
Abstract
Background:
Prevention of sports injuries is essential in youth, as injuries are associated with less future physical activity and thus greater all-cause morbidity.
Purpose:
To investigate whether a neuromuscular training warm-up operated by team coaches is effective in preventing acute lower extremity (LE) injuries in competitive U11-U14 soccer players.
Study Design:
Randomized controlled trial; Level of evidence, 1.
Methods:
Twenty top-level U11 to U14 soccer clubs in Finland were randomized into intervention and control groups and assessed for 20 weeks. Participants included 1403 players (280 female, 1123 male; age range, 9-14 years): 673 players (44 teams) in the intervention group and 730 players (48 teams) in the control group. The intervention group team coaches were introduced to a neuromuscular training warm-up to replace the standard warm-up 2 to 3 times per week. The control teams were asked to perform their standard warm-up. Injury data collection was done via weekly text messages. The primary outcome measure was a soccer-related acute LE injury, and the secondary outcome measure was an acute noncontact LE injury.
Results:
A total of 656 acute LE injuries occurred: 310 in the intervention group and 346 in the control group. The overall acute LE injury incidence was 4.4 per 1000 hours of exposure in the intervention group and 5.5 per 1000 hours of exposure in the control group, with no significant difference between groups (incidence rate ratio [IRR], 0.82 [95% CI, 0.64-1.04]). There were 302 acute noncontact LE injuries: 129 in the intervention group (incidence, 1.8 per 1000 hours) and 173 in the control group (2.7 per 1000 hours). A significant reduction in acute noncontact LE injuries of 32% (IRR, 0.68 [95% CI, 0.51-0.93]) was observed in the intervention group compared with the control group. Furthermore, significant reductions in injury incidence in favor of the intervention group were seen in the subanalyses of acute noncontact LE injuries, leading to ≤7 days of time loss and fewer ankle and joint/ligament injuries.
Conclusion:
A neuromuscular training warm-up operated by team coaches was found to be effective in preventing acute noncontact LE injuries in children’s soccer, but this was not seen in all acute LE injuries.
Clinical Relevance:
We encourage children’s soccer coaches and health care professionals to implement neuromuscular training warm-up in youth sports.
Registration:
ISRCTN14046021 (ISRCTN registry).
Soccer is broadly beneficial for overall health, 19 but there is a downside to participation in the sport—an increased risk of injury. 5,6,13 Severe and recurrent sports injuries are associated with decreased future physical activity and, consequently, a greater risk for all-cause morbidity, obesity, and posttraumatic osteoarthritis. 9,22 Injuries in youth sports are a public health concern that requires special attention. 4
Much research has been done regarding soccer injuries and their prevention in youth (U19) and adult players. There is, however, a paucity of literature evaluating injury prevention in children’s (U14) soccer. Injury rates in children’s soccer range from moderate to high when compared with those in other sports 17,21 but are 3 to 7 times lower when compared with those in adult elite soccer. 2,7,24 Added to the incidence, the severity of injuries also increases during maturation. 7 Injury types seem to be more or less similar between children and youth players, as most of the injuries are classified as contusions, sprains, and strains. 6,24 Previous injuries seem to be a significant risk factor for both reinjuries and new injuries in the youth and adult settings. 3,12,14,16
Several high-quality randomized controlled trials (RCTs) have shown that neuromuscular training (NMT) can prevent lower extremity (LE) injuries in youth and adult soccer 3,10,15,25 –27 and in other team sports. 18,20 However, the number of injury prevention studies in soccer players younger than 14 years of age is very limited. To our knowledge, only 2 previous studies have investigated the effects of a specific NMT warm-up to prevent injuries in children’s soccer (ages 7-12 and 7-14 years, respectively). 23,28 These studies used the International Football Federation (FIFA) targeted injury prevention program for children (FIFA 11+ Kids) and reported 48% 23 and 50% 28 lower overall injury incidence rates in the intervention groups compared with the control groups having their standard-of-practice warm-up.
Considering the little knowledge available on the effectiveness of injury prevention in this young soccer population, our aim was to examine whether an NMT warm-up can reduce the risk of acute LE injuries in Finnish children (U11-U14) soccer players. Our hypothesis was that the NMT warm-up program would reduce the acute LE injury rate in youth soccer players.
Methods
Study Design and Participants
This study was a 2-armed cluster RCT. The study was approved by the ethics committee of our institution, and we followed and completed the CONSORT (Consolidated Standards of Reporting Trials) checklist. 1
The Sami Hyypiä Academy (SHA) selects 20 competitive youth soccer clubs across Finland every other year to participate in a player development process. As part of this process, female and male youth soccer players (aged 9-14 years) participate in 2 monitoring events during the year.
We invited all 20 SHA soccer clubs (92 teams; n = 1643 players) to participate in this study, and all clubs and teams agreed. Every player who was an official member of the participating team was eligible to enter the study. Informed consent from each player and his or her parent or legal guardian was required for final participation in the study.
A total of 1424 players agreed to participate. Of these, 6 players were excluded for having an ongoing injury before the study onset that prevented them from participating in team practices and games. Of the 1418 players entering the study, 15 players who stopped playing on the participating teams before the follow-up were excluded from the analysis. A total of 98 players (7%) withdrew from participation during the study. Data from these players were included in the analyses for the time they participated. Thus, the final sample consisted of 1403 players (673 in the intervention group, 730 in the control group). The flow of participants through the study following the CONSORT guidelines is shown in Figure 1.

CONSORT (Consolidated Standards of Reporting Trials) flowchart.
The randomization of participating clubs into intervention and control groups was performed by a statistician who had no further involvement in the study. Twenty clubs from 13 cities were randomized into either an intervention or a control group with the home city of the club as the unit of randomization: all clubs from the same city were assigned to the same group. Cities with several clubs (n = 1), with 2 clubs (n = 4), and with only 1 club (n = 8) were allocated in different randomization blocks. These 3 blocks were randomized separately into 2 groups with the condition that the number of clubs would be even (10 clubs each). Both groups were given a computer-generated random number, and the group with the greater number was assigned as the intervention group following the concealment-of-allocation principle.
Intervention
The intervention took place in 2015 between January and June (20 weeks). Coaches from the intervention group attended a prestudy workshop (3-hour duration) led by the research team (January 2015) at which they were introduced to the NMT warm-up program and data collection methods. In addition, each coach received a tablet computer with filmed demonstrations of the exercises and a PDF booklet detailing how to complete individual exercises in team practices. Components of the NMT warm-up were derived from an NMT program previously implemented and tested in floorball, 20 a team sport containing similarities to soccer in movement patterns. The NMT warm-up consisted of 7 different exercises with progression and variations of diverse difficulty focusing on the players’ motor skills and movement quality (Appendix Figure A1). The teams in the intervention group were asked to substitute their standard warm-up with the NMT warm-up 2 to 3 times per week (20 minutes each). Teams in the control group attended a prestudy meeting (1 hour) led by the research team (January 2015) at which they were introduced to the data collection methods and were asked to continue their usual warm-up routines during the study period.
During the intervention, the research team members visited each intervention team 2 to 3 times to support and help coaches with the intervention training and to facilitate proper technique and progress of the NMT warm-up exercises. In addition, unannounced checkups were conducted at the control clubs for evaluating the warm-up routines during the study period. After the study, the control clubs received the same coach workshop and NMT warm-up program as the intervention clubs did.
Outcome Measures
The primary outcome measure was an acute soccer-related LE injury. The secondary outcome measure was an acute noncontact soccer-related LE injury.
The definition of injury used in this study was according to Fuller and colleagues 8 : any physical complaint sustained by a player that resulted from soccer training or playing, irrespective of the need for medical attention or time loss from soccer activities. This sensitive definition was chosen to cover the whole extent of the injury problem in a youth population. Players were regarded as injured until they could fully train and play soccer normally. Injury site was categorized following the same consensus methdology. 8
The severity of an injury was defined as the number of days injured (time loss from fully training and playing): slight (0 days), minor (1-3 days), mild (4-7 days), moderate (8-28 days), severe (>28 days), or career ending (injury causing the player to stop playing soccer totally or forcing the player to play at a lower level) injury. 8
Data Collection
The baseline player monitoring events for the 92 participating teams were organized by the SHA within a time frame of 5 months (September to January). Before their teams' event, the players together with their parents or guardians completed a baseline questionnaire including details about athlete characteristics (eg, age and sex).
Exposure hours were recorded separately for practices and games. The players were asked to report their weekly practice and game hours once per month. These reports were incomplete, and therefore some estimations had to be made. Teams' mean practice hours were used as individual exposure and imputed for participants missing training exposure data entirely. The time of exposure to soccer games was calculated for entire teams. The total number of games played by each team was collected by the SHA for winter (January to March) and from the Finnish Football Association for the competitive season (April to June). Game exposure was calculated using standard game durations (20-80 minutes) for each age group and number of players on the field (8-11 players). 8
For injury reports, the players’ parents or guardians received a short message service text regarding possible injuries each follow-up week: Has your child had any musculoskeletal complaint or injuries during the previous 7 days (yes/no)? After each new injury, a physical therapist involved in the study interviewed the injured player or his and her guardian over the telephone using a structured questionnaire. Four blinded physical therapists were responsible for the injury data collection.
The coaches in the intervention group recorded their teams' NMT warm-up sessions (date and duration). After the follow-up, the coaches in the control group completed a questionnaire concerning their teams’ possible injury prevention strategies during the study period.
Power Calculation and Statistical Analysis
The sample size was based on a cross-sectional survey conducted during the previous SHA season (pilot study; n = 1400) showing an average seasonal incidence of acute LE injuries among young soccer players. Our power calculation for the cluster RCT was based on the assumption that we would detect at least a 20% reduction 3,25 in the incidence of acute LE injuries from 0.69 injuries in 20 weeks per person in the control group to 0.55 per person in the intervention group. We set the statistical power to 0.80, the significance level to .05, and the coefficient of variation of incidence rate between clusters (at club level) to 0.05. Thus, we estimated that we would need to recruit a minimum of 1380 players from 20 clubs for the entire study.
Statistical analyses were performed using Stata statistical software Version 15.0 (StataCorp). The outcome variable was set as the incidence of injuries per 1000 hours of exposure (team practices and games). Because of overdispersion, we chose to explain this count variable by negative binomial regression instead of Poisson regression. Intragroup correlation among players in the same club was taken into account by calculating cluster-robust SEs.
Incidence rates were defined as the number of injuries within the group per 1000 hours of soccer practice and games. From these incidence rates, we derived incidence rate ratios (IRRs) and 95% CIs to examine differences between groups. Adjustments were made by age and sex. Analyses were performed by the intention-to-treat principle: all eligible players who were enrolled in study clubs at the start of follow-up were included in the analysis and analyzed according to the group to which they were originally assigned. Both statisticians and the first author (M.H.) performing the analyses were blinded.
Results
Player Characteristics and Response Rate
The player characteristics for the intervention and study groups are provided in Table 1. Mean weekly exposure hours in practice and games were 5.44 in the intervention group and 4.45 in the control group (Table 1).
Characteristics of Players Receiving Neuromuscular Training Warm-up (Intervention) and Usual Training (Control)
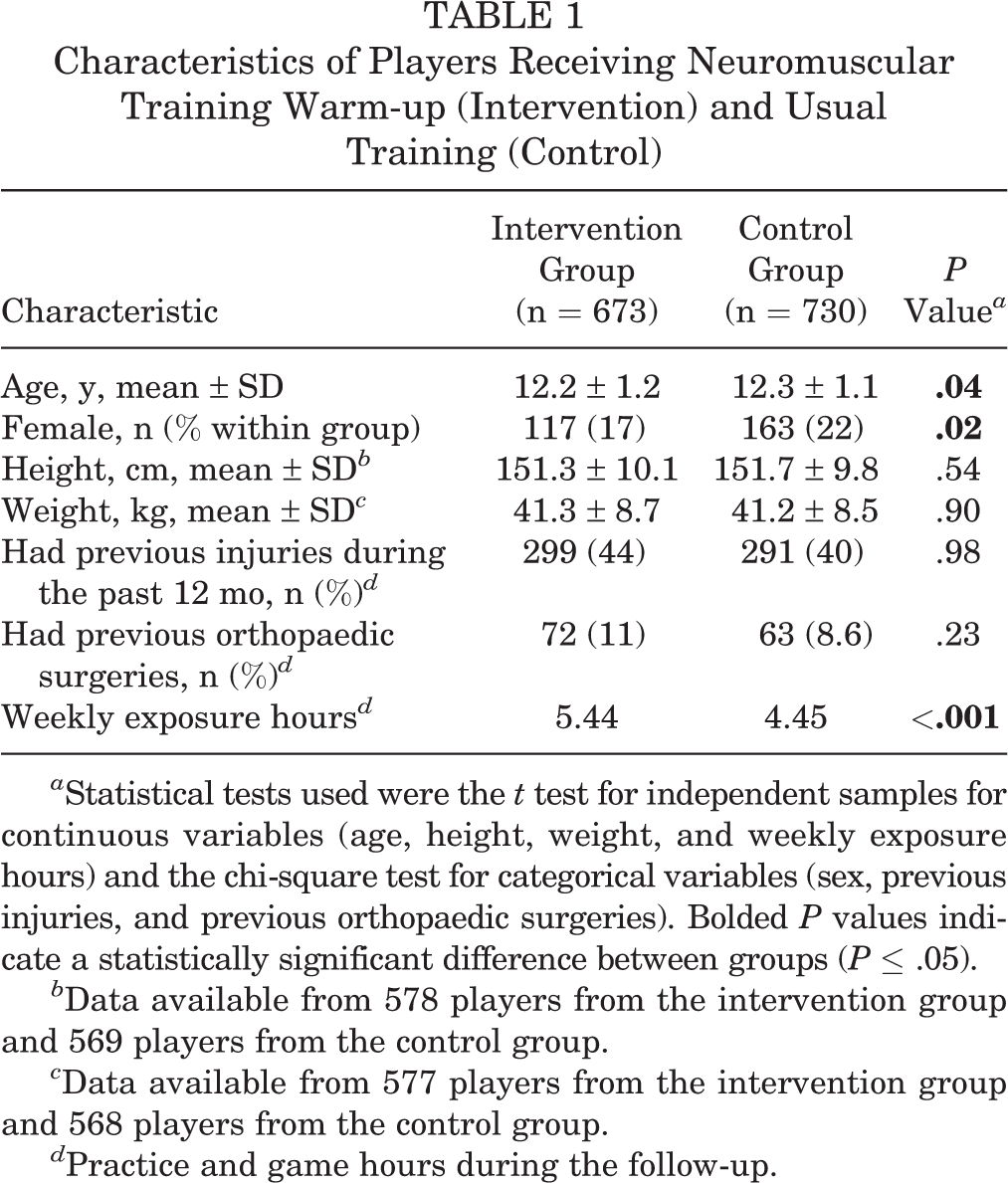
a Statistical tests used were the t test for independent samples for continuous variables (age, height, weight, and weekly exposure hours) and the chi-square test for categorical variables (sex, previous injuries, and previous orthopaedic surgeries). Bolded P values indicate a statistically significant difference between groups (P ≤ .05).
b Data available from 578 players from the intervention group and 569 players from the control group.
c Data available from 577 players from the intervention group and 568 players from the control group.
d Practice and game hours during the follow-up.
The average response rate for the 20 short message service messages was 95% (96% and 95% in the intervention and control groups, respectively). We received responses from 73% of the players’ parents or guardians each week; 95% responded 15 times or more.
Injury Incidence
During the study period, we recorded a total of 794 acute injuries for 541 individual players. Of these, 17 injuries involved the head/neck; 62, the upper extremities; 59, the trunk; and 656, the LEs. The incidence per 1000 hours of exposure of all acute LE injuries was 4.4 in the intervention group and 5.5 in the control group (unadjusted IRR, 0.81 [95% CI, 0.63-1.03]; adjusted IRR, 0.82 [95% CI, 0.64-1.04]) (Table 2).
Results of the Negative Binomial Regression Analysis of Acute Lower Extremity Injuries Overall and by Sex a
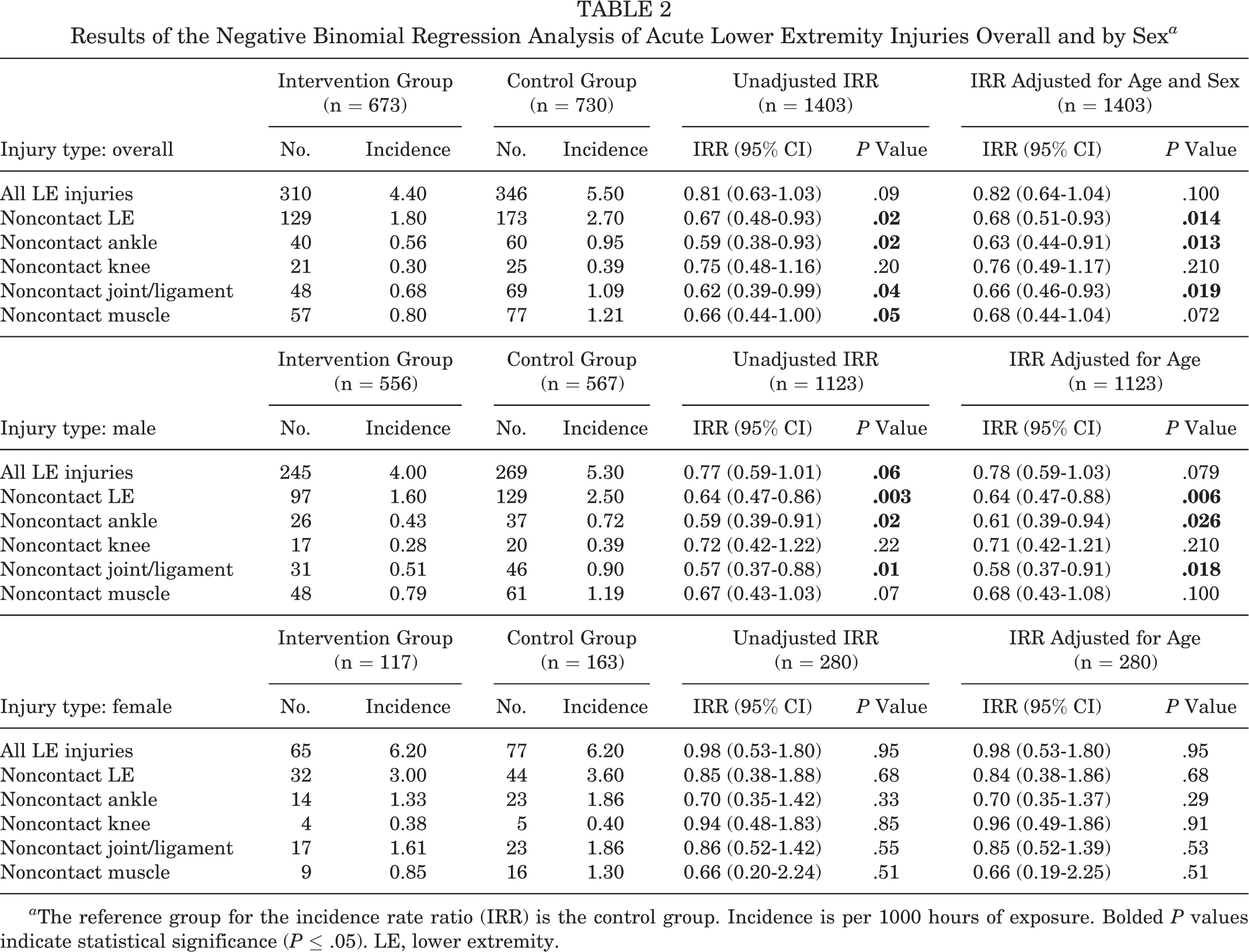
a The reference group for the incidence rate ratio (IRR) is the control group. Incidence is per 1000 hours of exposure. Bolded P values indicate statistical significance (P ≤ .05). LE, lower extremity.
Noncontact Injuries
Significantly fewer acute noncontact LE injuries occurred in the intervention group: the injury incidence rates were 1.8 and 2.7 per 1000 hours of exposure in the intervention and control groups, respectively (unadjusted IRR, 0.67 [95% CI, 0.48-0.93]; adjusted IRR, 0.68 [95% CI, 0.51-0.93]). Significant reductions in the incidence rates were also seen in the subanalyses of acute noncontact injuries, and the margins were greatest in joint/ligament injuries (by 38% in the unadjusted model) and in ankle injuries (41%) (Table 2). There were no differences in the incidence of contact LE injuries between groups (Appendix Table A1).
In the sex subgroup analyses, significant differences in the incidence rate reduction for boys were seen for the intervention group in all acute noncontact LE injuries as well as in ankle and joint/ligament injuries. No differences in the incidence rates were seen in the girls (Table 2).
Injury Severity
The number of injuries was too small for analyzing each severity group separately. Most acute LE injuries resulted in a time loss of between 0 and 7 days from soccer (n = 478; 73%), and the patterns of injury severity did not differ between the groups. Of the acute noncontact injuries, a total of 199 (66%) caused a time loss of between 0 and 7 days. The incidence of acute noncontact LE injuries resulting in ≤7 days of time loss was smaller in the intervention group compared with the control group (unadjusted IRR, 0.66 [95% CI, 0.45-0.97]; adjusted IRR, 0.67 [95% CI, 0.47-0.96]).
Team Adherence
The average number of NMT warm-up sessions was 1.7 per week in a team throughout follow-up. On an average follow-up week, 63% of the teams conducted the NMT warm-up at least twice (Table 3). Adherence to the NMT warm-up was higher in January than late in the study period. Almost all (95%) of the teams conducted 1 or more sessions during more than 75% of the weeks. The mean session length was 25 minutes (range, 10-70 minutes).
Adherence to the Neuromuscular Training Warm-up Program a
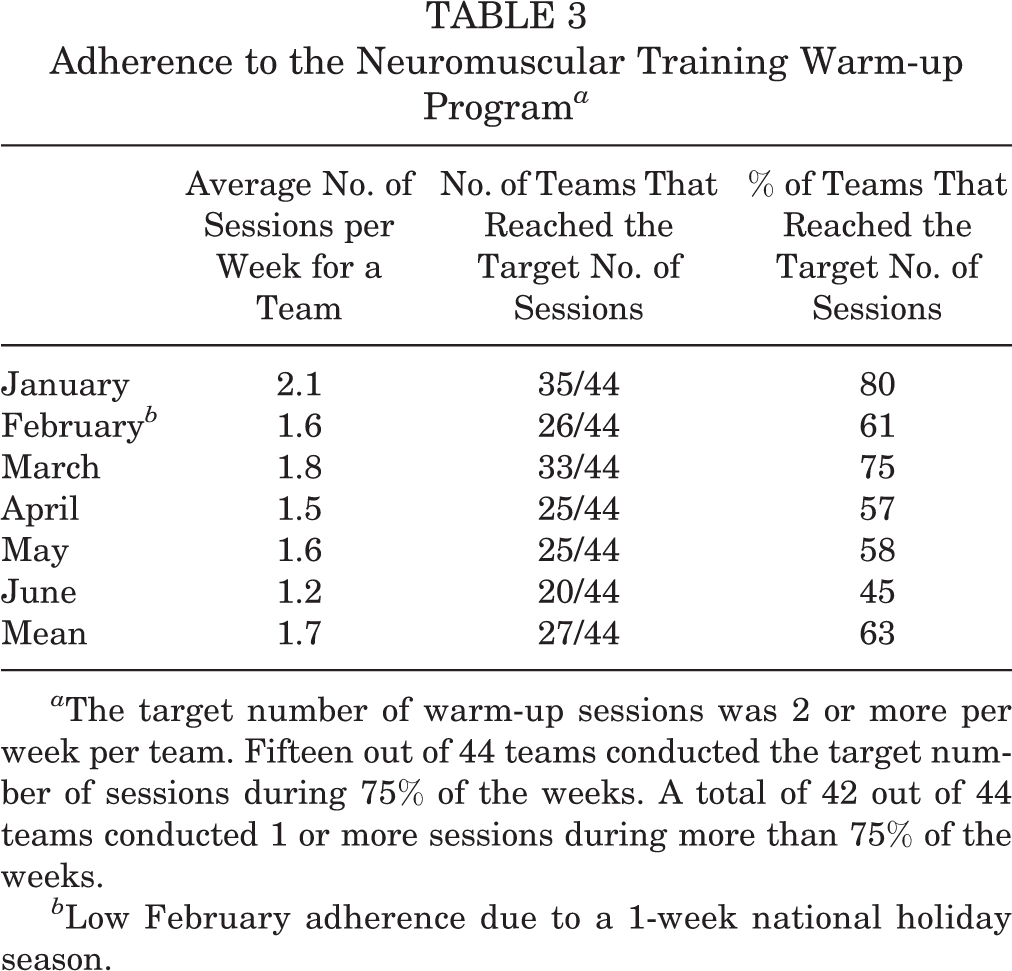
a The target number of warm-up sessions was 2 or more per week per team. Fifteen out of 44 teams conducted the target number of sessions during 75% of the weeks. A total of 42 out of 44 teams conducted 1 or more sessions during more than 75% of the weeks.
b Low February adherence due to a 1-week national holiday season.
A total of 34 of 48 teams (71%) in the control group responded to the questionnaire considering injury preventive measures during the study period. A total of 25 teams (74% out of all answers) reported having conducted some sort of weekly injury prevention strategy bearing similarity to the NMT warm-up examined in this study. In their weekly training, most control teams included planks (94% of the teams who answered), single-leg squats and/or lunges (82%), and single-leg jumps (82%), while hip muscle strength training was less popular (41%).
Discussion
Main Findings
In this trial, we examined the effects of an NMT warm-up on the incidence of acute LE injuries in a large cohort (n = 1403) of 9- to 14-year-old children playing soccer competitively. For the main outcome of all acute LE injuries, no statistically significant between-group difference was seen. The most important finding in our study was that the incidence of acute noncontact LE injuries was reduced by 32% in the intervention group compared with the control group. Statistically and clinically significant reductions in the injury incidence between the 2 groups were also seen in many subanalyses of acute noncontact injuries, most importantly in ankle injuries and joint/ligament injuries.
Currently, a limited number of studies have investigated injury prevention in children’s soccer. In recent studies, an NMT warm-up similar to ours reduced the overall injury risk in the intervention group by 48% 23 and 50% 28 among 7- to 12-year-old and 7- to 14-year-old soccer players. In an older age group (13- to 18-year-old players), other researchers have observed nonsignificant decreases of 17% to 32% in the risk for overall LE injuries. 3,26,26 In these earlier studies, the longer follow-up period (range, 4-9 months) might explain the more conclusive results compared with our study.
We observed that the intervention group had more training hours compared with the control group. Although we instructed them to include the NMT warm-up during usual practice hours, the execution in some of the intervention clubs might have resulted in an increase in training exposure. This difference in exposure should be addressed as a confounding factor in the interpretation of the results from this study: increased exposure might decrease the effect of the intervention on injury risk seen in the study, although exposure hours were taken into account in the analysis.
The awareness of injury prevention has also increased recently, and some NMT means were already in practice on a regular basis in youth soccer; this “contamination” makes it more difficult to point out differences. Unfortunately, a national knee injury prevention program led by the Finnish Football Association took place at the time of our study, and some control groups took part in it.
The type and severity of injuries we observed were in concordance with previous research. 6,24 The injuries were mostly classified as mild, as expected when studying a population this young. Severe injuries, such as tears of the anterior cruciate ligament of the knee, were absent. In line with findings in an age-comparable Norwegian soccer cohort, 7 the more severe injuries seem not to come into the picture until the intensity and speed of play increases during maturation toward adulthood.
Strengths and Limitations of the Study
The studied intervention was operated by the teams’ own coaches in their everyday practice and not by study personnel. Therefore, the studied NMT warm-up seems to be applicable for easy implementation in children’s soccer. The sample studied was large and representative of 9- to 14-year-old Finnish children playing competitive soccer. Recruited players were adherent in answering the weekly injury questionnaire, and the withdrawal rate was low. Both boys and girls were represented in the study population, and players in the study were recruited from both big clubs in big cities and smaller clubs in the periphery of Finland.
A limitation of the study was different recording methods for practice and game exposure. Players’ practice hours were collected by the SHA (web-based player diary). Game exposure was calculated for entire teams based on the number of games played by the team. Thus, training and game exposure data were not fully compatible together.
The adherence of the teams to the NMT warm-up toward the end of the follow-up was inadequate, as the adherence decreased from 80% in January to 45% in June. The same pattern of decreasing adherence has been witnessed in earlier studies too, 11,25 and research on the effective implementation of injury prevention programs is called for in the future.
We did not allow research team members to monitor and control the intervention training on a regular basis. Only 2 to 3 random unannounced checkups were conducted for each club. Thus, adherence to the intervention was determined largely by each team's coach only referring to real-life settings. We hypothesize that with a higher adherence of the participating teams, this training program would have become more effective concerning the main outcome measure of the study, the incidence of the overall acute LE injuries. Earlier research has reported lower injury incidence among more adherent participants to NMT intervention measures in youth soccer and floorball. 11,20,26
Finally, the number of female participants was too low to point out differences in female-only analyses, and no conclusions can be drawn on between-sex differences based on the results from this study. Further research in U14 female youth soccer on the efficacy of NMT in injury prevention is warranted.
Conclusion
The NMT warm-up operated by team coaches was effective in preventing acute noncontact LE injuries in children’s soccer, although no difference was seen in the overall acute LE injury incidence. However, the results of this study advocate for the beneficial effect of the NMT warm-up in reducing injury risk in children’s soccer. We encourage soccer coaches and health care professionals to take grassroots-level action in the use of NMT warm-up methods.
Footnotes
Acknowledgment
The authors acknowledge Sami Hyypiä Academy’s support of this project and thank all players, guardians, coaches, study physical therapists, and statisticians for their contribution to the study.
Final revision submitted January 20, 2021; accepted February 16, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was financially supported by the Finnish Ministry of Education and Culture, by the Competitive State Research Financing of the Expert Responsibility area of Tampere University Hospital, and by the Palloilu Säätiö, Tammela, Finland. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the ethics committee of Pirkanmaa Hospital District (ETL-code R13110).
Appendix
Contact Injuries by Injury Site a

| Intervention Group (n = 673) | Control Group (n = 730) | Unadjusted IRR (n = 1403) | IRR Adjusted for Age and Sex (n = 1403) | |||||
|---|---|---|---|---|---|---|---|---|
| No. | Incidence | No. | Incidence | IRR (95% CI) | P Value | IRR (95% CI) | P Value | |
| Hip/groin | 2 | 0.03 | 4 | 0.1 | 0.45 (0.10-1.96) | .29 | 0.43 (0.10-1.86) | .26 |
| Thigh | 27 | 0.4 | 18 | 0.3 | 1.35 (0.68-2.70) | .39 | 1.38 (0.69-2.77) | .37 |
| Knee | 40 | 0.6 | 45 | 0.7 | 0.79 (0.49-1.29) | .35 | 0.80 (0.49-1.32) | .39 |
| Shin/calf/Achilles tendon | 20 | 0.3 | 19 | 0.3 | 0.94 (0.46-1.90) | .86 | 0.94 (0.48-1.86) | .87 |
| Ankle | 56 | 0.8 | 61 | 1.0 | 0.82 (0.53-1.26) | .37 | 0.83 (0.54-1.27) | .39 |
| Foot/toe | 36 | 0.5 | 26 | 0.4 | 1.25 (0.71-2.20) | .44 | 1.22 (0.71-2.10) | .48 |
| Total | 181 | 2.5 | 173 | 2.7 | 0.94 (0.70-1.28) | .71 | 0.95 (0.70-1.29) | .75 |
a Incidence is per 1000 hours of exposure. IRR, incidence rate ratio.