
Abstract
Background:
Year-round competitive sports places the youth athlete at risk for injury from chronic repetitive stress. Various conditions have been reported secondary to overuse. Stress injuries to the distal femoral physis in active adolescents are rare.
Hypothesis/Purpose:
The purpose if this report is to highlight 3 male youth soccer players who presented with a lateral distal femoral hemiphyseal arrest and subsequent unilateral genu valgum deformity in their dominant “kicking leg” due to repetitive microtrauma a phenomenon we refer to as youth kicker’s knee.
Methods:
A retrospective review of adolescents that presented to our orthopedic clinic for lateral distal femoral hemiphyseal arrest secondary to chronic repetitive kicking was performed from 2010 to 2018. History, physical exam and imaging findings were obtained as well as the treatment course for all adolescents.
Results:
All patients were 14 years of age, and all participated in year-round high intensity soccer and American football. Patient specific data is summarized in Table 1 and 2. Imaging studies demonstrated aberration of the distal lateral femoral physis in all. (Figure 1) To address their limb deformity all adolescents were surgically treated with guided growth which was successful in correcting the mechanical axis in 2 of the 3 adolescents Patient Numbers (PN) 1 and 3. (Figure 2) The adolescent (PN 2) that failed to correct was definitively treated with a lateral distal femoral opening osteotomy successfully realigning his limb.
Conclusion:
Our series illustrates a unique presentation of a chronic overuse / stress injury in hyper sporting adolescents resulting in an ipsilateral genu valgum deformity. Understanding adolescent growth and developmental characteristics is paramount to appropriate care, prevention, and treatment of physeal injuries that may occur from repetitive overuse and avoid surgery in these young athletes when possible.
Patient characteristics and presenting symptoms. M – male. PMH – past medical history. PSH – past surgical history. BMI – body mass index.

| Patient Number (PN) | Sex | Age (years) | Race | Laterality | PMH | PSH | BMI | Pain | Symptom duration | Sport | Follow |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 14 | Caucasian | Right | none | none | 23.0 | Yes | 8 weeks | Soccer Football |
36 |
| 2 | M | 14.5 | Caucasian | Right | none | none | 26.6 | Yes | 5 months | Soccer | 29 |
| 3 | M | 14 | Hispanic | Right | none | none | 19.0 | Yes | 24 months | Soccer | 21 |
Radiographic findings in three patients with atraumatic lateral femoral hemiphyseal arrest. RLE – right lower extremity. LLE – left lower extremity. MAD – mean axis deviation. mLDFA – mechanical lateral distal femoral angle.

| Patient |
RLE MAD | LLE MAD | RLE Q Angle | LLE Q Angle | Coxa Vara | RLE |
LLE |
Bone Age |
Lateral Physeal Appearance |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 2+ | 0 | 20 | 12 | no | 78 | 85 | 14.5 | Irregular/widened |
| 2 | 2+ | 0 | 24 | 14 | no | 81 | 88 | 15 | Irregular/widened |
| 3 | 2+ | 0 | 19 | 8 | no | 82 | 89 | 13.5 | Irregular/widened |

A-D. CT and MRI sequences in an adolescent boy with atraumatic lateral distal femoral physeal arrest. CT demonstrates widening and fragmentation of the lateral physis (A-B). T2-weighted MRI sequences demonstrate increased signal and widening in the lateral distal femoral physis (C). T1-weighted images demonstrate physeal widening (D).
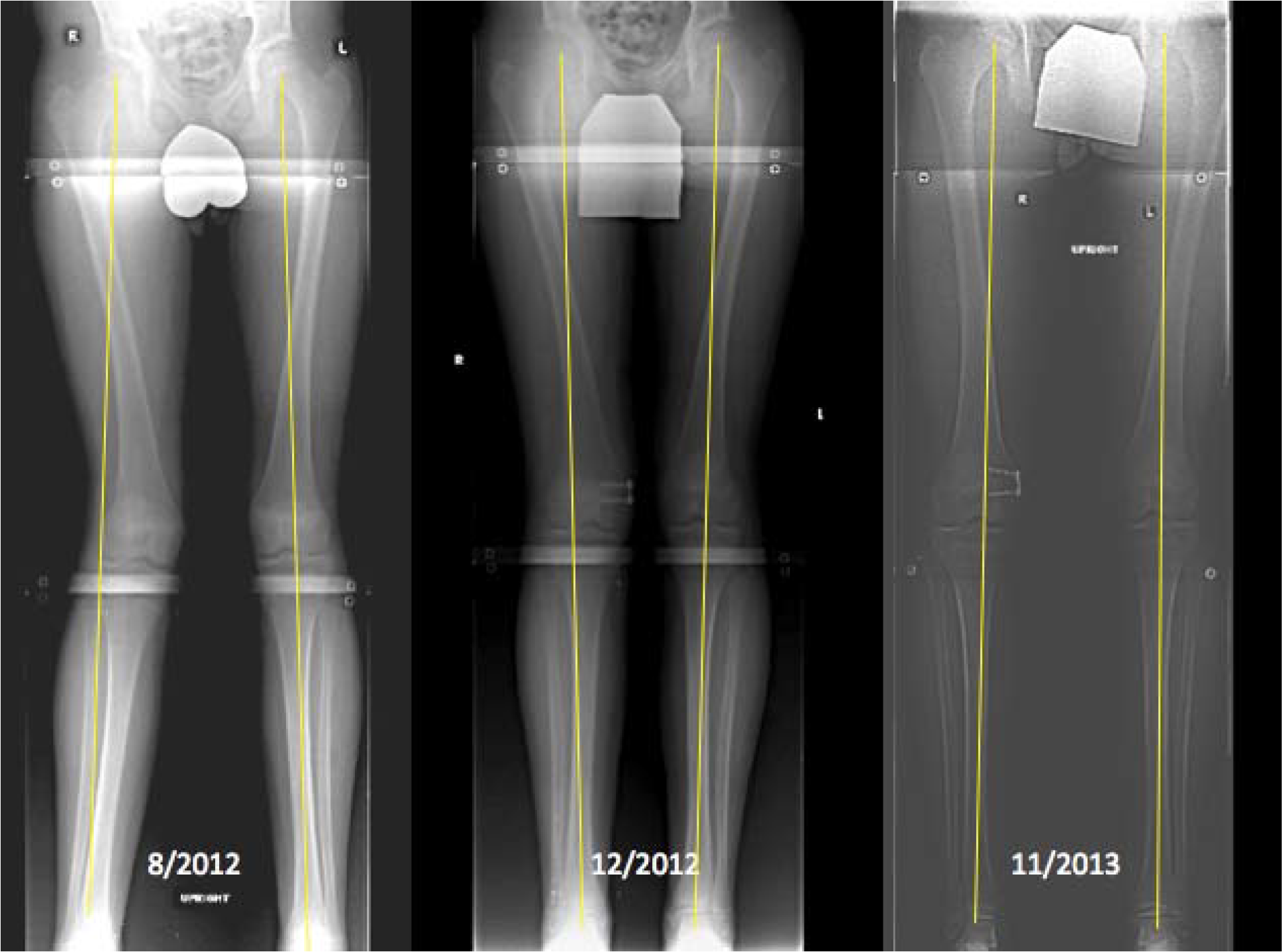
Serial standing alignment radiographs of an adolescent boy with lateral distal femoral hemiphyseal arrest treated with guided growth until resolution of his mechanical axis.