
Abstract
Background:
Arthroscopic treatment of femoroacetabular impingement syndrome (FAIS) has become a common procedure. However, meaningful long-term clinical outcomes have not been defined.
Purpose:
To define the minimal clinically important difference (MCID), substantial clinical benefit (SCB), and patient acceptable symptomatic state (PASS) for the modified Harris Hip Score (mHHS) at a minimum 10-year follow-up in patients undergoing arthroscopic treatment for FAIS and identify preoperative predictors for achievement of the MCID, SCB, and PASS.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
A consecutive series of patients undergoing arthroscopic treatment for FAIS between 2007 and 2009 with a minimum 10-year follow-up was analyzed. Patient data included patient characteristics, radiographic parameters, and the pre- and postoperative mHHS and visual analog scale (VAS) for pain score. Paired t tests were used to compare the patient-reported outcome measures (PROMs). The MCID was determined by calculating half of the standard deviation, and SCB and PASS were calculated by the anchor method. Correlation and logistic regression analyses were conducted to identify predictors for the achievement of the MCID, SCB, and PASS.
Results:
A total of 44 patients (27 men, 17 women) were included. The mean age and body mass index were 42.2 years (range, 16-67 years) and 22.3 kg/m2 (range, 16.76-29.78 kg/m2), respectively. The MCID, absolute SCB, net change SCB, and PASS of the mHHS were calculated to be 19.6, 90.1, 31.5, and 84.4 points, respectively. Preoperative symptom duration was identified as an independent predictor for the achievement of meaningful clinical outcomes. The median symptom durations for patients who achieved the MCID, absolute SCB, net change SCB, and PASS were 11.7, 9.1, 9.0, and 10.8 months, respectively. The median symptom duration for patients who did not achieve the MCID, absolute SCB, net change SCB, and PASS were 15.8, 17.4, 17.3, and 18.4 months, respectively. No other statistically significant correlations were found.
Conclusion:
The preoperative duration of symptoms was identified as an independent predictor for achievement of the MCID, SCB, and PASS. These findings can be helpful in accelerating the transition to surgical treatment of FAIS.
Femoroacetabular impingement syndrome (FAIS) is increasingly recognized as an important cause of hip pain. 2,14,17,23,43 Arthroscopic treatment of FAIS has been demonstrated to provide a high level of clinical success, and this has resulted in a significant increase in the number of arthroscopic hip surgeries. 4,26,27,37 –39,41
In recent years, orthopaedic research has evolved from merely demonstrating statistical improvements in patient-reported outcome measures (PROMs) to defining differences resulting in clinically significantly improved outcomes. 7,10,19,28,36,49 The minimal clinically important difference (MCID) is defined as the lowest outcome difference that the patient perceives as clinically important. 21,25 In addition to the MCID, substantial clinical benefit (SCB) is increasingly reported. SCB is defined as the clinical value that the patient thinks to be considerable. 16,46 Thus, the MCID is the lower bound and tracks the minimum improvement goal, whereas SCB gauges the upper bound, the best possible outcome. 12 The patient acceptable symptomatic state (PASS) score has been defined as the postoperative threshold, above which a patient is deemed to have had a satisfactory outcome. 25 Previous clinical investigators have defined the MCID, SCB, and PASS at different time points after the arthroscopic treatment of FAIS. 7,10,13,34,35,36 However, the MCID, SCB, and PASS for the mHHS have been defined for only short- and midterm follow-ups.
Data on meaningful, long-term improvements after arthroscopic treatment of FAIS are lacking. Therefore, the aim of this study was to define the MCID, SCB, and PASS for the mHHS in patients undergoing arthroscopic treatment of FAIS at the 10-year follow-up and determine correlations between preoperative patient characteristics and the MCID, SCB, and PASS at the long-term follow-up.
Methods
Patient Selection
After institutional review board approval, a prospective review of patients undergoing hip arthroscopy between 2007 and 2009 was conducted. Consecutive patients who underwent arthroscopic treatment for FAIS by a single surgeon (W.M.) were identified. Patient characteristics, pre- and postoperative clinical data, and PROMs were prospectively collected in our institutional registry. Inclusion criteria were clinical and radiographic diagnosis of symptomatic FAIS, 17 failure of conservative treatment, and a minimum 10-year follow-up. Exclusion criteria included conversion to total hip arthroplasty (THA), hip dysplasia (lateral center-edge angle [LCEA] of Wiberg, 48 <25°), osteoarthrosis Tönnis grade >1, history of pediatric hip disorders (slipped capital femoral epiphysis [SCFE], developmental hip dysplasia, etc), and follow-up of less than 10 years. Although hips with Tönnis grade >1 made up half of the original cohort, it is now known that these hips will experience less improvement, and nowadays, these hips are not likely to undergo joint-preserving surgery. Therefore, these hips were excluded.
Radiographic Analysis
Pre- and postoperative radiographs consisted of a standardized standing anteroposterior pelvic overview radiograph and a 45° Dunn view lateral hip radiograph. The alpha angle, 33 Tönnis angle, 45 Tönnis osteoarthrosis grade, and LCEA were measured individually by 2 authors (A.Z. and C.S.). The data were analyzed by calculating intraclass correlation coefficients (ICCs), a measure of the proportion of variance that is attributable to individuals. 30 An ICC of 1 indicates perfect agreement. We found very good agreement between the 2 observers (ICC, 0.98).
Surgical Technique
All hip arthroscopies were performed by a single fellowship-trained hip surgeon (W.M.) at a high-volume hospital. All hip arthroscopies were performed with the patient in the supine decubitus position and under general anesthesia. The patients were positioned on a traction table with a well-padded perineal post, and the ipsilateral hip was distracted. In total, 2 standard arthroscopy portals were used during the surgery: the anterolateral and midanterior portal. A periportal capsulotomy but no interportal capsulotomy was performed. Labral repair or routine capsular closure was not performed at our institute during the inclusion period of this study. If labral damage was encountered intraoperatively, selective labral debridement was performed sparingly to preserve the suction seal between the labrum and femoral head. The labrum was not routinely repaired, as there was not much evidence available during the eligibility period. Cartilage damage was treated by chondroplasty or microfracturing according to the International Cartilage Repair Society (ICRS) stages. In the case of anterior pincer morphology, the anterior rim was carefully trimmed using a round bur without decreasing the amount of anterior bony coverage. Femoroplasty was performed if cam morphology was present.
Psychometric Analyses
The modified Harris Hip Score (mHHS) 5,20,22 was assessed preoperatively and at the latest follow-up (minimum, 10 years). Patients also reported their visual analog scale (VAS) for pain score at these points. To quantify the clinical significance of meaningful outcome achievement, the MCID, SCB, and PASS were calculated for the mHHS. MCID was determined by calculating half of the standard deviation of the mHHS as described by Norman et al. 21,32
The absolute and net change SCB values were calculated using an anchor-based method. 16,36 The net change SCB indicates a change in the outcome measure that is considered substantial, while an absolute SCB indicates an overall outcome score that is substantial. At the latest follow-up, patients were asked the following anchor question: “Since your hip arthroscopy, how would you rate your overall physical ability?” Possible responses were much worse, worse, slightly worse, no change, slightly improved, improved, and much improved. Patients who responded with slightly worse, no change, or slightly improved were designated as the no-change group. The corresponding difference between the no-change group and much-improved group was used to define the SCB. Nineteen patients were assigned to the much-improved group and 17 patients to the no-change group.
PASS was calculated by use of an anchor-based method. Patients were asked the following question at the latest follow-up 7,35 : “Taking into account all the activities you have during your daily life, your level of pain, and also your functional impairment, do you consider that your current state is satisfactory?” Thirty-two of the patients responded yes and 12 responded no.
The SCB and PASS for the mHHS were calculated using a receiver operating characteristic (ROC) curve analysis 3 ; an area under the curve >0.8 was considered predictive of patients who did or did not achieve SCB and PASS. The cutoff point was defined using the Youden Index. 50
To determine whether there are preoperative patient characteristics that may predict achieving the MCID, SCB, and PASS, Spearman correlation analysis and logistic regression analysis were conducted. Variables used in the correlation and regression analyses were age, sex, BMI, smoking status, symptom duration in months before surgery, and radiographic analysis including alpha angle, LCEAm, and Tönnis grade.
Descriptive statistics for all continuous variables were reported as means ± standard deviations. Continuous data were analyzed with independent and paired t tests. The Levene test for variance was performed. Statistical analyses were conducted using SPSS Statistics for Windows (Version 26.0.0; IBM).
Results
Patient Characteristics and Radiographic Measurements
A total of 44 patients met the inclusion criteria and were included in the analysis (Figure 1). There were 61.4% male hips (27/44). The mean age was 42.2 ± 13.3 years (range, 16-67 years), the mean body mass index (BMI) was 22.3 ± 3.01 kg/m2 (range, 16.76-29.78 kg/m2), and the mean follow-up was 11.0 ± 0.8 years (range, 10.0-12.0 years) (Table 1). Four of the 44 hips required revision surgery (3 revision arthroscopies and 1 anteverting periacetabular osteotomy). There have been no complications observed in any of the patients.

Flowchart illustrating the number of patients excluded from the study, lost to follow-up, and who met inclusion criteria. THA, total hip arthroplasty.
Patient Data (N = 44) a
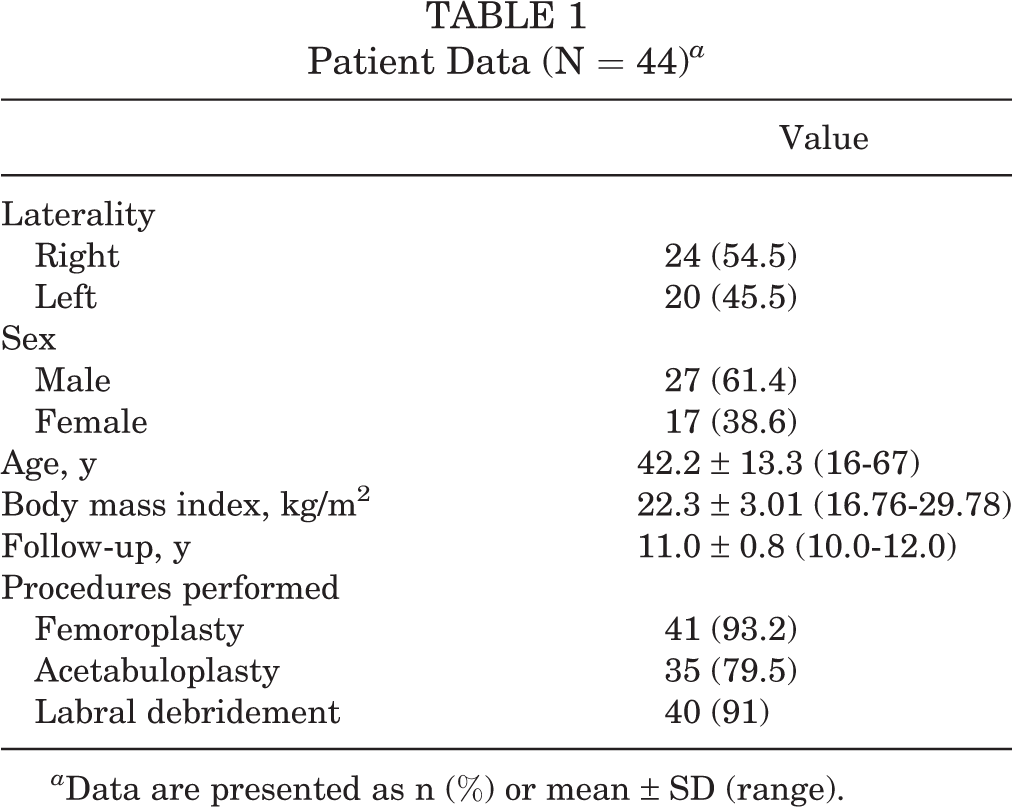
a Data are presented as n (%) or mean ± SD (range).
The majority of hips had preoperative Tönnis grade 1 (32 hips; 72.7%), while the remaining 12 hips (27.3%) had Tönnis grade 0. The mean preoperative alpha angle was 65.6° ± 13.3° (range, 50°-75°), which was significantly reduced to 45.6° ± 4.8° (range, 40°-55°) postoperatively (P < .001). The mean preoperative LCEA was 31.9° ± 4.8° (range, 26°-40°), which was significantly reduced to 28.5° ± 3.5° (range, 26°-35°) postoperatively (P = .001) (Table 2).
Pre- and Postoperative Radiographic Measurements a

a Data are shown as mean ± SD (range) unless otherwise indicated. Boldface P values indicate statistically significant between-group differences (P < .05). LCEA, lateral center-edge angle; NA, not applicable.
Analysis of Pre- Versus Postoperative Reported Outcome Score Measurements
Analysis of preoperative and long-term follow-up reported mHHS values demonstrated statistically significant improvement (55.6 ± 10.4 [range, 11.0-64.4] vs 89.3 ± 10.7 [range, 52.8-100] points; P < .0001). In addition, there was a statistically significant improvement in the VAS score for pain (6.6 ± 1.5 [range, 4-10] vs 2.3 ± 1.3 [range, 0-9] points; P < .0001).
Achievement MCID, SCB, and PASS
The MCID for the mHHS at a mean 11 ± 0.8 years (range, 10.0-12.0 years) of follow-up was 19.6. The ROC curve analysis for calculating the SCB and PASS are provided in Figures 2 to 4. The mHHS threshold scores for achieving absolute SCB, net change SCB, and PASS a mean 11 ± 0.8 years (range, 10.0-12.0 years) of follow-up were 90.1, 31.5, and 84.4, respectively. A total of 39 (89%) patients achieved the MCID mHHS, 26 (59%) achieved the absolute and net change SCB mHHS, and 33 (75%) achieved the PASS mHHS, respectively.

Histogram of the receiver operating characteristic (ROC) curve analysis of the postoperative score distribution for the absolute SCB modified Harris Hip Score (mHHS) (area, 0.833; SE, 0.068; 95% CI, 0.693-0.913; P = .005). SCB, substantial clinical benefit.

Histogram of the receiver operating characteristic (ROC) curve analysis of the postoperative score distribution for the net change SCB modified Harris Hip Score (mHHS) (area, 0.851; SE, 0.080; 95% CI 0.695-0.999; P = .001). SCB, substantial clinical benefit.
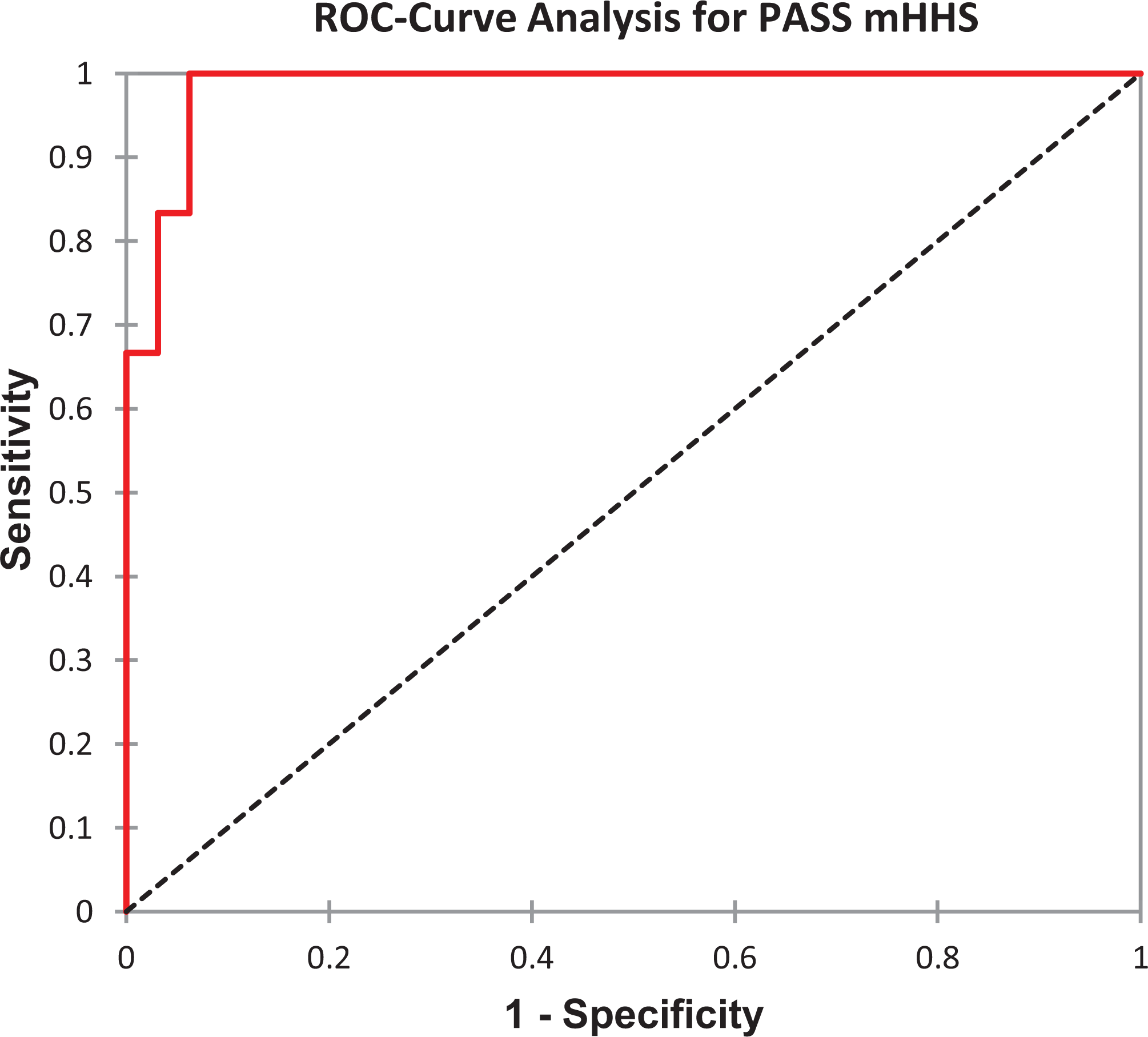
Histogram of the receiver operating characteristic (ROC) curve analysis of the postoperative score distribution for the PASS modified Harris Hip Score (mHHS) (area, 0.984; SE, 0.059; 95% CI 0.723-0.929; P = .005). PASS, patient acceptable symptomatic state.
Correlation and Logistic Regression Analyses
The correlation analysis showed a moderate linear association between preoperative symptom duration and the MCID (P = .024), absolute SCB (P = .001), net change SCB (P = .001), and PASS (P = .001). The mean durations of symptoms for patients who achieved the MCID, absolute SCB, net change SCB, and PASS were 11.7 ± 8.3 months (range, 3.0-18.0 months), 9.1 ± 2.7 months (range, 5.0-15.0 months), 9.0 ± 2.6 months (range, 5.0-15.0 months), and 10.8 ± 8.6 months (range, 3.0-18.0 months), respectively. The mean durations of symptoms for patients who did not achieve the MCID, absolute SCB, net change SCB, and PASS were 15.8 ± 6.1 months (range, 8.0-51.0 months), 17.4 ± 10.8 months (range, 3.0-51.0 months), 17.3 ± 10.7 months (range, 3.0-51.0 months), and 18.4 ± 6.2 months (range, 7.0-51.0 months), respectively. The mean durations of symptoms differed significantly between both groups for MCID, absolute SCB, net change SCB, and PASS (each P < .0001). There were no other statistically significant correlations found between preoperative values and the MCID, absolute SCB, net change SCB, and PASS (P > .05). The correlation analysis is summarized in Table 3.
Correlation Analysis of Preoperative Variables, MCID, SCB, and PASS a

a Boldface P values indicate statistically significant between-group differences (P < .05). BMI, body mass index; LCEA, lateral center-edge angle; MCID, minimal clinically important difference; PASS, patient acceptable symptomatic state; SCB, substantial clinical benefit.
Preoperative predictors of achieving a minimal threshold of meaningful clinical outcome based on MCID included a shorter preoperative pain duration (OR, 0.835; 95% CI, 0.779-1.001; P = .048). None of the other examined variables were found to be independent predictors for achievement of the MCID mHHS. A shorter preoperative pain duration could be identified as a preoperative predictor for achieving a maximum threshold of a meaningful clinical outcome based on absolute SCB (OR, 0.821; 95% CI, 0.720-0.935; P = .003) and net change SCB (OR, 0.819; 95% CI, 0.717-0.930; P = .003), respectively. None of the other examined variables were found to be independent predictors for achievement of absolute SCB or net change SCB mHHS. Preoperative predictors of achieving a higher threshold of meaningful clinical outcome on PASS included a shorter preoperative pain duration (OR, 0.858; 95% CI, 0.764-0.935; P = .009). None of the other examined variables were found to be independent predictors for achievement of PASS mHHS (Table 4).
Binary Logistic Regression Model for MCID, SCB, and PASS a

a Boldface P values indicate statistically significant between-group differences (P < .05). BMI, body mass index; LCEA, lateral center-edge angle; MCID, minimal clinically important difference; PASS, patient acceptable symptomatic state; SCB, substantial clinical benefit.
Discussion
There has been an increased interest in reporting meaningful patient outcomes after arthroscopic treatment of FAIS. Previous studies reported the MCID, SCB, and PASS for the mHHS at short- and medium-term follow-ups. 34,36 However, there are no reports for long-term follow-ups. This study reports the MCID, SCB, and PASS for the mHHS at a minimum 10-year follow-up. The MCID, absolute SCB, net change SCB, and PASS for the mHHS were calculated to be 19.6, 90.1, 31.5, and 84.4 points, respectively. Furthermore, we identified the preoperative duration of symptoms as an independent predictor for achievement of the MCID, SCB, and PASS.
Recent studies showed that patients with a preoperative duration of FAIS-associated symptoms of 2 or more years before hip arthroscopy experience inferior outcomes and a lower frequency of clinically significant outcome improvement than patients with a shorter duration of symptoms at short- or medium-term follow-up. 1,24 Our study confirms these findings at long-term follow-up. Our results show that patients with a longer preoperative duration of symptoms achieved a significantly less MCID, SCB, and PASS for the mHHS compared with patients with a shorter preoperative duration of symptoms. Furthermore, binary logistic regression analysis identified preoperative symptom duration as an independent predictor for MCID, SCB, and PASS achievement. One reason for this may be a worsening of the pathology due to the longer duration of symptoms. In our study, 75% of the hips could be assigned to Tönnis grade 1. This factor is extremely important and must be integrated into the decision-making process to fulfill patients’ expectations. In addition, these findings should encourage physicians to accelerate the transition to surgical treatment of patients undergoing conservative therapy. Other studies reported obesity, smoking, and age as additional risk factors influencing achievement of the MCID, SCB, and PASS. 6,40 Our results could not confirm these findings. Nevertheless, the study group did not include any obese patients (BMI, >30 kg/m2) and the correlation analysis almost reached significance, so that an influence of the BMI on the clinical outcome cannot be excluded with certainty.
The MCID for the mHHS has been described at various time points after hip arthroscopy. However, there was a noticeable spread of the described values. Chahal et al 8 first reported an MCID for the mHHS of 20.1 points 1 year postoperatively. This value 1 year postoperatively is noticeably higher than the MCID of 6.9 points recently described by Nwachukwu et al. 34 One reason could be the method for calculating the MCID. 9,42 While Chahal et al 8 used an anchor-based method, Nwachukwu et al 34 chose a distribution-based method. The anchor-based method has been shown to not being suitable for patients undergoing arthroscopic treatment of FAIS, as most patients report valuable improvements after surgery. 34 In the same study, Nwachukwu et al 34 published a 5-year value for the MCID, which was 11.4 points. Compared with our result, this is slightly lower. Since both studies were performed using a distribution-based method to calculate the MCID, the higher MCID values obtained in our study have a different origin. Nwachukwu et al’s 34 study presented a mean mHHS value of 78.2 points at the 5-year follow-up, compared with our mean mHHS value of 89.3 points at the 10-year follow-up. However, the preoperative values were comparable (57.5 and 55.6 points, respectively). The cause of this difference in MCID could be that the proportion of men was higher in our study (61.4% compared with 36.7%). However, this cannot be determined conclusively. One difference, though, which is evident for the study collectives, is the BMI, which is 4 points higher in the study by Nwachukwu et al 34 compared with our collective (26 versus 22 kg/m2). However, Nwachukwu et al 34 stated only the mean value with standard deviation, so no adequate conclusions can be drawn about the number of obese patients in their study.
Another outcome parameter that has been reported in recent times is the SCB. The absolute values reported in the literature for the mHHS at 1- and 5-year follow-ups are between 82.5 and 94.4 points. 34,36 The SCB of our cohort at the 10-year follow-up is therefore consistent with the values described above. The same applies to the PASS of our cohort, which was determined to be 84.4 points and therefore constant with the values reported in the literature: 84.1 points for the 1-year follow-up and 83.6 points for the 5-year follow-up. 7,34
Limitations
There are some limitations to this study. The small cohort size must be mentioned. On the one hand, this is because hip arthroscopy was in the establishment phase during the investigated time period. On the other hand, though, the indications were more generously defined at that time, so that patients who underwent hip arthroscopy are unlikely to receive arthroscopic treatment today. 11 There is also a high degree of selection within the cohort. Merely hips with no or minimal signs of osteoarthritis (Tönnis grade <2) were included. Similarly, the study population did not include obese patients, so the influence of BMI may be underrepresented, and therefore, a possible influence of BMI or degree of osteoarthrosis could not be adequately assessed. In addition, patients who received subsequent THA were excluded, as the mHHS was not viable for this group. This fact may have led to a missed identification of potential risk factors for failure. A further limitation is the use of the mHHS, for which a high-ceiling effect has been demonstrated. In recent years, other PROMs have been established that seem to be more suitable for younger patients and do not show this ceiling effect. 15,29,44 However, these PROMs had not yet been established, so that existing scores, such as the mHHS, were recorded at that time. Furthermore, the labrum and capsule were not routinely repaired, as there was not much evidence available during the eligibility period. Nowadays the labrum is considered to be preserved because of its biomechanical properties. 18,47 However, Menge et al 31 demonstrated that hip arthroscopy for FAIS with labral debridement or repair resulted in significant improvements in the PROMs and satisfaction of patients who did not eventually require THA at long-term follow-up.
Conclusion
This study reports the MCID, SCB, and PASS for the mHHS for the long-term outcomes of patients undergoing arthroscopic treatment of FAIS. Therefore, we identified the preoperative duration of symptoms as an independent predictor for achievement of the MCID, SCB, and PASS. Patients with a preoperative duration of symptoms longer than 12 months experienced a lower frequency of clinically significant outcome improvements. These findings can be helpful in accelerating the transition to surgical treatment of FAIS.
Footnotes
ACKNOWLEDGMENT
The authors thank Dr Marcus Vollmer (Institute of Bioinformatics, Greifswald, Germany) for his support regarding statistical analysis. We acknowledge support for the Article Processing Charge from the DFG (German Research Foundation, 393148499) and the Open Access Publication Fund of the University of Greifswald.
Final revision submitted August 27, 2020; accepted September 21, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: W.M. has received personal fees from Arthrex and Richard Wolf. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the regional ethics committee of Baden-Württemberg, Germany (ref No. F-2019-006).