
Abstract
Background:
Lateral meniscal deficiency increases the pivot shift in the knee, and although meniscal allograft transplantation (MAT) is a well-established procedure with satisfactory clinical results, biomechanical studies have failed to show whether this procedure is able to restore knee kinematics.
Purpose:
To assess, in vivo, the kinematic effect of lateral MAT in anterior cruciate ligament–intact knees, with a particular focus on the pivot-shift maneuver.
Study Design:
Controlled laboratory study.
Methods:
Enrolled in this study were 10 consecutive patients undergoing lateral MAT. A surgical navigation system was used to acquire and quantify the following variables: anterior-posterior displacement at 30° of flexion (AP30) and 90° of flexion (AP90), varus-valgus rotation at 0° of flexion (VV0) and 30° of flexion, and dynamic laxity on the pivot-shift test, which was determined through anterior displacement of the lateral tibial compartment (APlat) and posterior acceleration of the lateral tibial compartment during tibial reduction (ACC). Data from before and after MAT were compared.
Results:
From pre- to postoperatively, there was a significant decrease in tibial translation of 2.8 mm (43%; P = .005) for AP30 and 1.9 mm (38%; P = .018) for AP90 as well as a significant difference of 3.6° (64%; P = .001) for VV0. There was also a significant pre- to postoperative reduction in the pivot shift of 7.4 mm (39%; P = .021) for APlat and 302.9 mm/s2 (75%; P = .005) for ACC.
Conclusion:
Lateral MAT improved knee kinematic parameters at time zero after surgery; the biomechanical effect of MAT was particularly evident during the pivot-shift maneuver.
There has been growing interest over the past few years regarding the role of the menisci and meniscal tears on knee kinematics. 4,5,24,33 Current evidence suggests that medial and lateral menisci have unique roles in knee biomechanics: While the medial meniscus acts as a secondary restraint to anterior tibial translation, the lateral meniscus has important effects on dynamic laxity, showing that partial meniscectomy can produce loss of articular stability. 4 Specifically, several authors have demonstrated that a compromised lateral meniscus would produce a significant increase in the pivot-shift phenomenon in both anterior cruciate ligament (ACL)–intact and ACL-deficient knees. 8,23,24
In clinical practice, meniscal allograft transplantation (MAT) is a well-established surgical procedure that has demonstrated satisfactory results in terms of survival, clinical outcomes, return to sport, and efficacy in preventing or delaying osteoarthritic changes. 2,3,26,30,34 On the other hand, studies on the biomechanics of MAT have failed to show whether this procedure is able to restore intra-articular contact pressures and knee kinematics. 1,12,25,28 However, most of these studies are designed as finite element analyses or animal models, which do not resemble the correct human anatomy, or as cadaveric studies, which might not be as representative as in vivo clinical settings, although they have the advantage of an unrestricted number of tests and cutting protocols.
Therefore, this surgical navigation study aimed to assess the kinematic effect of lateral MAT in vivo, with a particular focus on the pivot-shift maneuver. The hypothesis was that the measured parameters would show decreased postoperative knee laxity after MAT.
Methods
Patient Selection
In this prospective case series, 10 consecutive ACL-intact patients undergoing isolated lateral MAT were enrolled in the study from August 2018 to October 2019. The inclusion criteria for eligibility were previous total/subtotal lateral meniscal removal, pain localized in the knee’s lateral compartment with Kellgren-Lawrence grade ≤2 osteoarthritis, and age ≥18 years. Exclusion criteria were previous removal of the medial meniscus, concomitant knee osteotomy, concomitant ligament reconstruction, concomitant cartilage procedures, and advanced osteoarthritis. The meniscal, ligamentous, and chondral statuses of the knee were investigated on preoperative magnetic resonance imaging and confirmed during arthroscopic surgery. This research study was approved by an institutional review board, and all of the enrolled patients signed informed consent forms prior to undergoing the surgical procedure.
Surgical Technique
All surgical procedures were performed by the senior author (S.Z.) at a single institution. Fresh-frozen (–80°C) nonirradiated and non–antigen matched allografts were used. The age criterion for donors was 15 to 35 years. Anthropometric parameters 10,29 were used to establish the correct size of the graft. Transplantation was performed arthroscopically using a transtibial tunnel technique, with soft tissue fixation but without bone plugs. The remnant of the native meniscus was removed up to the meniscal-capsular zone. A tibial tunnel aimed to the posterior horn insertion was prepared to secure the suture corresponding to the posterior meniscal horn to the anterior tibial cortex. The previously prepared graft was inserted into the joint with a Kelly clamp after passing a shuttle suture through the posterior tunnel. Pulling the shuttle suture, the graft was located correctly and fixed to the capsule with all-inside stitches (either FAST-FIX [Smith & Nephew] or TRUESPAN [DePuy Synthes]). The first suture was positioned at the junction between the posterior horn and body to immediately stabilize the graft in the correct position. The anterior horn of the graft was fixed through a second tunnel aimed toward the anterior horn insertion. Finally, the shuttle sutures were retrieved and tied to the tibial cortex to fix the graft’s horns (Figure 1). No outside-in fixation was performed. After checking for graft stability, the skin was closed, and a compressive bandage and full-extension brace were placed.
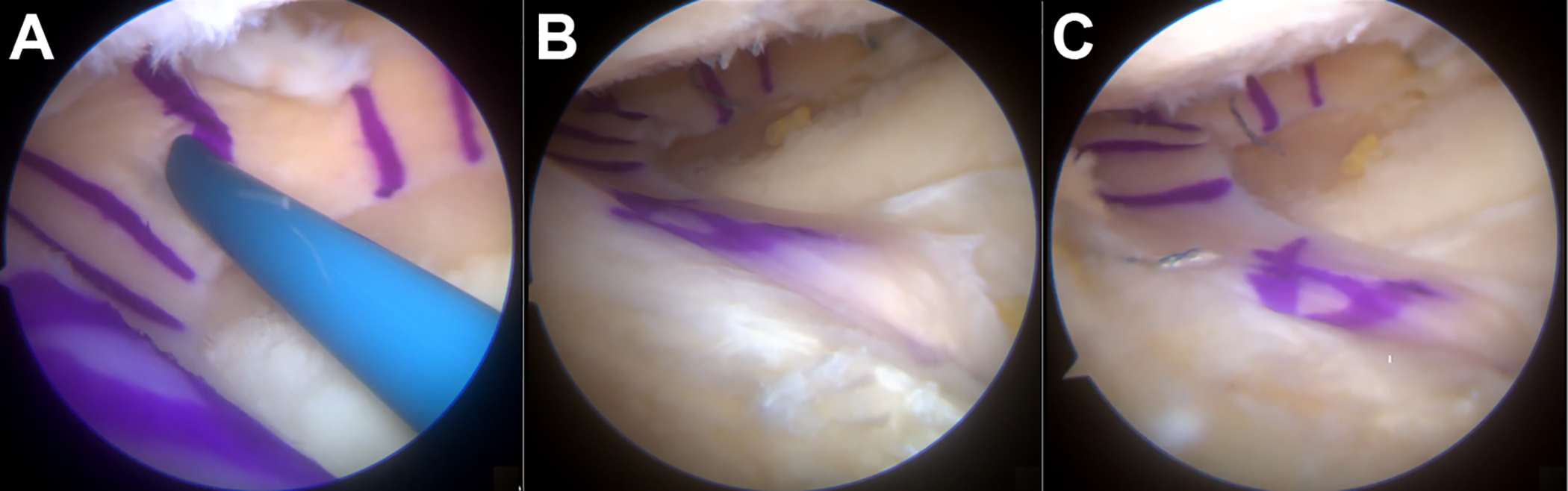
Arthroscopic images of lateral meniscal allograft transplantation with soft tissue fixation. (A) The allograft was fixed to the capsule with all-inside stitches. (B, C) The shuttle sutures were retrieved through the anterior and posterior tunnels and tied to the tibial cortex to fix the graft’s horns.
Testing Protocol
To acquire anatomic coordinates and kinematic data, a surgical navigation system was adopted (BLU-IGS; Orthokey), equipped with software specifically dedicated to intraoperative kinematic acquisition (KLEE; Orthokey). Such instrumentation includes the invasive use of cortical fixed optical trackers driven into the tibia and femur. The 3-dimensional accuracy of the surgical navigation system is 0.35 mm, as reported by the manufacturer. 31 The examination protocol was performed before MAT in the meniscus-deficient status and then after transplantation. Utilizing the method developed by Martelli et al, 20 the surgeon manually performed the following clinical kinematic tests at maximum force (Figure 2):
anterior-posterior displacement at 30° of flexion (AP30),
anterior-posterior displacement at 90° of flexion (AP90),
varus-valgus rotation at 0° of flexion (VV0),
varus-valgus rotation at 30° of flexion (VV30), and
pivot-shift test to assess dynamic laxity.

Intraoperative setup of the surgical navigation system.
A standardized technique of the pivot-shift test designed on the basis of the Galway and MacIntosh procedure was performed 7 and quantified, according to the literature, 19 through 2 different parameters: anterior displacement of the lateral tibial compartment (APlat) and posterior acceleration of the lateral tibial compartment during tibial reduction (ACC). Both these parameters have been shown to have a direct relation to clinical laxity. 14,18
The reliability of all laxity tests performed at maximum force was evaluated in previous studies. 20 During the entire set of tests, the examiner was the same and blinded to the quantitative results to avoid bias in data acquisition. Data were elaborated offline in MATLAB (MathWorks).
Statistical Analysis
The normal distribution of the data was verified by the Shapiro-Wilk test. Normally distributed continuous variables are presented as the mean ± SD, non-normally distributed continuous variables are presented as the median and interquartile range, and categorical variables are presented as the percentage. The Mann-Whitney U test was used to compare each group with one another. Differences between the groups were considered statistically significant if P < .05.
An a priori power analysis was performed based on the results of a similar study on fresh-frozen cadaveric specimens, 28 and considering a value of 5.1 mm after meniscectomy and 4.4 mm after MAT for anterior-posterior translation at 90° and hypothesizing an SD of 0.8 mm, at least 10 patients in each group were required to have a power of 80% and a type I error of .05. All statistical analyses were performed in MATLAB.
Results
A cohort of 10 patients (9 men and 1 woman), with a mean age of 35 ± 10 years, underwent navigated lateral MAT (Table 1). The mean time from previous lateral meniscectomy to MAT was 5.5 ± 5.5 years (range, 1-16 years). Pre- and postoperative kinematic data are presented in Table 2.
Patient Demographics

Laxity Measurements a

a Data are presented as median (interquartile range). ACC, posterior acceleration of the lateral tibial compartment during tibial reduction; AP30, anterior-posterior displacement at 30° of flexion; AP90, anterior-posterior displacement at 90° of flexion; APlat, anterior displacement of the lateral tibial compartment; VV0, varus-valgus rotation at 0° of flexion; VV30, varus-valgus rotation at 30° of flexion.
Anterior-Posterior Displacement
Regarding both AP30 and AP90, a significant difference (P < .05) between pre- and postoperative values was found (Table 3 and Figure 3A). Specifically, for AP30, there was a significant laxity reduction of 2.8 mm (43%; P = .005) compared with preoperatively. A similar result was reported for AP90, with a significant reduction of 1.9 mm (38%; P = .018) (Table 3).
Preoperative to Postoperative Difference a

a Bolded P values represent statistically significant differences between groups (P < .05). ACC, posterior acceleration of the lateral tibial compartment during tibial reduction; AP30, anterior-posterior displacement at 30° of flexion; AP90, anterior-posterior displacement at 90° of flexion; APlat, anterior displacement of the lateral tibial compartment; VV0, varus-valgus rotation at 0° of flexion; VV30, varus-valgus rotation at 30° of flexion.
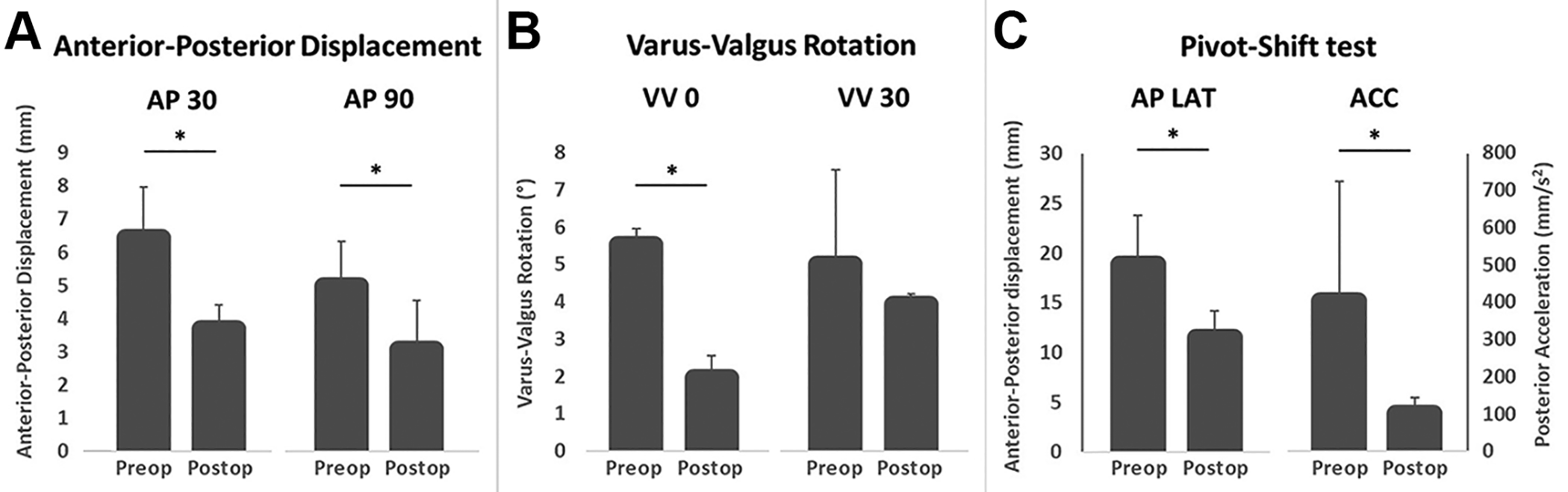
Pre- and postoperative (Preop and Postop) values for (A) anterior-posterior displacement at 30° (AP30) and 90° (AP90) of knee flexion, (B) varus-valgus rotation at 0° (VV0) and 30° (VV30) of knee flexion, and (C) dynamic laxity on the pivot-shift test evaluated through anterior displacement of the lateral tibial compartment (APlat) and posterior acceleration of the lateral tibial compartment during tibial reduction (ACC). *Statistically significant differences between pre- and postoperative values (P < .05).
Varus-Valgus Rotation
A significant difference was found for VV0 between pre- and postoperative values (P = .001) (Table 3 and Figure 3B).
Pivot-Shift Test
The pivot-shift test, used to assess dynamic laxity, showed significant differences between pre- and postoperative values (Table 3 and Figure 3C). There was a significant reduction of 7.4 mm (39%; P = .021) for APlat and 302.9 mm/s2 (75%; P = .005) for ACC.
Discussion
The main finding of the present study is that lateral MAT improved knee kinematics of the ACL-intact knee at time zero after surgery; the parameters of AP30, AP90, and VV0 as well as APlat and ACC during the pivot-shift maneuver were significantly improved postoperatively. To our knowledge, this is the first study to analyze the in vivo kinematics of MAT. Previously, the effect of lateral and medial MAT associated with ACL reconstruction was explored in a preliminary in vivo case report, the results of which suggested a synergistic role between MAT and the ACL in restoring knee kinematics; in particular, a clear laxity reduction was obtained after lateral MAT in AP30, AP90, VV0, and VV30. 33
The results of the current study confirmed the key role of the knee’s lateral compartment in controlling joint dynamic laxity, as reported in previous biomechanical studies. Moreover, the findings of the current study suggest that restoration of the lateral meniscus played a significant role in also controlling static laxity of the knee, as anterior-posterior translation parameters improved after lateral MAT.
The results of the present study are in only partial alignment with 2 recent studies by Novaretti et al 24,25 ; they investigated the effect of lateral meniscectomy and lateral MAT in 10 cadaveric knees. Their methodology was based on 3 loading protocols (simulated Lachman maneuver, simulated pivot shift, and simulated cutting/pivoting movement) applied in the intact state after meniscal removal and lateral MAT. Their results demonstrated that laxity increases progressively with meniscal removal and specifically that tibial rotation is significantly affected during a simulated pivot shift and cutting movements. Nevertheless, in contrast with the findings of the present study, they did not observe significant laxity reduction after MAT (neither with a bone block nor with a suture-only technique) on any simulated test. Instead, they found that lateral MAT can compensate for at least 50% to 60% of the load-bearing forces applied to the native meniscus. Similar results were reported by Brial et al 1 in a cadaveric study with simulated gait; they observed that lateral MAT is able to reduce the contact area and decrease peak stress in comparison with complete meniscectomy but not as much as the native meniscus.
One main difference to note is that the donors of specimens in the Novaretti et al 24,25 studies were significantly older (mean, 75 years) than the patients in this study (mean, 35 ± 10 years), and as stated by those authors, tissue degeneration and poor quality due to age might have caused some bias in their results. That said, one weak point that all these studies have in common is the evaluation at time zero that cannot account for in vivo changes observed postoperatively. Tissue healing and remodeling over time could affect the kinematics of MAT in unexpected ways: the graft could become firmly attached to the capsule, undergoing shrinkage, but it could also extrude to the articular periphery.
Indeed, graft extrusion has been already recognized as a common problem after MAT, occurring in about 50% of procedures and even shortly after surgery. 16 Some authors have conducted imaging studies that correlate the grade of meniscal extrusion with the surgical technique, obtaining controversial results. 6,11,21,22 Koh et al 13 demonstrated instead that lateral MAT was significantly more extruded than medial MAT at 3 years’ follow-up; this difference might be related to differences in the anatomic restraints of the medial and lateral compartments.
More importantly, Lee at al 15 demonstrated that graft sizing and mismatching of lateral MAT are positively correlated with the grade of extrusion soon after surgery. It is possible to speculate that the significant decrease in laxity observed after lateral MAT could be caused by nonperfect graft sizing, in particular oversizing, which fails to reproduce the anatomy as before meniscectomy. This overconstraint could be related to the consequent MAT extrusion, as reported by other authors, 27 caused by overstuffing of the lateral compartment. Nevertheless, it is worth noting that several studies did not find any correlation between MAT extrusion and clinical outcomes 9,17 ; therefore, it is not possible to delineate definitive results.
This study presents several limitations. First, when comparing this study to previous similar cadaveric studies with robot testing, it appears clear that it is not possible to reach the same level of measurement accuracy and number of acquisitions; moreover, the magnitude of the effect of soft tissue swelling from arthroscopic surgery and dissection on the kinematic measurements was not quantified, and the examiner was not blinded and may not have applied the same force during the evaluation both before and after MAT. Nevertheless, the manual testing protocol used in this study has been previously validated in several investigations. 17,20,32 Second, the number of patients included is small but similar to previous cadaveric studies, and according to the sample size analysis, this study is adequately powered. Third, the kinematic tests were performed manually, and it was not possible to standardize the force applied. However, the senior surgeon (S.Z.) has more than 10 years of experience with surgical navigation and already demonstrated high reliability in manual assessments. 5,32 Last, because of ethical issues, a comparison with the intact knee could not be made, as we could not acquire data from the healthy contralateral limb. Future research should focus on new methods of collecting kinematic data in vivo and in a noninvasive manner.
Conclusion
The present study shows that lateral MAT was able to improve knee kinematic parameters at time zero after surgery; the biomechanical effect of MAT was particularly evident during the pivot-shift maneuver.
Footnotes
Acknowledgment
The authors thank Ms Silvia Bassini for her support with the graphics.
Final revision submitted December 12, 2020; accepted January 26, 2021.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Istituto Ortopedico Rizzoli (0008900).