
Abstract
Background:
Previous studies have reported a high prevalence of menstrual dysfunction (MD) among adolescent female athletes. Little is known about the characteristics of adolescent athletes with MD, as well as their awareness of MD.
Purpose:
Our primary study purpose was to determine the prevalence and characteristics of female athletes who believe that MD is a normal response to high training demands. The secondary purpose was to explore the relationship between MD and patient-reported quality of life.
Methods:
We conducted a cross-sectional study of adolescent athletes undergoing pre-participation evaluation. Participants completed health history, family affluence, and Patient-Reported Outcomes Measurement Information System (PROMIS) questionnaires. Those who reported menarche within the past year were excluded. We categorized participants into groups based on their response to, “Do you think it is normal to lose your period during high levels of athletic training?” (yes/no). We compared groups using Mann-Whitney U and Fisher’s exact tests. We also grouped patients into MD (yes/no) if they exhibited one or more of the following: 1) age of menarche >15 years; 2) ≤9 periods in the last year; or 3) a period of three consecutive months without a menstrual cycle. We constructed a series of linear multivariable regression models assessing the effect of MD on PROMIS outcomes adjusting for age and BMI.
Results:
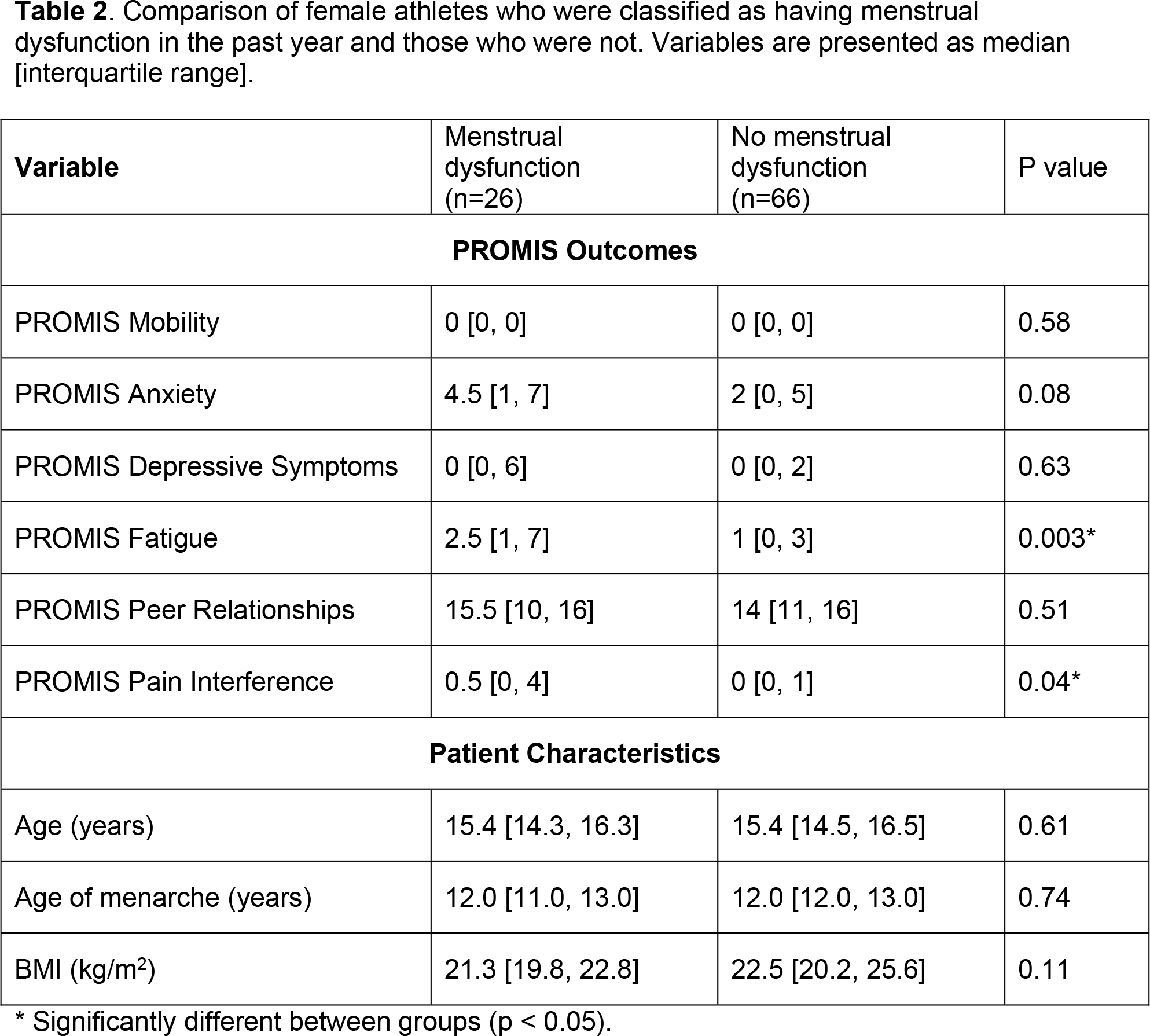
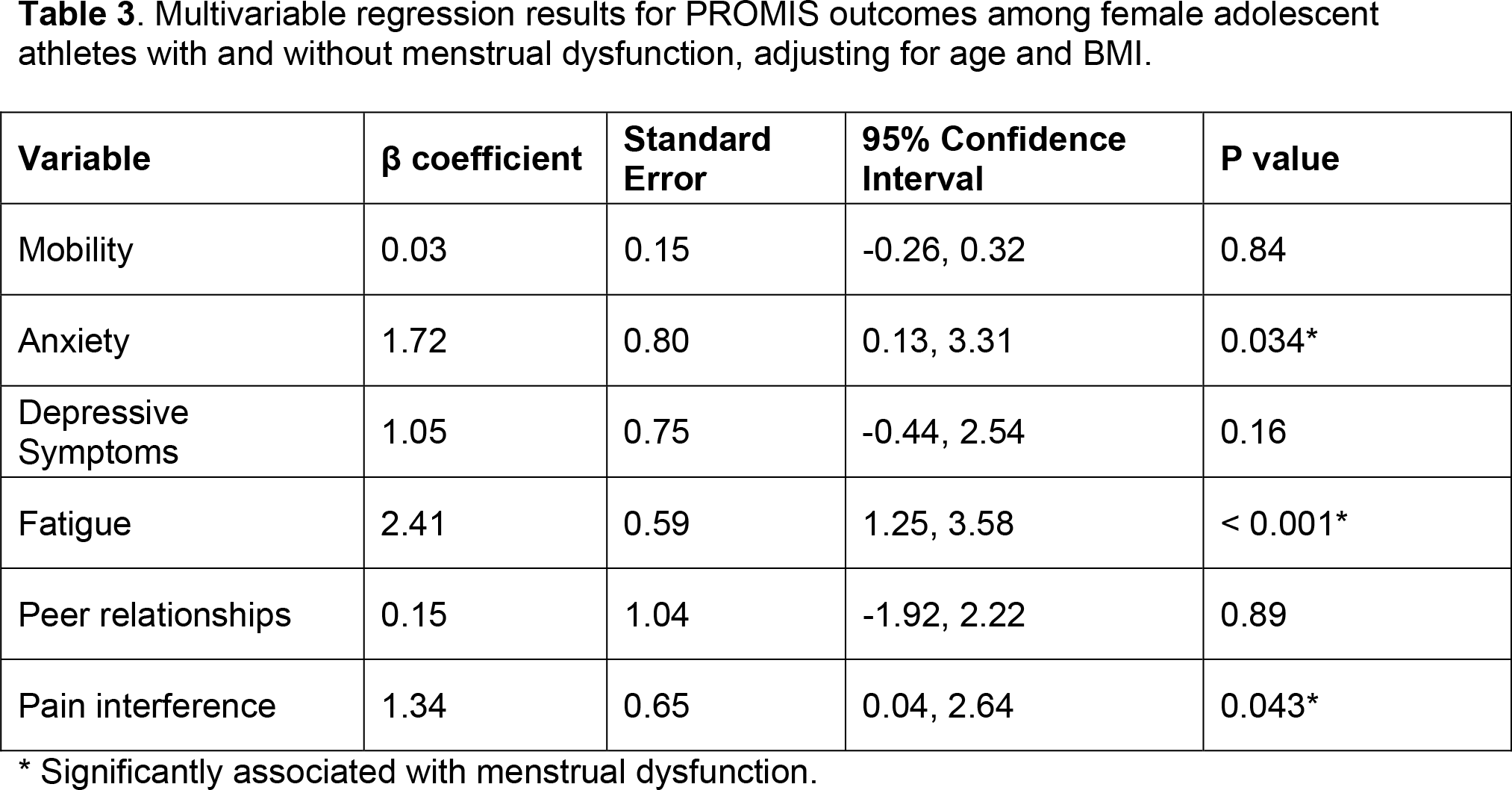
44% (n=40/90) answered that period loss was a normal response to a high level of training, and this group had lower body mass index (BMI), were less likely to report being worried about current weight, and had a higher family affluence level than those who answered period loss was not a normal response to training (Table 1). The overall prevalence of MD was 28% and was not significantly different between those who did and did not answer that period loss was a normal response to training (Table 1). Those with MD reported higher fatigue and pain interference scores than those without MD (Table 2). After adjusting for age and BMI, MD was significantly associated with higher levels of anxiety, fatigue, and pain interference (Table 3).
Conclusion:
Nearly half of our sample of adolescent female athletes perceive MD as a normal response to high training demands. Females with MD reported higher levels of anxiety and fatigue than those without MD. Understanding adolescent perceptions of MD and the characteristics of those with MD can guide future educational interventions aimed at high risk athletes for the female athlete triad.
Comparison of characteristics of female adolescent athletes based on answer to question regarding period loss in the setting of a high level of athletic training. Continuous variables are presented as median [interquartile range], categorical variables are presented as n (%).

| Variable | Answered loss of a period was a normal response to high level of training |
Answered loss of a period was NOT a normal response to high level of training |
P value |
|---|---|---|---|
| Current Age (years) | 15.5 [14.7, 16.5] | 15.2 [14.4, 16.3] | 0.30 |
| Age of menarche | 12.3 [12.0, 13.0] | 12.0 [11.0, 13.0] | 0.26 |
| BMI (kg/m2) | 21.2 [19.7, 23.3] | 22.8 [20.6, 25.6] | 0.04* |
| Menstrual dysfunction in the past year | 12 (30%) | 12 (24%) | 0.63 |
| Hours of training per week | 12 [10, 14] | 12 [10, 15] | 0.93 |
| History of stress fracture | 1 (3%) | 5 (10%) | 0.22 |
| Worried about weight | 1 (3%) | 8 (18%) | 0.04* |
| On a special diet | 5 (13%) | 4 (8%) | 0.73 |
| Family affluence scale score | 10 [9, 11] | 9 [8, 10] | 0.01* |
*Significantly different between groups (p < 0.05).
Comparison of female athletes who were classified as having menstrual dysfunction in the past year and those who were not. Variables are presented as median [interquartile range].
| Variable | Menstrual dysfunction |
No menstrual dysfunction |
P value |
|---|---|---|---|
| PROMIS Outcomes | |||
| PROMIS Mobility | 0 [0, 0] | 0 [0, 0] | 0.58 |
| PROMIS Anxiety | 4.5 [1, 7] | 2 [0, 5] | 0.08 |
| PROMIS Depressive Symptoms | 0 [0, 6] | 0 [0, 2] | 0.63 |
| PROMIS Fatigue | 2.5 [1, 7] | 1 [0, 3] | 0.003* |
| PROMIS Peer Relationships | 15.5 [10, 16] | 14 [11, 16] | 0.51 |
| PROMIS Pain Interference | 0.5 [0, 4] | 0 [0, 1] | 0.04* |
|
|
|||
| Age (years) | 15.4 [14.3, 16.3] | 15.4 [14.5, 16.5] | 0.61 |
| Age of menarche (years) | 12.0 [11.0, 13.0] | 12.0 [12.0, 13.0] | 0.74 |
| BMI (kg/m2) | 21.3 [19.8, 22.8] | 22.5 [20.2, 25.6] | 0.11 |
*Significantly different between groups (p < 0.05).
Multivariable regression results for PROMIS outcomes among female adolescent athletes with and without menstrual dysfunction, adjusting for age and BMI.
|
|
|
|
|
|
|---|---|---|---|---|
| Mobility | 0.03 | 0.15 | -0.26, 0.32 | 0.84 |
| Anxiety | 1.72 | 0.80 | 0.13, 3.31 | 0.034* |
| Depressive Symptoms | 1.05 | 0.75 | -0.44, 2.54 | 0.16 |
| Fatigue | 2.41 | 0.59 | 1.25, 3.58 | < 0.001* |
| Peer relationships | 0.15 | 1.04 | -1.92, 2.22 | 0.89 |
| Pain interference | 1.34 | 0.65 | 0.04, 2.64 | 0.043* |
*Significantly associated with menstrual dysfunction.