
Abstract
Background:
Prospectively-collected patient-reported outcomes (PROs) following shoulder instability surgery are limited. Attention has been drawn to standardizing these outcome measures in the adolescent literature.
Hypothesis/Purpose:
The purpose of this study was to evaluate which factors predict unfavorable PROs following shoulder instability surgery, including a “No” response to the Patient Acceptable Symptom State (PASS) question. We hypothesized that poor outcomes are associated with adolescent males, bone loss, larger labral tears, and articular cartilage injury.
Methods:
A cohort of patients age 13 years and older undergoing shoulder instability surgery were prospectively enrolled in point-of-care data collection at a single institution across 12 surgeons from 2015-2017. Demographics, ASES and SANE responses, and surgical findings were obtained at baseline. ASES, SANE, and PASS responses as well as revision surgery were queried at least one year post-operatively. Patients with isolated posterior labral tears and prior ipsilateral shoulder surgery were excluded. Regression analyses were performed.
Results:
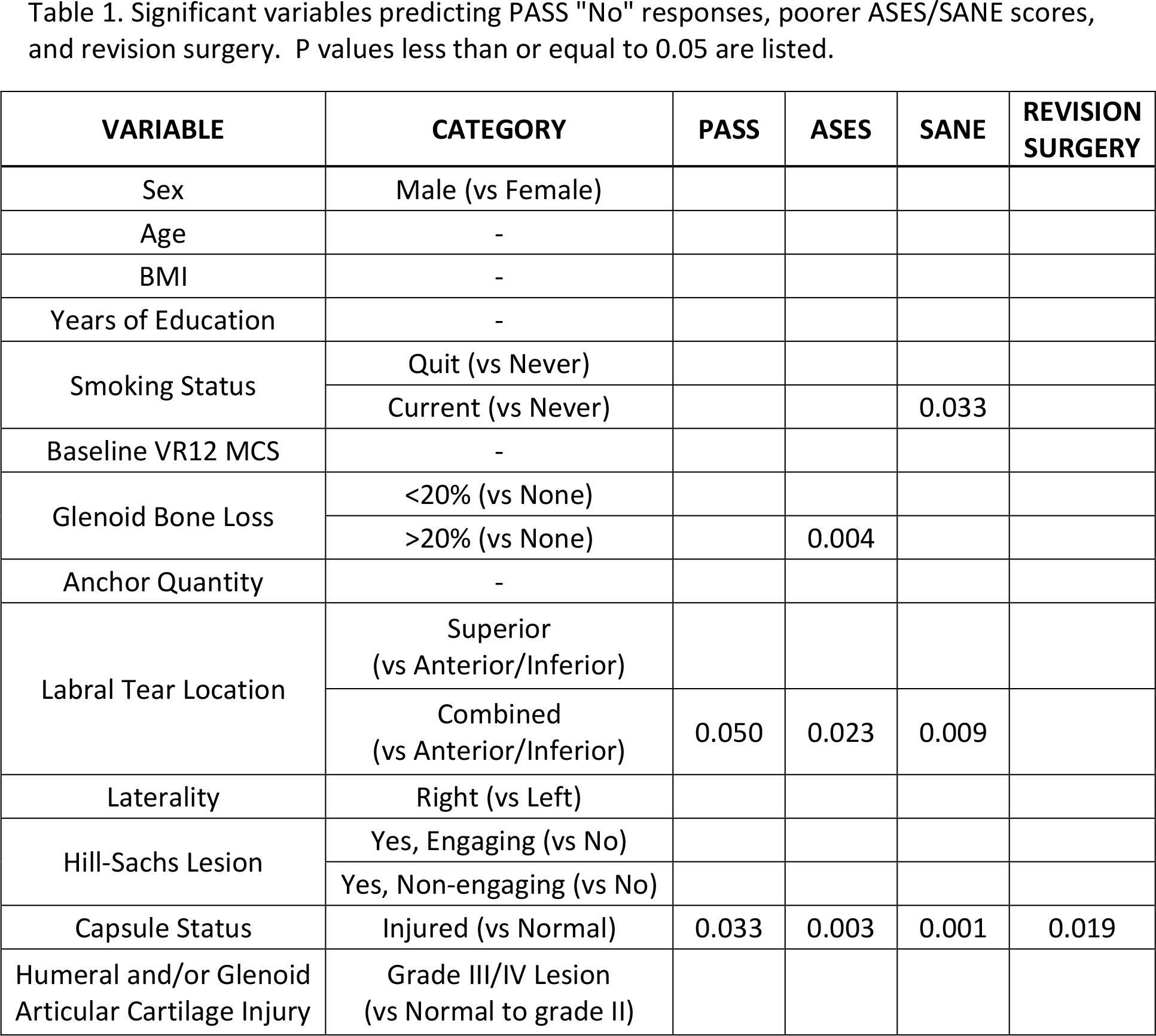
A total 268 patients met inclusion criteria of which 201 completed follow-up responses (75%). Non-responders had a greater BMI, smaller proportion of glenoid bone loss, fewer Hill-Sachs lesions, and lower baseline ASES scores by 7.5 points (p < 0.05). Responders’ mean age was 25.5 years and 23% were female. Revision surgery occurred in 2.5% of these patients, and 81% responded “Yes” to PASS. A “Yes” response correlated to mean 31-point improvement in ASES and 34-point improvement in SANE scores. On univariate analysis, “No” responders were more likely to have a smoking history, a larger proportion of glenoid bone loss, and revision surgery (p < 0.05). However, on multivariate analysis, only combined labral tears (anterior/inferior plus superior or posterior tears) and injured capsules were associated with greater odds of responding “No” to PASS and with lower ASES and SANE scores (p ≤ 0.05) (Table 1). Age, sex, Hill-Sachs lesions, and grade III/IV articular cartilage injuries were not associated with variation in any PROs.
Conclusion:
In this prospective cohort, patients largely approve of their symptom state at one year or greater following shoulder instability surgery. A PASS “Yes” response occurred in 81% of patients and correlated to a clinically and statistically significant improvement in ASES and SANE scores. Combined labral tears and injured capsules were negative prognosticators across PROs, whereas age, sex, and Hill-Sachs lesions were not.
Table:
Significant variables predicting PASS "No" responses, poorer ASES/SANE scores, and revision surgery. P values less than or equal to 0.05 are listed.
|
|
|
|
|
|
|
|---|---|---|---|---|---|
| Sex | Male (vs Female) | ||||
| Age | - | ||||
| BMI | - | ||||
| Years of Education | - | ||||
| Smoking Status | Quit (vs Never) | ||||
| Current (vs Never) | 0.033 | ||||
| Baseline VR12 MCS | - | ||||
| Glenoid Bone Loss | <20% (vs None) | ||||
| >20% (vs None) | 0.004 | ||||
| Anchor Quantity | - | ||||
| Labral Tear Location | Superior |
||||
| Combined |
0.050 | 0.023 | 0.009 | ||
| Laterality | Right (vs Left) | ||||
| Hill-Sachs Lesion | Yes, Engaging (vs No) | ||||
| Yes, Non-engaging (vs No) | |||||
| Capsule Status | Injured (vs Normal) | 0.033 | 0.003 | 0.001 | 0.019 |
| Humeral and/or Glenoid Articular Cartilage Injury | Grade III/IV Lesion |