritis (n = 1), multidirectional instability (n = 4), and greater tuberosity fractures (n = 1); if they had a history of surgery for shoulder instability (n = 3); if they showed noncompliance with the physical therapy protocol (n = 1); if they were aged >50 years (n = 1); if the Hill-Sachs lesion was absent on radiological imaging (n = 1); or if no postoperative radiological imaging data were available (n = 4) (Figure 1).
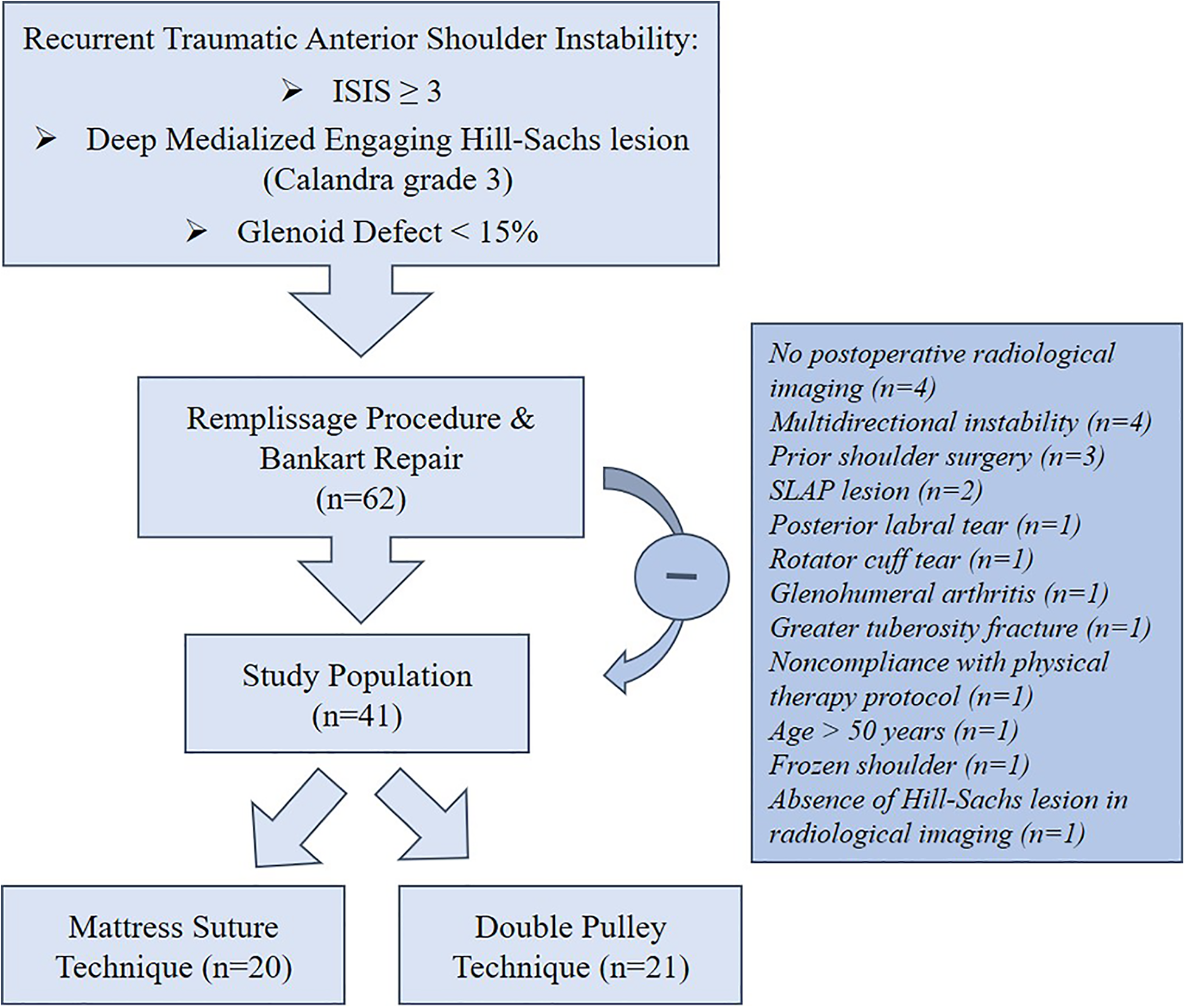
Study flowchart. ISIS, Instability Severity Index Score; SLAP, superior labrum anterior to posterior.
Clinical Evaluation
The clinical assessment was performed by an orthopaedic surgeon (B.O.) and physical therapist who were blinded to the treatment modality and radiological outcome. In the apprehension test, the shoulder was abducted to 90° and rotated externally to assess anterior glenohumeral instability. The Gagey hyperabduction test or sulcus sign test was used to assess inferior glenohumeral instability. Multidirectional instability was defined as symptomatic glenohumeral joint subluxations or dislocations occurring in >1 direction.
Postoperative active ROM, including forward flexion, abduction, external rotation in a neutral position, and external rotation at 90° of abduction, was measured and recorded for both shoulders at the last follow-up. The difference between the affected and unaffected sides, defined as motion loss, was calculated using a universal goniometer. Internal rotation was assessed using the highest spinal level reached by the patient’s thumb and then rated as buttocks (2 points), sacrum (4 points), L3 (6 points), T12 (8 points), or higher than T7 (10 points). The Rowe score 35 (composed of stability, motion, and function), the Walch-Duplay score 41 (consisting of activity, stability, pain, and mobility), and the American Shoulder and Elbow Surgeons 28 (ASES) score (comprising pain and function) were utilized for the functional evaluation of the patients. The presence of subluxation or dislocation episodes was defined as recurrence.
Radiological Evaluation
Radiological assessments were performed by a senior musculoskeletal radiologist lacking knowledge about the clinical outcome. All patients underwent plain radiography, computed tomography (CT), and magnetic resonance imaging (MRI) preoperatively. The glenoid defect was assessed using 3-dimensional CT multiplanar reconstruction using a sagittal en face view of the glenoid bone. The glenoid defect was evaluated using the Sugaya index, which is the ratio of the remaining glenoid width to its diameter. 39 The Hill-Sachs lesion was measured on the axial CT section on which the defect was largest. On this section, the most suitable circle was drawn from medial to lateral around the humeral head. The surface areas of the humeral head and Hill-Sachs defect were measured and recorded using a picture archiving and communication system program. The ratio of the Hill-Sachs lesion surface area to the surface area of the humeral head was calculated as a percentage of the defect (Figure 2).

Measurement of the humeral head surface area (H) and Hill-Sachs defect surface area (h) on preoperative computed tomography to calculate the Hill-Sachs defect ratio (h/H).
Patients underwent MRI to assess filling of the Hill-Sachs lesion and healing after capsulotenodesis at the last follow-up. All MRI examinations were performed using a 1.5-T MRI scanner (Siemens, Avanto) using routine pulse sequences without contrast media in external rotation of the shoulder to relax the infraspinatus tendon. The Filling Index Score of Remplissage (FISOR) was used to classify filling of the lesion with the posterior joint capsule and infraspinatus tendon (Table 1). 34 The assessment was performed using the axial MRI section on which the defect size was the largest, and this section was subsequently used as a scout image. The sagittal sections were opened on the monitor screen, and the most appropriate section was selected. The measurements in both planes were performed using digital imaging software. The total sum of the scores from the axial and sagittal planes was classified into 5 grades: excellent (7-8 points), good (5-6 points), fair (3-4 points), poor (1-2 points), and no filling of the lesion (0 points).
Filling Index Score of Remplissage Grading System 34

Surgical Procedure
All patients underwent surgery under general anesthesia in the beach-chair position. The shoulder was examined for instability before surgery by abducting the arm to 90° with varying degrees of external rotation. After draping and preparing the patient, bony landmarks were drawn, and standard stabilization portals including anterior and posterior portals were established. Diagnostic arthroscopic surgery was performed to identify Bankart and Hill-Sachs lesions. The anterior labrum and glenoid were prepared for Bankart repair. Subsequently, an anterosuperolateral portal was created to provide a better view of the glenoid surface.
A dynamic arthroscopic examination was performed to identify an “engaging” Hill-Sachs lesion in abduction and external rotation (Figure 3). The depth of the Hill-Sachs lesion was assessed during arthroscopic surgery and graded using the Calandra classification (grade 1, defect on the articular surface down to, but not including, subchondral bone; grade 2, defect on the articular surface including subchondral bone; and grade 3, large defect on subchondral bone). 9,37 The presence of a deep, medialized, “engaging” Hill-Sachs lesion (Calandra grade 3) intraoperatively, as well as a correlation with the preoperative imaging findings, informed the decision to perform the remplissage procedure. After preparation of the Hill-Sachs bone defect and anterior labrum, the procedure was performed sequentially by first passing the suture through the infraspinatus tendon and then through the posterior capsule and finally tying it after performing Bankart repair.

Detection of a deep (Calandra grade 3), medialized, “engaging” Hill-Sachs lesion using a dynamic arthroscopic examination.
For the mattress suture technique, a single 5.5-mm, titanium, double-loaded suture anchor (Corkscrew FT Anchor; Arthrex) was inserted into the center of the defect perpendicularly. 10 A sharp tissue penetrator (BirdBeak suture passer; Arthrex) was used to pass the sutures through the posterior capsule and infraspinatus tendon. The first pair of suture strands from the double-loaded anchor was passed through the superomedial and superolateral margins of the lesion, followed by the second pair of suture strands, which was passed through the inferomedial and inferolateral margins (Figure 4). The superior and inferior suture strands were tied in a blinded fashion.

(A) Insertion of a single double-loaded suture anchor in the center of the defect and establishment of a quadrangular suture configuration using the mattress suture technique. (B) Illustration of the mattress suture technique on sagittal and axial views with the sutures tied down to fill the Hill-Sachs defect with the infraspinatus tendon.
For the double-pulley technique, two 4.5-mm, single-loaded, metal suture anchors (Twinfix Ultra Ti; Smith & Nephew) were inserted at the superior and inferior borders of the Hill-Sachs lesion, next to the articular margin (Figure 5). 23 A sharp tissue penetrator (Arthro-Pierce; Smith & Nephew) was used to pass the suture strands through the posterior capsule and infraspinatus tendon. The subacromial space was cleaned to visualize the infraspinatus tendon and to prevent interposition of bursal tissue. Neither subacromial decompression nor acromioplasty was performed in any patient. One limb from each suture anchor was tied together and fixed using the double-pulley technique. The remaining limbs were tied, and the suture tails were cut.

(A) Positioning of 2 single-loaded suture anchors next to cartilage using the double-pulley technique. (B) Illustration of the double-pulley technique on sagittal and axial views with the sutures tied down to fill the Hill-Sachs defect with the infraspinatus tendon.
Postoperative Follow-up Protocol
A standard postoperative rehabilitation protocol was applied for all patients. After surgery, the shoulder was immobilized in a 30° of abduction sling at a neutral rotation for 6 weeks while enabling gentle elbow, wrist, and finger motions. Shoulder pendulum exercises were started during the third postoperative week. Gradual external rotation of the shoulder was initiated during the fourth week. Active assisted shoulder ROM was allowed at 6 to 8 weeks, and active exercises were initiated at 8 to 12 weeks. Return to sports was allowed at 6 months after the shoulder regained >90% of its strength compared with that of the contralateral side.
Statistical Analysis
All statistical analyses were performed using the SPSS statistical software package (2011; IBM Corp). The Shapiro-Wilk test was used to determine the concordance of continuous data in a normal distribution. Continuous data are presented as the median (range) and mean ± standard deviation. Comparisons between groups were performed using the Mann-Whitney test and independent-samples t test. Categorical data were compared using the Fisher exact test. The results are reported as related P values. P < .05 was considered statistically significant.
Results
Patient Characteristics
A total of 41 patients who underwent the remplissage procedure were included in the study. Overall, 20 patients were treated using the mattress suture technique with a single anchor (group SA), and 21 were treated using the double-pulley technique with 2 anchors (group DA). The characteristics of the patients were similar in both groups (Table 2). The mean follow-up was 43.2 ± 10.2 months (range, 28-65 months).
Patient Characteristics a
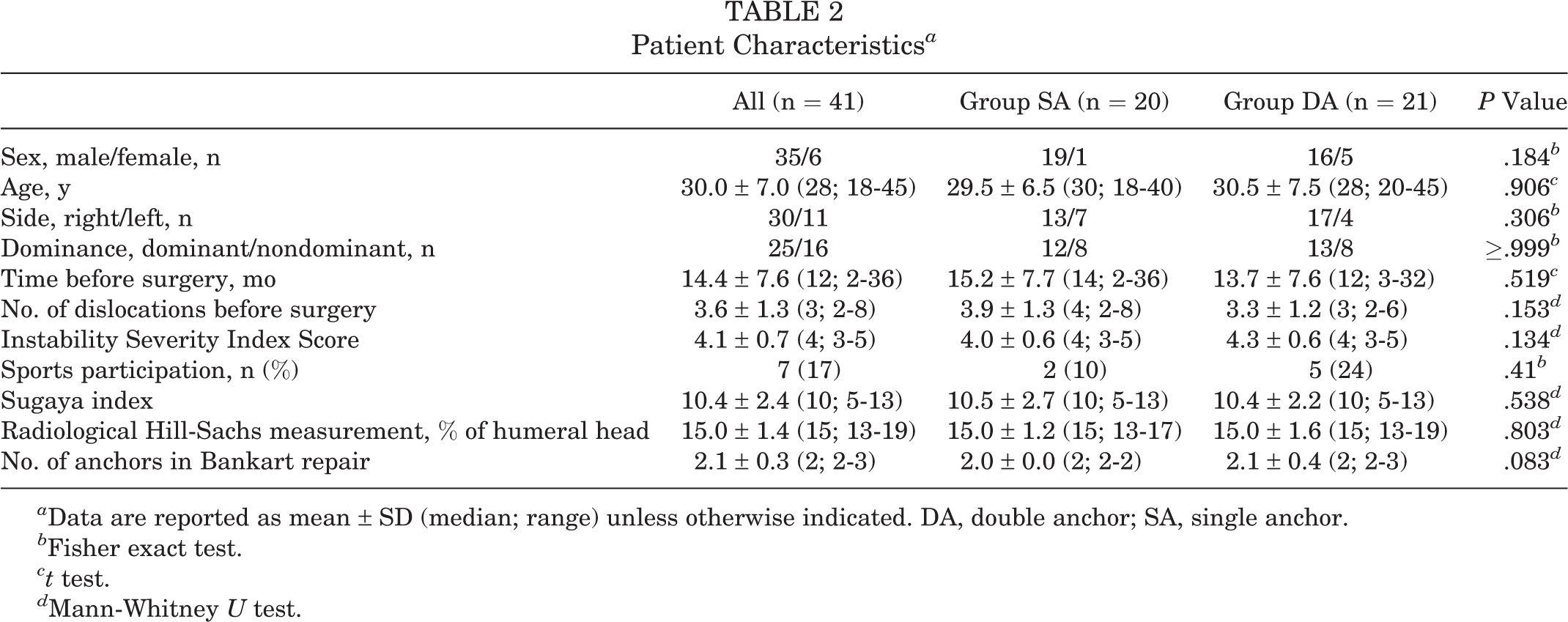
a Data are reported as mean ± SD (median; range) unless otherwise indicated. DA, double anchor; SA, single anchor.
b Fisher exact test.
ct test.
d Mann-Whitney U test.
Clinical Findings
The mean postoperative forward flexion, internal rotation, external rotation in a neutral position, and external rotation at 90° of abduction were 174.9° ± 6.6° (range, 150°-180°), 9.4° ± 0.9° (range, 8°-10°), 70.7° ± 7.3° (range, 55°-90°), and 81.5° ± 5.3° (range, 70°-90°), respectively, at the last follow-up. The mean loss of forward flexion, internal rotation, external rotation in a neutral position, and external rotation at 90° of abduction were 2.4° ± 5.3° (range, 0°-30°), 0.3° ± 0.8° (range, 0°-2°), 10.5° ± 3.1° (range, 5°-15°), and 9.5° ± 3.5° (range, 5°-15°), respectively. At the last follow-up, the mean ASES, Rowe, and Walch-Duplay scores were 90.4 ± 3.8 (range, 80-95), 89.3 ± 4.7 (range, 80-95), and 88.7 ± 6.2 (range, 65-95), respectively.
The difference in the amount of external rotation loss in a neutral position (P = .003) and at 90° of abduction (P = .006) in group SA was significantly less than that in group DA. Patients in group DA had higher ASES (P = .005) and Walch-Duplay (P = .012) scores than did those in group SA (Table 3). Post hoc power analysis according to the primary outcomes (ASES and Walch-Duplay scores, mean loss of external rotation) with a significance level of .05 showed a large effect size (2.11) and a power (1 – β) between 0.72 and 0.91, which confirmed that the sample size was adequate.
Clinical and Radiological Outcomes a

a Data are reported as mean ± SD (median; range) unless otherwise indicated. Bolded P values indicate a statistically significant difference between groups. ASES, American Shoulder and Elbow Surgeons; DA, double anchor; ER, external rotation; FISOR, Filling Index Score of Remplissage; SA, single anchor.
b Mann-Whitney U test.
c Fisher exact test.
Radiological Findings
On preoperative CT scans, the mean Sugaya index was 10.4 ± 2.4 (range, 5-13), and the Hill-Sachs lesion accounted for 15.0% ± 1.4% (range, 13%-19%) of the humeral head. The mean FISOR grade was 6.3 ± 1.4 (range, 3-8) on MRI at the last follow-up (Figure 6). The FISOR grade was 8 points in 10 patients (24%), 7 points in 9 patients (22%), 6 points in 10 patients (24%), 5 points in 9 patients (22%), 4 points in 1 patient (2%), and 3 points in 2 patients (5%). FISOR grading according to groups is shown in Table 4. The mean FISOR grade of group DA (6.8 ± 1.3) was significantly higher than that of group SA (5.8 ± 1.3) (P = .015).
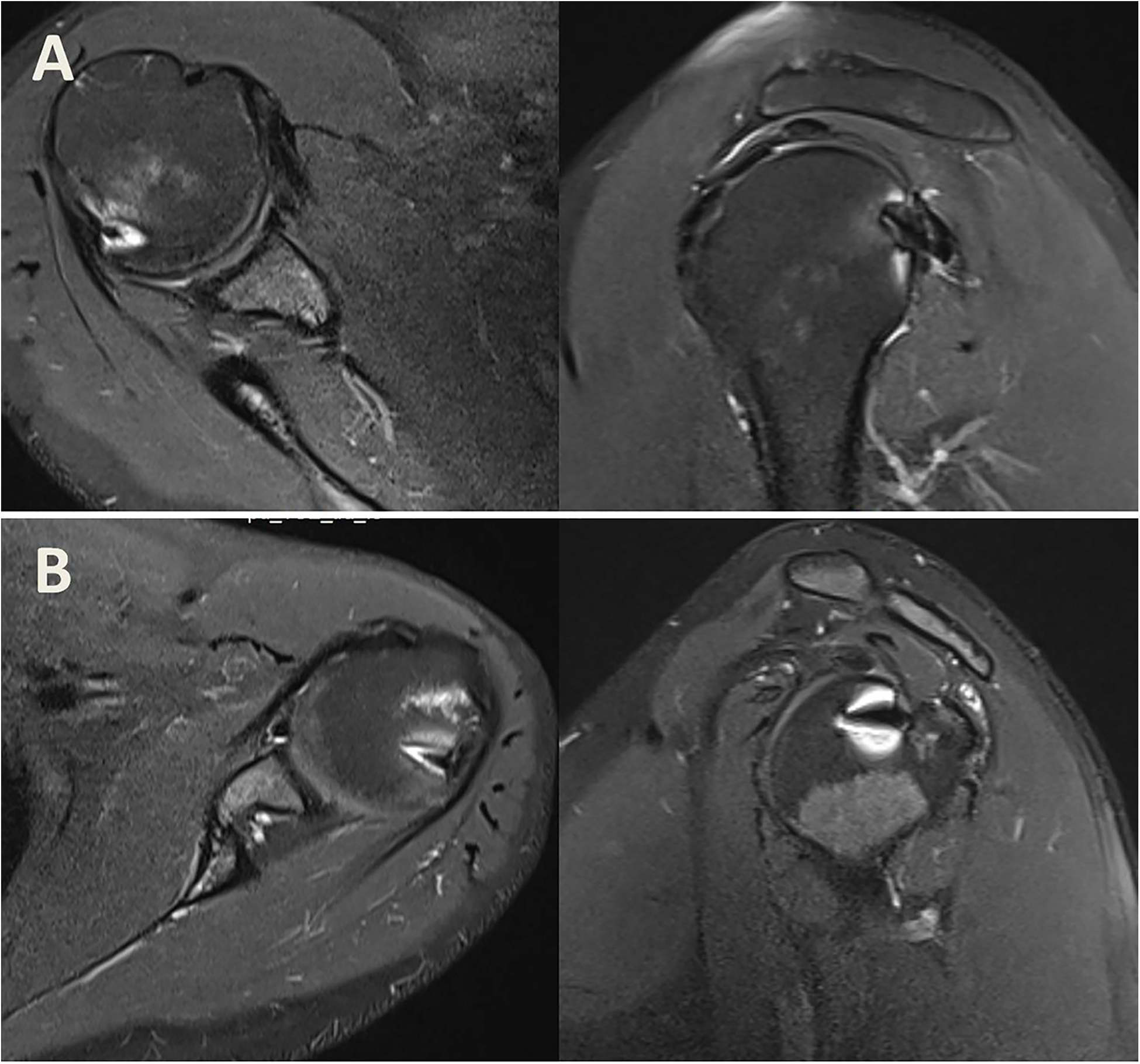
Detection of excellent filling on magnetic resonance imaging scans at the last follow-up after the remplissage procedure using the (A) mattress suture technique and (B) double-pulley technique.
FISOR Grades a
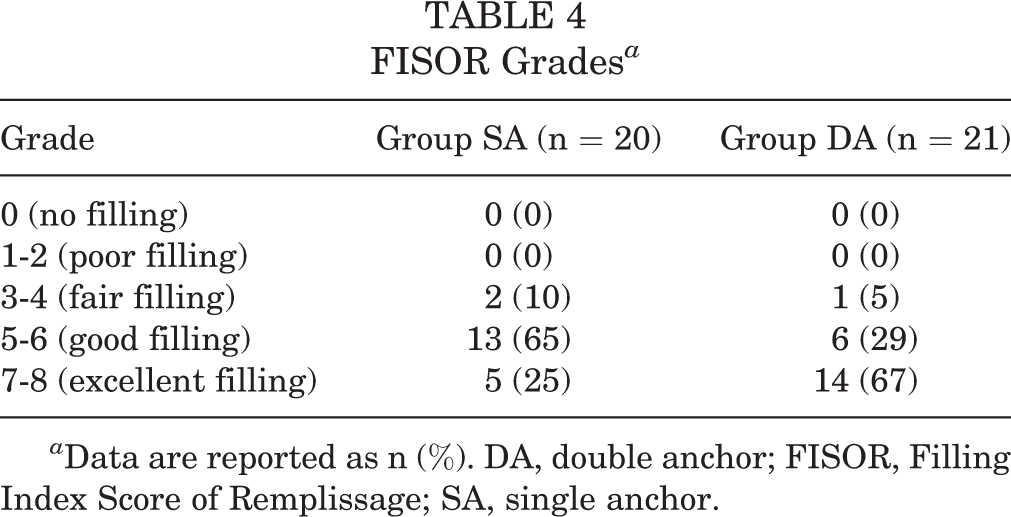
a Data are reported as n (%). DA, double anchor; FISOR, Filling Index Score of Remplissage; SA, single anchor.
Complications
Postoperative shoulder instability was observed in 3 (7%) patients; 1 (5%) of them was in group SA, and 2 (10%) of them were in group DA. The 2 patients in group DA underwent revision surgery using the arthroscopic Latarjet procedure. They remained symptom-free at the final follow-up (36 and 48 months). The shoulder of the 1 patient with recurrence in group SA was stable enough for activities of daily living; therefore, the patient declined further surgery and remained symptom-free at the final follow-up (35 months). No other postoperative complications were observed. There was no significant difference in recurrence between the groups (P ≥ .99).
Discussion
The significant finding of this study was that there was less restriction of external rotation using the mattress suture technique than the double-pulley technique both in a neutral position and at 90° of abduction. On the other hand, the double-pulley technique resulted in better Walch-Duplay and ASES scores as well as better defect filling on MRI scans at the final follow-up than did the mattress suture technique.
The remplissage procedure is frequently used for the treatment of engaging Hill-Sachs lesions; however, there is no standard surgical technique for this procedure, and there are many described variations. 4,10,11,23,31 Importantly, the literature comparing the outcomes of various remplissage techniques is limited. In the mattress suture technique, the suture anchor is placed at the center of the defect, whereas it is placed at the edge of the humeral head defect adjacent to subchondral bone in the double-pulley technique. 10,23 In a biomechanical study, Elkinson et al 13 compared 3 different techniques of remplissage and reported no significant difference between placement of the suture anchor at the center of the valley or at the humeral edge of the defect adjacent to subchondral bone. These researchers also concluded that both 15% and 30% Hill-Sachs defects significantly restricted glenohumeral rotation, independent of the position of the anchor, if the sutures were passed 1 cm medially through the infraspinatus tendon and capsule. These researchers also reported a mean rotation restriction of 21° for 15% Hill-Sachs defects (P = .034) and 13° restriction for 30% Hill-Sachs defects (P = .044). However, in their study, they routinely used a single anchor in 15% Hill-Sachs defects and 2 anchors in 30% defects for capsulotenodesis. As a result, a comparison of stability and rotation restriction based on the number of anchors was not possible.
Deutsch and Kroll 12 were the first to report that capsulotenodesis may cause a mechanical block to external rotation after the remplissage procedure; however, this finding is still controversial in the literature. Despite some studies showing that external rotation is significantly restricted between 2° and 10°, 5,20,27 several studies have shown that this restriction is mild and not statistically significant. 8,16,18,31,40,46 In addition, Boileau et al 5 and Merolla et al 27 reported that the effect of ROM restriction on daily activities was very small. The characteristics, size of the Hill-Sachs defect, ROM measurement method, operative position, and technique were all variable in these studies without a comparison of techniques. Therefore, it is difficult to determine the restriction of external rotation based on the surgical technique. In our study, the double-pulley technique using 2 anchors, with a large footprint, caused more limited external rotation compared with the mattress suture technique using a single anchor in patients with similar characteristics. This study demonstrates that the surgical technique and the number of anchors used in the remplissage procedure may affect external rotation.
A classification method for determining whether Hill-Sachs lesions are engaged was recently defined in the literature. Yamamoto et al 43 classified these lesions as on-track or off-track according to the glenoid track concept using preoperative CT scans. Itoi 22 stated that a Hill-Sachs lesion that stays on the glenoid track (on-track lesion) cannot engage with the glenoid and cannot cause dislocations; therefore, failure to repair the labrum before a dynamic examination overestimates the rate of engaging Hill-Sachs lesions. Although the glenoid track concept is important and accepted in the literature, the 2 senior surgeons in the current study did not use this concept in preoperative planning in their daily surgical practice during the study period. In addition, there is still a need for further studies to determine when a bony procedure is indicated versus the Hill-Sachs remplissage procedure combined with arthroscopic Bankart repair. Shoulder instability is a dynamic problem with humeral head translation that can also be examined in an active diagnostic arthroscopic setting. As we gain increased understanding of the dynamic interactions between the glenoid and Hill-Sachs lesion, we can determine the bony defects and engagement of the Hill-Sachs lesion during the arthroscopic procedure. Our indications for combining the Hill-Sachs remplissage procedure with arthroscopic Bankart repair were the same as those reported by Boileau et al 5 : symptomatic recurrent traumatic anteroinferior glenohumeral instability, Instability Severity Index Score ≥3, deep medialized Hill-Sachs (Calandra grade 3) defect engaging over the anterior glenoid rim in abduction–external rotation, and absence of substantial anteroinferior glenoid bone loss on preoperative imaging and intraoperative arthroscopic examinations. Therefore, we propose focusing on this dynamic anterior glenohumeral instability situation to predict the risk of recurrence and to consider the glenoid to be an important prognostic factor.
In the literature, previous studies on arthroscopic Bankart repair combined with the remplissage procedure have cited good to excellent postoperative functional scores with consistently high satisfaction; however, these studies were performed without a comparison of techniques. 5,8,15,16,18,27,40,46 In our study, the mean ASES, Rowe, and Walch-Duplay scores were 90.4 ± 3.8 (range, 80-95), 89.3 ± 4.7 (range, 80-95), and 88.7 ± 6.2 (range, 65-95), respectively, at the last follow-up. The functional scores in our study were similar to those in other studies in the literature. Our patients treated using the double-pulley technique had good functional scores, despite having restricted external rotation, compared with those in our patients treated using the mattress suture technique. Although these differences may not be clinically significant, they might be important in the population of patients participating in overhead sports. In our opinion, this nonanatomic procedure, which creates a large footprint area using the double-pulley technique, decreases both the articulating surface of the humeral head and the joint space, thereby restricting external rotation. In contrast, the functional scores of the patients increased because of increased shoulder stability. Although there is a statistical difference between these 2 techniques in terms of both external rotation restriction and functional scores, their effect on daily activities is negligible.
The apprehension test is being used in some studies to describe recurrence after the remplissage procedure, although many have used the presence of dislocations or subluxations instead. Previous studies have demonstrated that the rate of dislocation recurrence is 0% to 15% 3,5,15 –18,20,27,29,46 and that the rate of positive apprehension is 0% to 16%. 3,15,16,34,46 According to Boileau et al, 5,6 the reduction of recurrence is partly related to the application of strict operative indications, which reinforces their opinion that Hill-Sachs remplissage must strictly be applied in patients with humeral head bone loss. Interpreting the studies on this subject is quite difficult because of differences in parameters, such as patient characteristics, operative techniques, and the number of suture anchors. In our study, recurrence, defined as the presence of dislocations or subluxations, was found in 3 of 41 (7%) patients: 1 (5%) in group SA and 2 (10%) in group DA. Importantly, 2 patients with instability symptoms and recurrent dislocations underwent revision surgery using the Latarjet procedure; however, the other patient refused to undergo additional surgery because of satisfaction with activities of daily living. The groups could not be compared with each other in terms of instability recurrence because the number of patients with recurrent instability was low in both groups. Additional studies are needed to investigate the effect of the technique on the recurrence of instability after the remplissage procedure.
Rhee et al 34 described the use of the FISOR based on MRI with contrast media to assess structural healing of the infraspinatus tendon after the remplissage procedure. These researchers reported good and excellent healing results in 19 of 23 (83%) patients. In contrast, França et al 15 reported that the relaxed infraspinatus tendon in the external rotation position may provide a good structural assessment without the use of contrast media, and they found a high grade of filling in 25 of 25 (100%) patients. In our study, we used the FISOR without contrast media to evaluate the infraspinatus tendon at the last follow-up. As a result, 19 of 41 (46%) excellent and 19 of 41 (46%) good radiological healing outcomes were obtained. In line with the functional scores, radiological outcomes were also significantly better in group DA with 2 anchors and 2 fixation points, which creates a larger footprint area, than in group SA with a single anchor (P = .015). In our opinion, the use of contrast media is not necessary because of possible side effects of contrast material, such as pain, pruritus, anxiety, and infections. 36
Limitations
This study has several limitations, including its retrospective nature and the small number of patients. Although the characteristics of patients in groups SA and DA were similar, 2 different techniques were performed separately by 2 different senior shoulder surgeons at 2 different centers. Each surgeon used only 1 of these techniques. In addition, there was no randomization and no specific selection criteria for the double-pulley technique using 2 anchors versus the mattress suture technique using a single anchor. Not using the glenoid track concept in the assessment of instability can also be considered a limitation. 22,43 During the radiological evaluation, the radiologist could not be blinded to the technique used because of the number of anchors in the humeral head. Regarding the imaging results, all MRI examinations were performed without the use of contrast media, as routine and fatty muscle degeneration was not evaluated. The overwhelming majority of participants were male and did not participate in sports, and none of the participants was aged <18 years; therefore, the results may not reflect the outcomes of female patients or patients heavily involved in sports. A comparison of only the double-pulley and mattress suture techniques in the remplissage procedure is another limitation because of the existence of other validated techniques, including the tripod-pulley 11 and double-barrel 4 techniques. Another limitation of the study is the absence of quantification regarding the loss of infraspinatus muscle strength.
Conclusion
Good functional and radiological results were obtained after arthroscopic Bankart repair combined with the remplissage procedure using either the double-pulley technique with 2 anchors or the mattress suture technique with a single anchor for the treatment of recurrent anterior shoulder instability. Comparative analyses at the final follow-up showed significant differences in FISOR grades as well as Walch-Duplay and ASES scores, which favored the double-pulley technique using 2 anchors, and in external rotation, which favored the mattress suture technique using a single anchor. However, the clinical significance of these differences seems to be negligible. Future prospective, randomized, controlled comparative studies involving more patients and with longer follow-up times are needed to determine which technique might be more satisfactory in terms of clinical and radiological results for the Hill-Sachs remplissage procedure.
Footnotes
Final revision submitted December 4, 2020; accepted January 5, 2021.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Bezmialem Vakif University (No. 45446446-010.99-3589).