
Abstract
Background:
Scapular kinesia is an important component of glenohumeral rhythm and shoulder stability. No studies have evaluated scapular dyskinesis and its relationship to shoulder proprioception in patients who have undergone arthroscopic Bankart repair (ABR).
Purpose:
To investigate scapular dyskinesis, proprioception, and functional level after ABR.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This study included 13 male patients who underwent ABR (ABR group; mean age, 30 years; range, 24-36 years) and 13 sex- and age-matched healthy individuals (control group). The age, height, weight, and dominant side of all participants were collected. Scapular dyskinesis was evaluated using the lateral scapular slide test and the scapular dyskinesis test; proprioception was measured by the active angle reproduction test using a smartphone goniometer application, and functional level was assessed using the upper-quarter Y-balance test for dynamic stability as well as the Rowe score and Walch-Duplay score for quality of life and return to activities of daily living.
Results:
The presence of static scapular dyskinesis in the neutral position, at 45° of abduction, and at 90° of abduction as well as the presence of dynamic scapular dyskinesis was higher in the ABR group compared with the control group (P ≤ .04 for all). Shoulder joint position sense (absolute error) at 40° and 100° of shoulder elevation and shoulder functional level according to the Rowe score were worse in the ABR patients compared with the healthy controls (P ≤ .02 for all). Dynamic scapular dyskinesis was negatively related to shoulder joint position sense at 40° of shoulder elevation (r = –0.64; P = .01). Static scapular movement as measured on the lateral scapular slide test was moderately related to the Rowe score (r = 0.58; P = .03).
Conclusion:
Scapular kinematics and proprioception should be evaluated after ABR. Treatment approaches to improve scapular control and proprioceptive sense should be included in the rehabilitation program for patients after ABR.
Impairment of scapulohumeral rhythm has been observed after shoulder injuries or surgeries. 18 Shoulder instability can be determined by pathological kinematic pattern, impaired movement, and dysfunction of the scapula. Additionally, abnormal position of the scapula, downward rotation of the glenoid, and decentralization of the humeral head from the glenoid cause shoulder instability. 12 Loss of proprioceptive sense has been found after shoulder injury, pathology, and/or surgery. 16 Shoulder instabilities may entail loss of proprioceptive sense by mechanoreceptors in the stabilizer muscles of the shoulder that cannot provide adequate control for the shoulder joint. 1,14,30
Scapular dyskinesis has been reported in 25% of patients who have undergone a Latarjet procedure 4 and 100% of patients with anterior shoulder instability. 24 To the best of our knowledge, no study has evaluated scapular dyskinesis after arthroscopic Bankart repair (ABR). When searching the literature, we found a case report that investigated the effect of ABR on shoulder proprioception, which might be considered a related study. 8 Those authors found improved active shoulder proprioception at abduction and external rotation. Another study evaluated shoulder proprioception after different shoulder instability surgeries (10 patients with open Bankart repair and 4 patients with ABR). 20 In that work, proprioception was found to be improved after surgical repair for shoulder instability, but the authors did not make comparisons between the 2 surgical techniques. 20
To the best of our knowledge, no study in the literature has evaluated scapular dyskinesis after ABR. 13 The aim of the present study was to investigate scapular dyskinesis, shoulder joint position sense, and shoulder functional level after ABR. The hypothesis was that there is a relationship between scapular dyskinesis, proprioception, and functional level in patients who undergo ABR.
Methods
Study Design and Participants
This was a case-control study; each patient’s unaffected limb acted as his own internal control, and the dominant side was assessed for the healthy control participants. Ethical approval for the study was received from Uskudar University, and written consent was obtained from all participants. A total of 24 male patients who had undergone ABR between 2018 and 2019 were eligible for enrollment; of these, 5 patients refused to participate. A further 4 patients were excluded because of their smoking addiction, and 2 patients discontinued follow-up because of other health problems. To sum, 13 patients who underwent ABR were included in the study. After the patients were assessed, healthy individuals with the same age and physical characteristics (weight and height) were invited, and 13 sex- and age-matched healthy controls were included in the study. The flowchart of the study is shown in Figure 1.

Flowchart of the study.
Inclusion criteria for the ABR patients were as follows: (1) age between 18 and 40 years; (2) at least 6 months after surgery; (3) a single first-time anterior shoulder dislocation; (4) Bankart repair accomplished with 1 double-loaded suture anchor; and (5) full and pain-free range of shoulder motion at 6 months after ABR. Exclusion criteria for the ABR patients were (1) history of 2 or more shoulder dislocations; (2) any previous upper extremity surgery; (3) history or clinical evidence of neurologic signs or disease or cognitive, mental, or psychological problems; (4) any systemic disease that may cause deep sensory loss (eg, diabetes, metabolic syndrome, chronic renal failure); (5) body mass index (BMI) >30 kg/m2; and (6) history of smoking. For the healthy control participants, inclusion criteria were (1) age between 18 and 40 years; (2) no injury, surgery, or pathology of the shoulder joint; (3) no history or clinical evidence of neurologic signs or disease or cognitive, mental, or psychological problems; (4) no systemic disease that may cause deep sensory loss (eg, diabetes, metabolic syndrome, chronic renal failure); (5) BMI <30 kg/m2; and (6) no history of smoking.
Operative Procedure
All operations were performed by the same surgeon (A.M.O.) with the patient in the beach-chair position; no arm holders were used. First, a standard posterior portal (2 cm inferior and 1 cm medial to the posterolateral corner of acromion) was placed for viewing. Second, an anteroinferior portal was placed under direct vision from the posterior portal with aid of a spinal needle. This portal, which was slightly inferolateral to the coracoid and just above the superior edge of the subscapularis tendon, was used for anchor placement. Third, an anterior portal was placed lateral and superior to the coracoid process and just anterior to the biceps tendon under direct vision from the posterior portal with aid of a spinal needle; this portal was used for suture management. A single all-suture anchor with double-loaded sutures 2.9 mm in diameter (Doratek Medical) was used in all cases. The suture anchor was placed on the glenoid surface at the 5-o’clock position for the right shoulder and at the 7-o’clock position for the left shoulder. Postoperatively, an arm sling was used for 4 weeks for all patients, but passive elevation and abduction exercises and active elbow range of motion were started on the first postoperative day. All patients underwent a standard rehabilitation program after ABR. 8,20
Measures
The age, height, weight, and dominant side of all participants were collected. Before the assessment, all participants jogged for about 5 minutes to induce whole-body warming. Then, using a resistive elastic band, participants performed upper extremity warming for about 5 minutes at flexion, extension, abduction, adduction, and external and internal rotation. A rest of 120 seconds was given between the whole-body and upper extremity warming.
Assessment of Scapular Dyskinesis
The presence of scapular dyskinesis was evaluated using static and dynamic scapular movement tests. All scapular dyskinesis assessments were performed by the first author (C.S.). Static scapular movement was assessed with the lateral scapular slide test (LSST). The test was performed when the participant was in a standing position. Measurements were collected from 3 different positions of the shoulder (in neutral, at 45° of abduction, and at 90° of abduction). Distances were measured in 2 ways: (1) the spinous process of T3 vertebra to the medial corner of the scapula and (2) the spinous process of T7 vertebra to the inferior corner of the scapula. Measurements were made with a tape measure, and the difference between the 2 sides was calculated (Figure 2). Scapular dyskinesis was accepted as positive if the difference between the 2 sides was >1.5 cm. 29

Assessment of static scapular dyskinesis using the lateral scapular slide test for (1) the spinous process of T3 vertebra to the medial corner of the scapula and (2) the spinous process of T7 vertebra to the inferior corner of the scapula.
Dynamic scapular movement was assessed with the scapular dyskinesis test (SDT). Data from 5 repetitions of bilateral active shoulder flexion and 5 repetitions of bilateral shoulder abduction were collected. 15,26 The arm of the patient was simultaneously elevated as far as possible to a 3-second count using the “thumbs-up” position and then lowered to a 3-second count (Figure 3). All tests were done with 1.4- or 2.3-kg dumbbells. After the SDT was completed, the type of dynamic scapular dyskinesis was determined: type 1, inferior angle prominence; type 2, medial border prominence; type 3, excessive superior border elevation; or type 4, symmetric (normal) scapular motion. 15,26

Assessment of dynamic scapular dyskinesis using the scapular dyskinesis test.
Assessment of Shoulder Joint Position Sense
Shoulder joint position sense was evaluated by using an active position repetition test, also known as the active angle repetition test. The active position repetition test is a valid and reliable method in the shoulder joint. 1 The active angle repetition test for the shoulder joint position was evaluated using a smartphone application software program (Goniometer Pro; G-Pro, 5FUF5 CO). The goniometer application is adapted to both iOS (Apple) and Android systems (Open Handset Alliance), and it is valid and reliable for determining joint position sense of shoulder. 10 Shoulder proprioception was defined as the ability to match reference shoulder joint angles (the “target angle”) without visual feedback. For each repetition, the patients moved the arm to the target angles (40° and 100°) for shoulder elevation at the scapular plane (45° anterior to the frontal plane) actively. 10,30 When patients felt they had reached the target angle, they stopped their arm and were not permitted to correct the angle. The angle was recorded from the on-screen goniometer; this process was repeated 6 times for each target angle. A total of 6 readings were taken; the difference between the perceived angle and each of the target angles (40° for shoulder elevation at the scapular plane and 100° for shoulder elevation at the scapular plane) was noted as the absolute error, and an average absolute error was calculated for each trial. Deviations of mean 6.6° or less were considered to indicate normal proprioceptive sense. Deviations above this cut-off value were accepted as pathological proprioceptive sense. 30 All shoulder joint position assessment was performed by the second author (M.U.).
Assessment of Shoulder Functional Level
The functional level of the shoulder was determined using the upper-quarter Y-balance (YBT-UQ) test, the Walch-Duplay score, 27 and the Rowe score. 22 All functional assessments were performed by the third author (M.C.). The YBT-UQ test was used to evaluate the dynamic stability of the upper extremity; this test was performed as described by Gorman et al. 6 Three tape measures were attached to the floor in the medial, inferolateral, and superolateral reach directions. Of these, 2 posterior tape measures were positioned 135° from 1 anterior tape measure, with an angle of 90° between the posterior tape measures. The patient was asked to reach as far as possible in all 3 directions, and the distances for all trials in each direction were collected. The maximum reach distance was divided by the patient’s upper extremity length to normalize each reach distance. To measure upper extremity length, the patient raised (abduction) the right arm to shoulder height (90°). The distance from the C7 spinous process to the tip of the right middle finger (in centimeters) was measured. Each participant performed 3 repetitions, and the greatest value was recorded.
The Rowe score and Walch-Duplay score were used to determine quality of life and return to activities of daily living. Results were interpreted according to the total score for both scales: 90-100 = very good, 75-89 = good, 51-74 = medium, and ≤50 = bad.
Statistical Analysis
All data were analyzed with the Statistical Package for the Social Sciences (SPSS Version 22; IBM Corp). Characteristics of patients were described using means and standard deviations. The normality of the distribution of the data was investigated by Kolmogorov-Smirnov testing with α set at .05. This test confirmed that the data were normally distributed and that further statistical analyses using the parametric testing would be appropriate. The chi-square test was used to compare extremes for data of the SDT and the Walch-Duplay score. The Mann-Whitney U test was used to compare sides regarding the LSST, joint position sense, the YBT-UQ, and the Rowe score. Spearman correlation was used to investigate the relationship between scapular dyskinesis, proprioception, and functional level. Statistical significance was set at α < .05. The sample size of 13 participants for each group was calculated on joint position sense data with power 80% and alpha level 1% from Pötzl et al. 20
Results
For the 13 patients who underwent ABR, the average age was 30 years (range, 24-36 years; BMI, 25.04 ± 2.82 kg/m2), and for the 13 sex- and age-matched control participants, the average age was 30 years (range, 24-36 years; BMI, 23.63 ± 3.59 kg/m2) The average time from surgery to evaluation in the ABR patients was 16 months (range, 8-36 months).
Comparisons Between the ABR Patients and Healthy Controls
When comparing the operated side of the ABR patients with the dominant side of the control participants, we found significant differences in the distance between the spinous process of T7 vertebra to the inferior corner of scapula at neutral position (P = .04), 45° of abduction (P = .03), and 90° of abduction (P = .04), indicating that the presence of static scapular dyskinesis was higher in the ABR group (Table 1). The presence of dynamic scapular dyskinesis was also higher in the ABR group versus the controls (P = .03) (Table 2).
Differences in Lateral Scapular Slide Test Results Between the ABR Patients and Controls a
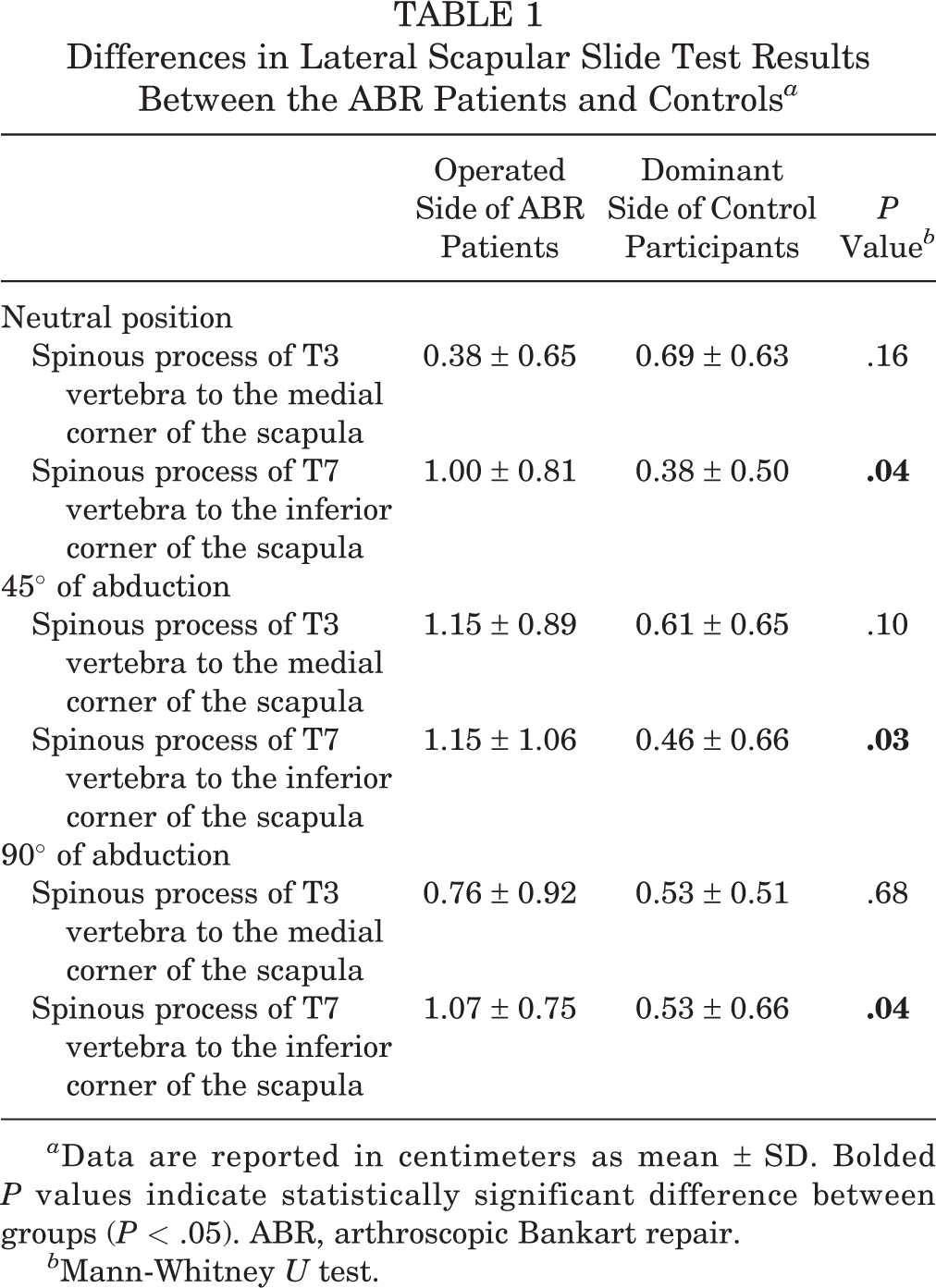
a Data are reported in centimeters as mean ± SD. Bolded P values indicate statistically significant difference between groups (P < .05). ABR, arthroscopic Bankart repair.
b Mann-Whitney U test.
Differences in the Type of Dynamic Scapular Dyskinesis Between the ABR Patients and Controls a

a Data are reported as n (%). Bolded P value indicates a statistically significant difference between groups (P < .05). ABR, arthroscopic Bankart repair.
b Chi-square test.
Shoulder joint position sense (absolute error) was significantly worse in the ABR group versus the control participants, at both 40° and 100° shoulder elevation (P = .01 for both) (Table 3). A standard deviation of ≤6.6° was accepted as ordinary proprioceptive sense.
Differences in Joint Position Sense (Absolute Error) at 40° and 100° of Shoulder Elevation Between the ABR Patients and Controls a

a Data are reported as mean ± SD. Bolded P values indicate a statistically significant difference between groups (P < .05). ABR, arthroscopic Bankart repair.
b Mann-Whitney U test.
No difference in the YBT-UQ test was found between the ABR patients and the control participants (Table 4). The ABR patients had a significantly worse Rowe score versus the controls (P = .02), although there was no difference in the Walch-Duplay score between the groups (Table 5).
Differences in the Upper-Quarter Y-Balance Test Scores Between the ABR Patients and Controls a
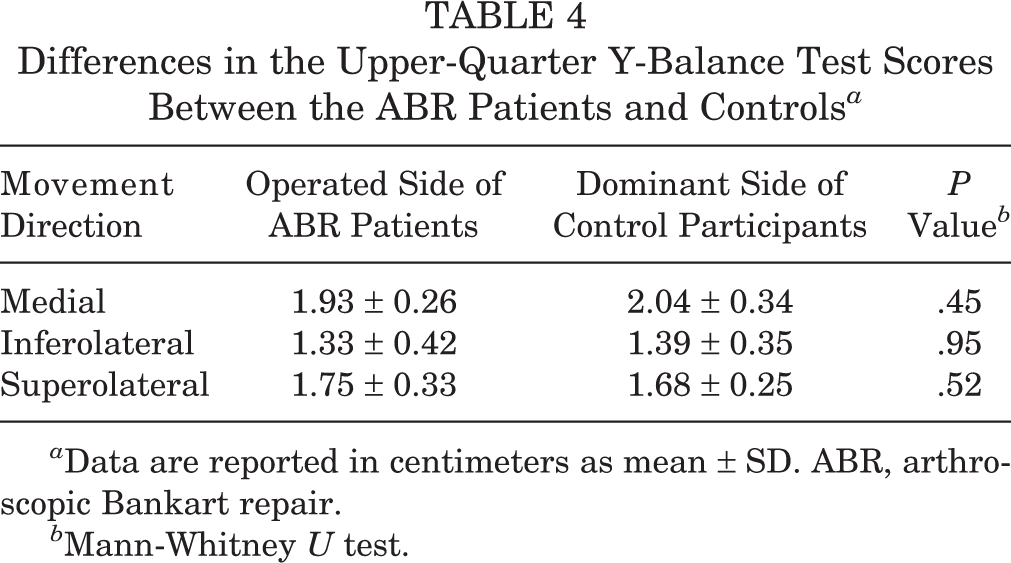
a Data are reported in centimeters as mean ± SD. ABR, arthroscopic Bankart repair.
b Mann-Whitney U test.
Differences in the Rowe Score and Walch-Duplay Score Between the ABR Patients and Controls a
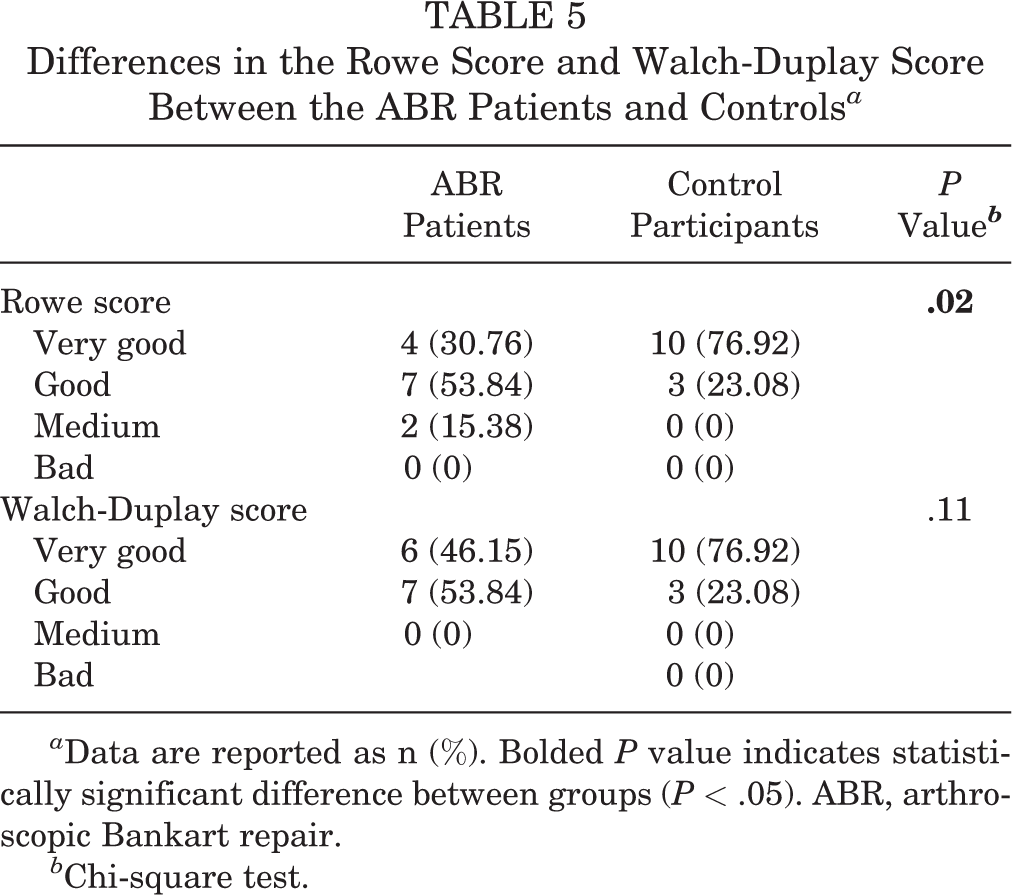
a Data are reported as n (%). Bolded P value indicates statistically significant difference between groups (P < .05). ABR, arthroscopic Bankart repair.
b Chi-square test.
Relationship Between Scapular Dyskinesis, Proprioception, and Functional Level
No significant relationship was found between static scapular dyskinesis (as measured by the LSST) and joint position sense (absolute error) at 40° and 100° of shoulder elevation. A strong negative correlation was found between dynamic scapular dyskinesis (as measured by the SDT) and joint position sense (absolute error) at 40° of shoulder elevation (r = –0.64; P = .01). There was no significant relationship between static scapular dyskinesis and the YBT-UQ test, nor was there a relationship between dynamic scapular dyskinesis and the YBT-UQ test. We noted a moderate relationship between static scapular dyskinesis (neutral/inferior) and the Rowe score (r = 0.58; P = .03). There was no significant relationship between dynamic scapular dyskinesis and either the Rowe score or the Walch-Duplay score.
Power Analysis of the Study
A post hoc power calculation was conducted using G* Power 3.1.9.2, with joint position sense at 100° of shoulder elevation, an alpha level of .01, and a sample size of 13. The statistical power was 95.11%.
Discussion
This was the first study to investigate scapular dyskinesis after ABR. Scapular dyskinesis and joint position sense deficit in patients who underwent ABR were found to be comparable to values for the dominant side of healthy control participants. Patients had similar functional levels as healthy controls according to YBT-UQ and Walch-Duplay scores, whereas patients had lower Rowe scores compared with healthy controls. Dynamic scapular movement was negatively related to shoulder joint position sense at 40° and 100° of shoulder elevation. Static scapular movement was also related to the Rowe score, which affects the quality of daily living.
The normal kinematic parameters of the scapula have an important role in providing harmonious, fluent, and coordinated movement pattern in the upper extremity. The task of the scapula is to contribute to shoulder movements, control of movement, and shoulder stabilization during arm elevation. 7 Scapular dyskinesis may be due to injury or surgery as well as glenohumeral and subacromial pathologies. 21
Numerous studies have evaluated the presence of scapular dyskinesis in shoulder problems. 7,18,23 In these studies, scapular dyskinesis was evaluated with regard to rotator cuff tears and impingement syndrome. Few studies have evaluated the role of scapular dyskinesis in shoulder instability, 17,28 and we found no study that evaluated the presence of scapular dyskinesis after ABR.
In the present study, we evaluated static scapular dyskinesis using the LSST in patients who had undergone ABR. The LSST should evaluate both the position of the scapula and the stabilization ability of the posterior muscles of the shoulder. 11 We found differences between the operated side of the patients and the dominant side of the control participants in terms of the distance between the spinous process of T7 vertebra to the inferior corner of the scapula at neutral, 45° of abduction, and 90° of abduction. We noted no relationship between static scapular dyskinesis, shoulder proprioception, and functional level. In the present study, the active angle reproduction test was used to evaluate shoulder proprioception. During this test, mechanoreceptors from the muscles and ligaments around the shoulder and scapula actively send signals to the central nervous system. The difference between the operated side of the patients and the dominant side of the healthy controls in the static test may not have been reflected during the dynamic activities. This situation is supported by the fact that the dynamic SDT is highly related to the proprioception test. If passive proprioception tests had been used, shoulder joint position sense might be related to the static scapular dyskinesis test. Studies are needed to determine the relationship between static scapular dyskinesis and passive shoulder joint position tests in patients with ABR.
We evaluated dynamic scapular dyskinesis using the SDT and determined types of scapular dyskinesis. Scapular dyskinesis was found in 10 of the 13 ABR patients and 3 of the control participants. Scapular dyskinesis may be an important finding in both healthy individuals and patients. The presence and type of scapular dyskinesis are thought to be important guides in determining whether scapular dyskinesis will lead to instability. Muscles that provide dynamic stabilization of the shoulder should determine the position of the scapula. Loss of control in these muscles should cause malposition and dysfunction of the scapula and proprioception deficit. 13,25
Proprioception of the glenohumeral joint contributes to shoulder stabilization and coordination of capsuloligamentous complex and muscle activation. 5 Loss of proprioception with impaired neuromuscular control leads to instability of the joint. After dislocation or subluxation, shoulder stabilizers are not sufficient to control glenohumeral joint movement, and impaired neuromuscular control due to decreased proprioceptive sense may lead to the recurrence of shoulder instability. 30 In the present study, we found differences in joint position sense (absolute error) at 40° and 100° of shoulder elevation between the operated side of the patients and the dominant side of the controls, while there was a strong negative correlation between dynamic SDT and joint position sense (absolute error) at 40° of shoulder elevation at the operated side of patients.
Elevation of the shoulder complex up to 30° is performed by the glenohumeral joint, 11 and the scapula comes into play at this angle. 31 At 40° of shoulder elevation, the activity of the upper trapezius muscle increases. 19 The relationship between dynamic scapular dyskinesis and proprioception deficit at 40° of shoulder elevation may be due to increased activity of the upper trapezius. The increased distance between the spinous process of T7 vertebra to the inferior corner of the scapula at neutral position, 45° of abduction, and 90° of abduction on a patient’s operated side may support increased upper trapezius activity. Increasing these distances indicates that the scapula moves more upward and laterally. Additionally, increased upper trapezius activity excessively elevates the scapula through clavicular elevation. 9 Altered scapular movement or position may be related to shoulder proprioception deficit. 19 To clarify this issue, studies are needed that collect electromyographic activity of the upper trapezius and scapular dyskinesis evaluation using 3-dimensional motion analysis during proprioception testing.
In recent years, 2 studies have examined proprioception after Bankart repair. 2,8 Hung 8 evaluated proprioception in shoulder abduction and rotation in a patient who underwent open Bankart repair surgery. The rehabilitation program was performed and proprioception was reevaluated after 6 months. The author found improved proprioception in the patient after the rehabilitation program. Data analysis in that study showed that proprioception at 90° and 135° was normal, whereas a proprioception deficit at 45° of abduction remained after 6 months surgery. The author explained why proprioception at 90° and 135° was normal, as follows: “After surgery, anterior glenohumeral joint structures would be tightened to provide better passive restraints. Moreover, tightened passive shoulder stabilizers can heighten shoulder joint position sense with more sensitive joint or capsule receptors.” 8 Tightened passive shoulder stabilizers may be due to excessive activity of the upper trapezius, as we mentioned above.
Aydin et al 2 evaluated 20° internal rotations and 20° external rotations at 90° of shoulder abduction for joint position sense of the shoulder. The authors concluded that ABR normalizes proprioceptive sensitivity. The 20° shoulder rotations are the early phase exercises for ABR. Use of 45° shoulder rotations for proprioception tests in their study would have led to a different result in terms of proprioception. The results cannot be compared with our results because the authors did not evaluate proprioception in the abduction movement.
It could be concluded from the present study and studies in the literature that the proprioception level of patients with shoulder instability is worse than that of healthy individuals, regardless of whether they undergo surgery. Studies are needed to investigate the effects of exercise programs to improve proprioception after ABR. Considering that loss of proprioception has been reported in the third year after anterior cruciate ligament reconstruction, 3 the results of follow-up at 16 months after surgery, as in the present study, may not be sufficient to understand whether Bankart repair has a positive effect on proprioception. Long-term follow-up studies are needed.
We found no differences in YBT-UQ test results or Walch-Duplay scores between patients with ABR and the control group. These findings suggest that shoulder function had reached normal levels after ABR. The absence of pain and kinesiophobia and the presence of full range of motion may have positively affected the patients’ functional level. When questioned during the test about pain intensity, none of our patients reported pain. Additionally, all patients had full range of motion, as this was an inclusion criterion. Kinesiophobia was not evaluated in this study. We believed that these parameters should be assessed in patients with functional impairment after ABR.
Limitations
There were some limitations of our study. Only postoperative evaluation was performed. Therefore, we had no information about the presence of scapular dyskinesis and proprioceptive sense before surgery or injury. Use of 3-dimensional movement analysis to evaluate scapular dyskinesis and isokinetic testing to evaluate joint position sense would have provided more precise and objective results. We did not evaluate patients who underwent shoulder instability surgery other than ABR, and the sample size was small. Furthermore, the duration of follow-up differed among our patients. We evaluated 1 patient at 8 months after surgery, at which time the patient had successfully completed the rehabilitation process. The results of the patient were very good, and we retained the patient in the study. All other patients were evaluated at least 1 year after their surgery.
Conclusion
In the current study, scapular dyskinesis and proprioceptive deficits were found in patients who had undergone ABR. The functional level of patients after ABR was found to be similar to that of healthy individuals. We believe that patients who are considered to have scapular dyskinesis and loss of proprioception before surgery and/or injury should undergo postoperative rehabilitation to correct scapular dyskinesis and improve proprioception. Additionally, we noted a strong negative relationship between dynamic scapular dyskinesis and joint position sense at 40° of shoulder elevation on the operated side of patients. Exercises that improve both dynamic scapular control and proprioception <90° shoulder elevation should be considered for these patients.
Footnotes
Final revision submitted July 22, 2020; accepted September 4, 2020.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Uskudar University (ref No. B.08.6.YÖK.2.ÜS.0.05.06/2018/920).
Acknowledgment
The authors are grateful to all of the participants in this study.