
Abstract
Background:
Graft-tunnel mismatch is an avoidable complication in anterior cruciate ligament (ACL) reconstruction. Patient height and sex may be predictors of patellar tendon length (PTL) and intra-articular ACL length (IAL). Understanding these relationships may assist in reducing graft-tunnel mismatch during ACL reconstruction with bone–patellar tendon–bone (BTB) autograft.
Purpose:
To determine the association of patient height and sex with PTL and IAL.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Magnetic resonance imaging (MRI) studies were obtained on the healthy knees of 100 male and 100 female patients. Patients with prior surgery, open physes, significant degenerative changes, ACL rupture, or extensor mechanism injury were excluded. Three independent readers measured PTL, IAL, and Caton-Deschamps Index (CDI) on MRI. Bivariate and linear regression analysis was performed to detect the association of anthropometric data with anatomic parameters measured on MRI studies.
Results:
The mean age and body mass index were not significantly different between the male and female patients; however, male patients were significantly taller than female patients (1.75 vs 1.72 m, respectively; P < .001). There was a substantial agreement between the 3 readers for all parameters (κ > 0.75). Overall, female patients had significantly longer PTL (47.38 vs 43.92 mm), higher CDI (1.146 vs 1.071), and shorter IAL (33.05 vs 34.39 mm) (P < .001 for all). Results of the linear regression analysis demonstrated that both height and female sex were predictive of longer PTL. Further, height was independently predictive of IAL but sex was not.
Conclusion:
PTL was correlated more with patient sex than height. IAL was also correlated with patient sex. Longer BTB grafts are expected to be harvested in female patients compared with male patients of the same height despite shorter IAL. These associations should be considered during BTB ACL reconstruction to minimize graft-tunnel mismatch.
Anterior cruciate ligament (ACL) reconstruction using bone–patellar tendon–bone (BTB) autograft is a reliable procedure with consistent outcomes and low rerupture rates. 7,10 Tunnel placement error is the most common reason for failure of this procedure. 22 Whether transtibial, modified transtibial, or anteromedial drilling is performed, the final graft placement, and therefore function is determined by tunnel placement. Tunnel position is determined by the combined coronal and sagittal angles chosen for the tibial guide, the width of the tibia, the location of tunnel entry on the outer cortex of the tibia, and portal placement. Graft-tunnel mismatch is when the tendon graft between bone plugs is too short or too long, resulting in the tibial bone plugs either sinking deep within or, more commonly, protruding out of the tibial tunnel aperture, thus compromising graft fixation. 2 Graft-tunnel mismatch occurs in 13% to 26% of ACL reconstructions and has been associated with mechanical malfunction, widening of the bone tunnels, impingement, and laxity. 17 Optimal tibial tunnel placement must take into account graft length as well as tunnel position in order to avoid graft-tunnel mismatch.
It has been recommended that an optimal BTB graft length should result in the tibial-side bone plug being fully within the tibial tunnel with the distal tip flush with the tunnel’s outer cortical aperture. 13 Graft-tunnel mismatch can potentially be avoided by adjusting either graft length 12 or tunnel length via position. 13,14,16 A broad range of tibial tunnel locations was reported using a single technique, which likely varies even more when taking into account varied drilling techniques. 26
Multiple techniques have been described to avoid graft-tunnel mismatch. 8,13,18,21,24 For example, Miller and Hinkin 13 described an “N+7” technique in which 7 mm is added to the soft tissue graft length to yield the drilling angle on the tibial guide. Meijer et al 12 reported using the Blumensaat line plus 20 mm to estimate the patellar tendon length (PTL). Current BTB autograft harvest methods typically utilize a 10 × 25–mm tibial bone plug and a 10 × 20--mm patellar bone plug, which can be adjusted if needed to account for tendon length mismatch. 4 The angle used to make the tibial tunnel can also alter tunnel length. However, the optimal method to avoid graft-tunnel mismatch is to anticipate extremes of length and plan tunnels accordingly.
Previous studies have shown that patient height is associated with the lengths of both intra-articular ACL 2,9 and patellar tendon. 5 A long patellar tendon has been associated with graft-tunnel mismatch. 6 However, the lengths of the patellar tendon and intra-articular ACL with respect to patient sex have not been described.
The purpose of this study was to examine the relationship of patient height and sex on PTL and IAL. Patient height, sex, and PTL can all be quantified preoperatively, enabling preoperative graft length calculation. We hypothesized that both sex and height are independent predictors of PTL as well as IAL.
Methods
Institutional review board approval was obtained for this study. Knee MRI studies performed between 2014 and 2019 were extracted from the electronic medical record of a large academic institution. Knee MRI studies obtained for any reason were reviewed. Patients were excluded if an ACL tear was present; prior ACL reconstruction or any prior surgery was evident; and if extensor mechanism injury, prior repair, or significant degenerative changes were noted. Patients with open physes or those patients aged over 40 years were excluded so a patient cohort most commonly undergoing ACL reconstruction without anatomical variation from subtle developmental (open physes) or degenerative (age over 40 years) processes could be studied. Anthropometric data, specifically height and weight, were obtained from the medical record. A total of 100 male and 100 female MRI studies were ultimately included in this study. Three readers (2 sports fellows [A.L.C., D.Y.], 1 fellowship-trained attending sports medicine surgeon [C.A.U.]) measured the following parameters on all MRI studies: PTL, IAL, CDI, and global International Cartilage Regeneration & Joint Preservation Society (ICRS) grade.
MRI Measurements
PTL was measured along the posterior aspect of the patellar tendon from the inferior-most patellar origin to proximal-most tubercle insertion. This was performed on midsagittal T1-weighted images as described. 3 The CDI measures patellar height and has been verified on MRI. This was measured on the sagittal cut in which the maximum length of the patellar articular cartilage was visible. 15 The IAL was also measured on sagittal series. The clearest cut showing both the tibial and the femoral insertion sites was chosen, and the distance between the midportion of the insertion sites was measured from bone to bone in the midsection of the ligament. 1,25 These measurements are demonstrated in Figure 1.
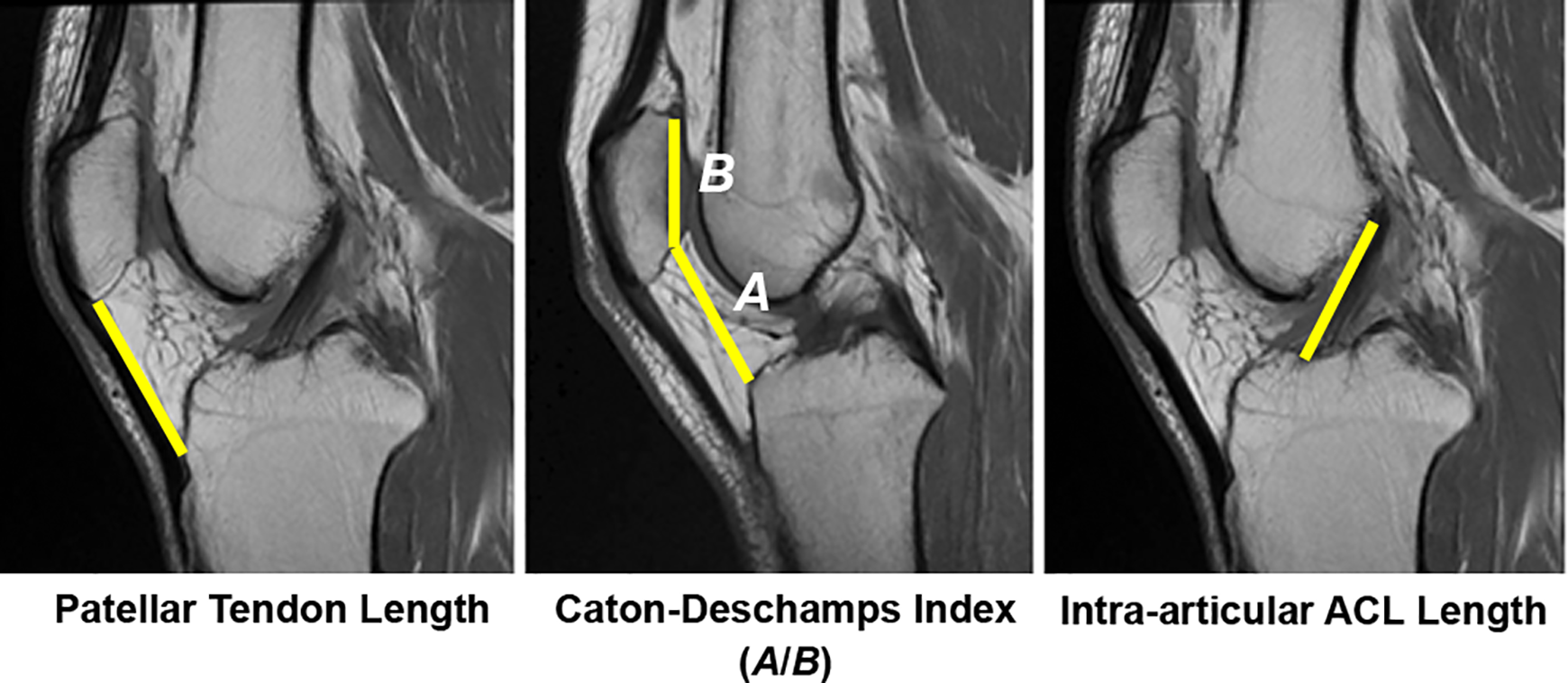
Example of patellar tendon length, Caton-Deschamps Index (CDI), and intra-articular ACL length measurements performed on T1-weighted sagittal magnetic resonance imaging. Yellow lines refer to parameters measured on MRI. CDI is calculated as the quotient A/B, in which A = distance between proximal tibia and inferior patella and B = patellar articular surface length. ACL, anterior cruciate ligament.
Statistical Analysis
An a priori power analysis was performed. To detect a 3-mm difference in PTL between groups (alpha, .05; beta, 0.2; power, 0.8), 44 patients were required of each sex. Reliability analysis was performed by determining the intraclass correlation coefficient using a 2-way random effects model of average scores to assess the agreement between 3 observers (A.L.C., D.Y., C.A.U.) in measuring the radiographic parameters of each patient. Bivariate analysis was performed using a student t test for parametric variables and a Mann-Whitney U test for nonparametric variables. Normality was determined with a Shapiro-Wilk test. Linear regression analysis was performed to assess the independent effects of height and sex on PTL and IAL. Statistical significance was set at P < .05 or in the case of multiple comparisons, a Bonferroni corrected P < .0125. Effect size was reported as Cohen d. Statistics were performed using R Version 3.5.1 (R Foundation for Statistical Computing).
Results
Knee MRI studies of 100 female and 100 male patients were reviewed. The mean age was not significantly different between groups (women, 23.9 years; men, 24.4 years; P = .437). The mean body mass index was not significantly different between groups (women, 24.1 kg/m2; men 24.7 kg/m2; P = .309). There was a significant difference in height between female and male patients (1.72 vs 1.75 m; mean difference, -0.035 mm ± 0.01 [95% CI, -0.055 to -0.016]; P < .001). The average ICRS score was less than 1 in both female and male patients (mean difference, 0.063 ± 0.060 [95% CI, -0.055 to 0.182]; P = .264).
Reliability Analysis
There was, at minimum, substantial agreement between the 3 raters (A.L.C., D.Y., C.A.U.) for PTL (κ = 0.848; P = .003), IAL (κ = 0.754; P < .001), and CD (κ = 0.791; P < .001). These are outlined in Appendix Table A1.
Bivariate Analysis
On bivariate analysis, PTL was significantly longer in female than in male patients (mean difference, 3.468 mm ± 0.74 [95% CI, 1.988-4.948]; P < .001). The mean CDI was significantly higher in female than in male patients (0.076 ± 0.019 [95% CI, 0.039-0.113]; P < .001). Conversely, IAL was significantly shorter in female than in male patients (mean difference, -1.337 mm [95% CI, -2.098 to -0.576]; P < .001). These results are displayed in Table 1.
Bivariate Analysis Results of MRI Measurements Including Cohen da

a Measurements are presented as mean ± SD. ACL, anterior cruciate ligament; CDI, Caton-Deschamps Index; IAL, intra-articular ACL length; MRI, magnetic resonance imaging; PTL, patellar tendon length.
Effect of Sex on PTL and IAL
A linear regression was performed using the Enter method, and results indicated that height and sex had a significant effect on PTL (F = 14.01; P < .001; R 2 = 0.125; R 2 adj = 0.116). The analysis showed that height significantly predicted PTL (unstandardized β = 13.274 [95% CI, 2.677-23.871]; standardized β = 0.170; t = 2.470; P =.014) as did female sex (unstandardized β = 3.938 [95% CI, 2.429-5.446]; standardized β = 0.354; t = 5.148; P < .001).
Height was independently predictive of IAL (F = 39.32; P < .001, R 2 = 0.285; R 2 adj = 0.278), but sex was not. The analysis results showed that height correlated positively with IAL (unstandardized β = 19.368 [95% CI, 14.551-24.186]; t = 7.929; P < .001), but sex had no significant correlation (unstandardized β = -0.652 [95% CI, -1.338 to 0.033]; t = -1.876; P = .062).
Analysis results to determine whether the data met the assumption of collinearity indicated that multicollinearity was not a confounder (tolerance = 0.938; variance inflammation factor = 1.066). The histogram of standardized residuals indicated that the data contained approximately normally distributed errors, as did the normal Q-Q plot of standardized residuals.
Discussion
Increasing height has been associated with greater IAL. 2,9 A previous study by Ko et al 9 on avoiding BTB allograft mismatch found a strong positive correlation between individual height and intra-articular length of the ACL with in situ measurements during surgery. Another MRI measurement study by Goldstein et al 5 on BTB allograft mismatch reported significantly shorter (3 mm) PTL in women compared with men; however, the mean height per group was not reported and analysis of the reported data suggested shorter height. Therefore, taller patients will both yield longer BTB grafts and require longer grafts to match longer IALs.
This is the first study to examine the association of sex with PTL and IAL. In the multivariate regressions adjusted for height, female sex was associated with a greater PTL but not a greater IAL. In fact, the current study suggests that, based on standardized beta coefficients, sex is a stronger predictor of PTL than height. This comparison of men and women demonstrates that while shorter on average, women can be expected to have longer patellar tendons with shorter ACLs than men. These findings suggest that tibial tunnel planning cannot be performed based on height alone, but patient sex must also be taken into account.
Although it has not been established that women can be expected to have higher incidences of graft-tunnel mismatch, there are no studies directly comparing mismatch incidence between sexes. Overall, women have been reported to have higher rerupture rates, 11,20 laxity, 19 and worse clinical outcomes following ACL reconstruction. 23 This may be related to graft-tunnel mismatch. With a longer BTB autograft in a woman with a height of 1.70 meters (5’7”) compared with a man of the same height, yet smaller or similar IAL, the female knee is more likely to face graft-tunnel mismatch. Using a standardized angled guide to create the tibial tunnel in all individuals fails to acknowledge that the patellar tendon graft varies in length. Insufficient bone block present within the tibial tunnel may raise the risk of failure. Anticipating graft-tunnel mismatch may mitigate the failure risk that exists in women.
Although various techniques exist to avoid graft-tunnel mismatch, our findings highlight the importance of preoperative planning and challenge the surgeon to think about graft-tunnel mismatch.
Limitations
Selection bias is a limitation in this study, as all MRI studies were reviewed by the first author (A.L.C.) to determine if prior surgery was performed, arthritic grade too high, or other excluding factors were present, such as ACL rupture. MRI measurements are also a limitation: ACL is not a perfectly sagittal structure, and intra-articular length was measured on a sagittal plane image. However, as this study is a relative comparison between MRI studies in a standard plane and not an absolute quantification study, comparisons can still be made between sexes. Last, the differences identified between height and IAL on MRI were statistically significant but quite small (0.04 mm and 1.34 mm, respectively). Even with these small differences— that is, assuming that the female and male patients studied had similar height and similar IAL, the finding that the PTL is 3.47 mm longer in female patients is clinically significant in the context of 35 to 55 mm average tendon graft length in BTB ACL reconstruction. 16
Conclusion
These findings underline the importance of considering sex when planning ACL reconstruction with BTB autograft to avoid graft-tunnel mismatch. As longer grafts are likely to be harvested in a female patient compared with a male patient of the same stature, without greater IALs, there is a high risk of facing graft-tunnel mismatch in female patients specifically. Therefore, careful consideration for patient height and sex on BTB graft length should be recognized when establishing the tibial tunnel during ACL reconstruction.
Footnotes
Final revision submitted November 12, 2020; accepted December16, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.L.C. has received education payments from Arthrex and Micromed and grants from Arthrex. D.Y. has received hospitality payments from Medical Device Business Services. C.A.U. has received consulting fees and nonconsulting fees from Arthrex; hospitality payments from Arthrex; and education payments from Smith & Nephew. O.L. has received consulting fees from Arthrex and Linvatec; nonconsulting fees from Arthrex; education payments from Arthrex; and royalties from Linvatec. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Cedars-Sinai (Protocol ID: STUDY00000363).
Appendix
Results of Reliability Analysis a

| Kappa Coefficient | 95% CI | P Value | |
|---|---|---|---|
| Patellar tendon length | 0.848 | 0.349-0.941 | .003 |
| Intra-articular ACL length | 0.754 | 0.561-0.876 | <.001 |
| Caton-Deschamps Index | 0.791 | 0.612-0.876 | <.001 |
a ACL, anterior cruciate ligament.