
Abstract
Background:
Osteochondral allograft (OCA) transplantation has evolved into a first-line treatment for large chondral and osteochondral defects, aided by advancements in storage protocols and a growing body of clinical evidence supporting successful clinical outcomes and long-term survivorship. Despite the body of literature supporting OCAs, there still remains controversy and debate in the surgical application of OCA, especially where high-level evidence is lacking.
Purpose:
To develop consensus among an expert group with extensive clinical and scientific experience in OCA, addressing controversies in the treatment of chondral and osteochondral defects with OCA transplantation.
Study Design:
Consensus statement.
Methods:
A focus group of clinical experts on OCA cartilage restoration participated in a 3-round modified Delphi process to generate a list of statements and establish consensus. Questions and statements were initially developed on specific topics that lack scientific evidence and lead to debate and controversy in the clinical community. In-person discussion occurred where statements were not agreed on after 2 rounds of voting. After final voting, the percentage of agreement and level of consensus were characterized. A systematic literature review was performed, and the level of evidence and grade were established for each statement.
Results:
Seventeen statements spanning surgical technique, graft matching, indications, and rehabilitation reached consensus after the final round of voting. Of the 17 statements that reached consensus, 11 received unanimous (100%) agreement, and 6 received strong (80%-99%) agreement.
Conclusion:
The outcomes of this study led to the establishment of consensus statements that provide guidance on surgical and perioperative management of OCAs. The findings also provided insights on topics requiring more research or high-quality studies to further establish consensus and provide stronger evidence.
The popularity of fresh osteochondral allograft (OCA) transplantation has increased substantially over the past decade given its long-term success, with survivorship of ∼90% at 5 years and ∼75% at 10 years. 8,11 Several decades of translational studies have helped identify appropriate patient indications, # improve graft storage and processing, 28,62 –64 and provide a body of literature reporting successful clinical results and long-term graft survivorship in patients treated with OCAs. ** Despite the current evidence supporting its use, there remain areas of controversy and debate in the nuances of OCA application. Parameters of patient selection, contraindications, surgical technique, graft matching procedures, and rehabilitation protocols vary within the orthopaedic community. The current literature lacks quality evidence and comparative studies. Given these limitations and the lack of standardization across the clinical community, it is important to establish consensus on issues surrounding OCA transplantation of the knee.
It has been shown that, in the absence of consistent and objective conclusions from the literature, consensus criteria can be established by leveraging expert opinion and clinician experience through a Delphi approach. This type of process has been reported for various treatment/management controversies in the field of orthopaedics. 18,51,72 A group of the most highly experienced surgeons (experts), selected for their contribution to the science and clinical application of OCA, was assembled to identify and address areas of standards of care and controversy in OCA surgery and subsequently develop consensus statements through the Delphi method. The goal of this process was to establish evidence-based consensus statements regarding indications, surgical technique, graft matching, and rehabilitation and return-to-sport recommendations. The level of consensus and evidence in these categories were analyzed to provide guidance where data were inconclusive and to identify areas that would benefit from further research to improve knowledge and quality of evidence. The aim was to assist clinicians in making decisions involving OCA transplantation application and patient care.
Methods
Modified Delphi Method
A focus group of 23 experts was convened in 2018 to address controversies and identify areas of research opportunity for various clinical, scientific, and technical aspects of OCA transplantation. The expert group included the highest-volume surgeons, all performing >30 OCA transplantations per year (JRF Ortho Tissue Bank data) and all previously selected to participate in the Metrics of OsteoChondral Allografts (MOCA) Committee based on contributions to the science of OCA. MOCA is a working group dedicated to improving OCA restoration through outcomes and translational research. The group identified 4 main topic areas in an effort to address unanswered clinical discrepancies in the literature and questions among the clinical community for OCA cartilage restoration: (1) indications, (2) surgical technique, (3) graft matching, and (4) rehabilitation and return to sport. A modification of the Delphi method, with 3 rounds of voting, was used to develop the consensus statements and establish agreement among the group. 50 The level of consensus was measured for each statement and defined as follows: consensus, 66.6% to 79%; strong consensus, 80% to 99%; and unanimous consensus, 100%. Details of the modified Delphi process are outlined in the Appendix.
Systematic Literature Search
A comprehensive systematic literature search was conducted to determine the level of evidence (LOE) of the supporting literature. PubMed/MEDLINE were reviewed from inception to April 2019. A general search strategy was followed by specific search terms using defined inclusion/exclusion criteria to screen and identify supporting peer-reviewed articles for each topic area of the generated consensus statements (Appendix). In total, 75 articles were identified that addressed OCA procedures and/or use of the Delphi method in the orthopaedic literature. These were used as the basis to construct the first round of questions and were then linked to support each statement as appropriate.
Quality of Statements
The quality and grade of each statement were evaluated by measuring the LOE using the Centre for Evidence-Based Medicine’s LOE and grades of recommendation. Two authors (S.G., S.M.T.) independently reviewed the LOE and grade for each statement and resolved any differences. The LOE and grades of recommendation are described in the Appendix.
Results
Delphi Process Results
The 23 experts completed round 1 of the Delphi process (100% response rate), consisting of statements addressing key and/or empirically controversial areas in osteochondral allografting. After round 1 voting, the comments were summarized, and 15 additional statements were included in the round 2 survey; responses were requested within a 2-week time frame. A total of 21 experts completed round 2 of the survey within this time frame (91% response rate). The outcomes of round 2 led to the modification of 2 statements and the removal of 4 redundant statements. The final round was completed by 18 experts, who attended the 2018 MOCA meeting in person or participated remotely via mobile app (78% response rate) (Table 1).
Modified Delphi Process Results to Establish Consensus on Osteochondral Allografts

Comments from committee members were used to modify preliminary statements or add new statements in round 2, to find common ground. In round 3, statements were again modified or culled to remove redundancy or overlap in ideas. Of the 25 preliminary statements voted on during the final round, 13 were modified and 8 were tabled. Of the 17 statements that reached consensus, 11 received unanimous agreement (100% agreement) and 6 received strong agreement (80%-99% agreement). The percentage of agreement and level of consensus for the final statements by category (indications, surgical technique, graft matching, and rehabilitation and return to sport) are summarized in Table 2.
Percentage of Agreement and Level of Consensus for Final Statements by Category a

a OCA, osteochondral allograft; OCD, osteochondritis dissecans.
Indications for Osteochondral Allografting
Level and Grade of Evidence
In the indications category, 5 statements reached strong or unanimous consensus. Of these statements, 1 was supported by level 2, level 3, and level 4 studies, and 3 statements were supported by level 3 and/or level 4 studies (grade C). One statement was expert opinion of the focus group (grade D) (Table 3).
Level of Evidence and Grade of Evidence for Indications for OCA a

a OCA, osteochondral allograft; OCD, osteochondritis dissecans.
Evidence Summary
The efficacy of OCAs for the treatment of osteochondral lesions is well established in the clinical community and supported by a substantial body of literature. Numerous studies have evaluated OCAs for various indications. †† All experts of this focus group concurred that symptomatic osteochondral defects secondary to trauma, osteochondritis dissecans (OCD), osteonecrosis, and intra-articular fractures are appropriately treated with OCA. A recent systematic review demonstrated improved patient-reported outcomes and a mean survival rate of 78.7% at 10 years in OCAs of the knee for traumatic and degenerative chondral lesions, OCD, steroid-associated and spontaneous osteonecrosis, and osteoarthritis. 23 It was the unanimous consensus that contraindications include uncorrected ligamentous instability, uncorrected contributory malalignment, and advanced osteoarthritis, except in rare instances as a bridging procedure. This is supported by literature demonstrating higher failure rates of OCAs in patients with uncorrected limb malalignment and advanced osteoarthritis. 30,36,44,55,57,71 Additionally, a histological analysis of retrieved failed OCAs revealed a high presence of inflammatory cells and mediators associated with systemic inflammatory diseases in early and late failures of OCAs. 36
Although there is a lack of consensus in the clinical community on surgical treatment algorithms for OCD, 67 the study participants strongly agreed (94%) that OCAs can be a primary treatment option for OCD. This result aligns with a number of studies that demonstrate improved patient outcomes, return to sport, and >90% graft survivorship at 5 years for treatment of OCD with fresh OCAs. 8,22,27,52,67,78 Specifically, Sadr et al 67 and Emmerson et al 22 demonstrated 95% and 91% graft survivorship at 5 years and 93% and 76% at 10 years, respectively. A recent study evaluating the association between patient satisfaction and clinical outcomes of patients treated with OCA showed a high and predictable satisfaction rate (95.6%) associated with outcomes for patients who underwent OCA for OCD. 78
Additionally, a robust body of literature supported the statement that OCAs can be used to revise previously failed cartilage restoration procedures. 17,32,34,39,46,56,76,86 Of these studies, a comparison of outcomes after primary OCA versus revision OCA after a failed cartilage procedure showed no significant difference and similar survival rates between the 2 cohorts. 32,39,56 A recent systematic review investigating outcomes of revision cartilage restoration procedures demonstrated that revision OCA consistently had similar results to primary OCA transplantation, even if the subchondral bone was affected. 46
Surgical Technique
Level and Grade of Evidence
The surgical technique category consisted of 5 statements that reached consensus and were graded as C or D (Table 4). Four statements were expert opinion or supported by basic science studies (grade D), and 1 of the 5 statements was supported by level 3, level 4, and level 5 studies (grade C).
Level of Evidence and Grade of Evidence for Surgical Technique a

a OCA, osteochondral allograft.
Evidence Summary
Although the surgical technique statements were limited by clinical evidence, fixation of unstable grafts and the surgical management of subchondral cysts beneath surface lesions were critical technical considerations that may affect graft success. Based on expert opinion and extensive clinical experience, the focus group agreed (94%) that supplemental fixation of an OCA is needed only if the graft is unstable, as might be the case in grafts that are not circumferentially contained and do not achieve a press fit. Despite the absence of evidence, there are several case series detailing the use of fixation to manage unstable grafts. 8,31,35 Additionally, unanimous consensus was established for addressing bony cysts beneath a lesion at the time of osteochondral allografting. While there is no specific clinical literature regarding management of cysts, all experts concurred that these should be addressed with curettage and bone grafting, preferably with autologous bone graft generated during host graft bed preparation. The discussions of surgical technique also led to the unanimous consensus of the ideal depth of a femoral OCA to measure between 6 and 10 mm. Wang et al 86 detailed the use of OCAs with a bone depth between 8 and 10 mm. A more recent article evaluating OCA bone depth concluded that 7 and 10 mm--length plugs had significantly better resistance to pullout and subsidence than the 4 mm--deep plugs. 4
With regard to pulsatile lavage, several articles have evaluated the effectiveness of using pulse lavage on allografts to remove marrow elements and debris, 38,41,75 which is considered important to decreasing their potential immunogenicity and bioburden. Ibrahim et al 41 demonstrated that pulse lavage removed a significant amount of marrow content from morselized allograft bone—protein (70.5%), fat (95.2%), and DNA content (68.4%). A more recent study investigated the effect of lavage duration, flow intensity, and graft storage conditions on the extent of marrow removal from human osteochondral cores and showed increased marrow removal with greater lavage durations. 75 Besides reducing the immunogenicity of the graft, removal of marrow elements may also improve bone integration. A goat model showed increased bone ingrowth after rinsing allografts, suggesting that reduction of immunogenic factors in the marrow may improve bone incorporation. 81 With regard to biologic adjuncts enhancing bone incorporation of OCAs, the evidence is lacking and inconsistent. Two studies investigated the effects of autologous bone marrow aspirate concentrate (BMAC) on bone integration. 61,85 In the first study, OCA augmented with BMAC did not enhance bone integration or affect cystic changes as compared with OCA without BMAC, 85 contradicting the findings of the second, which showed improved bone integration in the OCA group containing BMAC. 61 Various factors may influence outcomes, including methods to assess osseous integration, patient selection, graft matching, and BMAC harvesting technique and processing. The contradictory results in the literature support the need for additional research to understand the role and determine the effectiveness of biologic adjuncts in OCA.
Graft Matching
Level and Grade of Evidence
Of the 4 statements established for the graft-matching category (Table 5), 2 were supported by comparative clinical (level 3) and basic science (level 5) studies (grade C). The remaining 2 statements were expert opinion or supported by basic science studies (grade D).
Level of Evidence and Grade of Evidence for Graft Matching a

a CT, computed tomography; MRI, magnetic resonance imaging; OCA, osteochondral allograft.
Evidence Summary
There was strong consensus on defining the contralateral graft as an OCA from the opposite condyle and allowing its use for single-plug restoration. This has ramifications for optimizing donor tissue utilization, as the preponderance of lesions of the medial femoral condyle (MFC) in patients leads to a relative shortage of MFC grafts and a related surplus of lateral femoral condylar (LFC) grafts. The evidence supporting the use of a contralateral/nonorthotopic OCA for a single-dowel restoration has increased in recent years. Mologne et al 58 investigated OCA surface matching of LFC grafts into MFC 20-mm defects. The outcomes showed that MFC and LFC donors matched well, with an overall height deviation of 0.63 mm for area and 0.47 mm for stepoff, with no significant difference between them. These results are consistent with more recent studies demonstrating that a contralateral LFC graft can provide acceptable size and similar surface matching with MFC grafts. 80,88 These cadaveric studies were corroborated in a recent clinical study (level 3) comparing clinical outcomes of nonorthotopic or contralateral OCAs with traditional site-matched orthotopic OCAs. 80 Both patient groups significantly improved clinically with no significant differences in failure rates and patient-reported outcomes, suggesting that condyle-specific matching is not necessary.
This growing body of literature evaluating contour, topography, and graft matching of OCAs in various cadaveric studies supports the width measurement of the femoral condyle or tibial plateau as the standard for size matching OCAs. 7,58,80,88 The experts strongly agree that femoral condyles can be adequately size matched using condylar and/or tibia width measured on radiographs with magnification correction or magnetic resonance imaging/computed tomography. A recent clinical study showed that graft-recipient anteroposterior mismatch was not associated with OCA failure or patient outcomes, suggesting that anteroposterior length mismatch is not an absolute contraindication for graft acceptance. 82
With regard to cartilage viability, all experts concurred that a standardized method for testing cartilage viability and metabolic activity should be established. Chondrocyte viability is considered critical for durable osteochondral restoration, survivorship, and long-term outcomes. Pallante et al 63 investigated the effect of various OCA storage parameters on graft health using an in vivo goat model and demonstrated that reduced chondrocyte cellularity at the articular surface of OCAs at the time of implantation, as a result of various storage conditions, was associated with poor outcomes at 12 months. The importance of chondrocyte viability on successful osteochondral repair was supported in a canine in vivo model 73 demonstrating successful osteochondral repair with donor OCAs containing >70% chondrocyte viability and poor outcomes with grafts <70% viability. Gross et al 36 conducted a histological analysis of fresh OCA specimens retrieved at the time of revision surgery, which ranged from 1 to 25 years after the index OCA procedure, and demonstrated an association between viable chondrocytes and long-term graft survival. The histological analysis of early graft failures showed a lack of viable chondrocytes and cartilage and matrix staining, 36 consistent with the animal data.
Rehabilitation and Return to Sports
Level and Grade of Evidence
Out of the 3 statements established for the “rehabilitation and return to sports” category (Table 6), 2 statements were supported by level 4 clinical studies (grade C), and 1 was based on expert opinion of the focus group (grade D).
Level of Evidence and Grade of Evidence for Rehabilitation and Return to Sports a
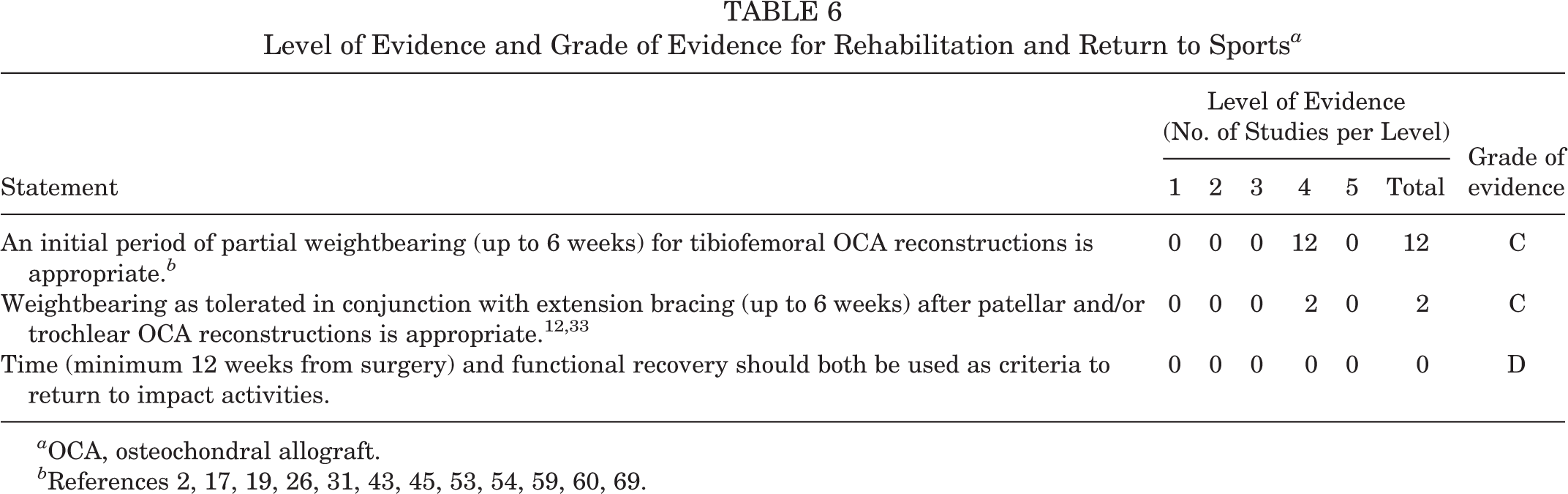
a OCA, osteochondral allograft.
Evidence Summary
Unanimous consensus was reached for all statements related to rehabilitation and return to sport. Various rehabilitation protocols and guidelines have been reported after OCA transplantation of the distal femur. The majority of studies before 2017 favored more restrictive postoperative weightbearing instructions, typically characterized as nonweightbearing initially for 6 to 8 weeks or a slow progression of toe-touch weightbearing (TTWB) during the initial convalescence. ‡‡ Studies published in 2017 and later generally reported more permissive postoperative weightbearing protocols in comparison with historic recommendations of strict nonweightbearing. 1,25,26,60,84 Nielsen et al 60 prescribed 4 to 6 weeks of TTWB, followed by a month of progressive weightbearing, and Frank et al 25,26 allowed immediate partial weightbearing with a hinged brace for 4 to 6 weeks. All subsequently reported significant improvement in patient-reported outcomes. 25,26 These recent studies aside however, a moderately restrictive weightbearing protocol after distal femur OCA transplants is most common and is supported by the results of this expert focus group.
With regard to rehabilitation protocols after patellar and trochlear reconstructions with OCAs, few studies exclusively focused on postoperative rehabilitation in the patellofemoral region. Although many reports included surgery in this anatomic area, at the patella, 10,14,55 trochlea, 12,19,45 or both, 1,25,26,60,84 few specified rehabilitation protocols in this subset. Cameron et al 12 reported on a cohort of trochlear allograft recipients who were permitted TTWB with a brace limiting knee flexion to <45° and progressive weightbearing by 8 to 10 weeks, depending on quadriceps function. They reported a graft survivorship of 78% at 5 years and 55.8% at 15 years, with significantly improved outcome scores. Although there are limited studies evaluating rehabilitation in the patellar and trochlear regions, the evidence is consistent with the established consensus statement. All respondents agreed that rehabilitation after OCA reconstruction of the patellofemoral region should include weightbearing as tolerated in conjunction with extension bracing (up to 6 weeks).
This consensus group agreed that time (minimum 12 weeks from surgery) and functional recovery should both be used as criteria to return to loading activities. Several studies addressed timing of return to impact activity and/or sport specifically. Universally, for sports, this is never before 3 months and more typically 4 to 6 months after an OCA transplant, generally with deference to functional capacity restoration. §§
Discussion
The major outcome of this study was the development of consensus (>89% agreement) for 17 statements spanning surgical indications, graft matching, surgical technique, and rehabilitation/return to sport for OCA transplantation of the knee (Appendix). All but 1 statement in the indications category reached unanimous consensus. All experts agreed on appropriate indications, contraindications, and use of OCAs for primary and revision cartilage procedures. The evidence for this category was much greater than any other, which facilitated the high level of agreement. Numerous level 2, 3, and 4 studies spanning 2 decades supported the statements on patient indications. The statements in the surgical technique category were limited by lack of high-quality studies. Despite the paucity of evidence, most or all experts were in agreement on addressing unstable grafts and subchondral cysts intraoperatively. Most participants agreed that subchondral bone cysts underlying index chondral lesions should be selectively curetted during graft bed preparation, rather than coring the entire recipient socket to the depth of the cysts. While the use of pulsatile lavage was universally recommended, further work is necessary to evaluate the effects of marrow removal on immunogenicity and bony integration of OCAs, as well as the optimal irrigant, volume, duration, pressure, and potential additives such as antibiotics. Given the limited and inconsistent literature evaluating the augmentation of OCAs with biologics, 61,85 the expert members all agreed that it is unknown if biologic adjuncts can enhance OCA bone incorporation and that this requires additional investigation.
Strong and unanimous consensus was established for all statements related to graft matching. All experts were in agreement on the utilization of contralateral grafts. A number of cadaveric studies and a level 3 clinical investigation corroborated this statement and validated empirical clinical practice. MOCA experts all agreed that chondrocyte viability corresponds to graft efficacy and outcomes and that a standardized method for testing viability and metabolic activity should be established, as currently there remains significant variability in assays and methodology. The category on rehabilitation and return to sports achieved unanimous consensus on all statements. Experts concurred on an initial period of protected weightbearing after OCA surgery, and most agreed that this could be advanced as tolerated for single well-contained dowel grafts. Grafts in the patellofemoral joint were unanimously felt to be amenable to weightbearing in extension, where the patella does not engage the trochlear groove. Of note, time and functional recovery were considered paramount over radiographic or other imaging parameters in determining return to impact loading.
The strengths of this study include the ability to leverage the MOCA Committee, consisting of leaders and experts in the field of OCAs, to develop the consensus statements. The use of the online surveys and methodology for executing the Delphi process allowed for blinded anonymous results of each round to provide transparency while avoiding any bias or bandwagon effect. The methodology also involved a systematic review of the literature to determine the quality of evidence for each statement. This analysis provided insights into areas lacking robust clinical data and opportunities for additional research to improve the quality of evidence and further the scientific understanding of OCAs. The in-person debate allowed for active exchange and the opportunity to discuss various viewpoints and the supporting evidence for those opinions.
While consensus statements provide a mechanism to address inconsistencies and controversies in the clinical community when evidence is lacking, there are limitations. A significant limitation of this study is the risk of nonresponse bias. Rounds 1 and 2 resulted in 100% and 91% response rates, respectively, and the final round resulted in a lower rate of 78%. Another potential source of bias was the method used to generate questions for the study. This process did not involve all members of the expert group and was not conducted anonymously. In this study, methods were implemented to avoid bias, including distributing all survey results, agreement percentages, consensus statements, and comments to the entire group anonymously after each round. While all the statements reached consensus and may be useful for understanding and guiding various aspects of OCA transplantation, it is not a conclusive standard that can address all aspects of treating chondral lesions. Recent, ongoing, and future studies continue to provide insights and evidence to support the use of OCAs for various indications and to drive improvements in surgical technique, graft matching, and rehabilitation protocols. The consensus statements will be updated when high-quality evidence is available to corroborate the statements, and further studies are needed to address additional areas of debate.
Conclusion
The main findings of this study led to the establishment of consensus statements to provide guidance on surgical management of chondral lesions with OCA transplantation. Unanimous agreement was established for statements describing indications and contraindications for OCA application, which were supported by clinical evidence. Despite limited evidence supporting management of cysts and unstable grafts, unanimous agreement was achieved. Consensus was established for further studies to understand and determine the efficacy of pulse lavage and biologic adjuncts for OCAs. The inconsistencies in the literature regarding assays and methodologies for testing chondrocyte viability led to the unanimous call for standardized methods for testing chondrocyte viability and metabolic activity. The consensus statements developed around graft matching were supported by recent cadaveric and clinical studies. Unanimous agreement was achieved for all statements describing rehabilitation and return to sports, despite the limited literature. Although strong and unanimous consensus was achieved in this study, many statements lacked directive-type evidence and highlight the need for high-quality clinical trials and data sharing, to substantiate these recommendations.
Footnotes
Authors
Simon Görtz, MD (Brigham and Women’s Hospital, Boston, Massachusetts, USA); Suzanne M. Tabbaa, PhD (University of California, San Francisco, San Francisco, California, USA); Deryk G. Jones, MD (Ochsner Sports Medicine Institute, Jefferson, Louisiana, USA); John D. Polousky, MD (Children’s Health Andrews Institute for Orthopedics and Sports Medicine, Plano, Texas, USA); Dennis C. Crawford, MD, PhD (Oregon Health and Science University, Portland, Oregon, USA); and Metrics of OsteoChondral Allografts (MOCA) Group Collaborators: William D. Bugbee, MD (Shiley Center for Orthopaedic Research and Education, Scripps Clinic, La Jolla, California, USA); Brian J. Cole, MD, MBA (Midwest Orthopaedics at Rush, Chicago, Illinois, USA); Jack Farr, MD (OrthoIndy, Indianapolis, Indiana, USA); James E. Fleischli, MD (OrthoCarolina Sports Medicine Center, Charlotte, North Carolina, USA); Alan Getgood, MD (Fowler Kennedy Sport Medicine Clinic, Western University, London, Ontario, Canada); Andreas H. Gomoll, MD (Hospital for Special Surgery, New York, New York, USA); Allan E. Gross, MD (Mount Sinai Hospital, University of Toronto, Toronto, Ontario, Canada); Aaron J. Krych, MD (Mayo Clinic, Rochester, Minnesota, USA); Christian Lattermann, MD (Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts, USA); Bert R. Mandelbaum, MD (Santa Monica Orthopaedic and Sports Medicine Group, Santa Monica, California, USA); Peter R. Mandt, MD (Proliance Orthopaedics and Sports Medicine, Issaquah, Washington, USA); Raffy Mirzayan, MD (Kaiser Permanente, Baldwin Park, California, USA); Timothy S. Mologne, MD (Orthopedic and Sports Institute, Appleton, Wisconsin, USA); Matthew T. Provencher, MD, Capt MC, USNR (Steadman Philippon Research Institute, Vail, Colorado, USA); Scott A. Rodeo, MD (Hospital for Special Surgery, New York, New York, USA); Oleg Safir, MD (Mount Sinai Hospital, University of Toronto, Toronto, Ontario, Canada); Eric D. Strauss, MD (New York University Langone Health, New York, New York, USA); Christopher J. Wahl, MD (Orthopaedic Physician Associates, Seattle, Washington, USA); Riley J. Williams 3rd, MD (Hospital for Special Surgery, New York, New York, USA); Adam B. Yanke, MD, PhD (Midwest Orthopaedics at Rush, Chicago, Illinois, USA).
Final revision submitted July 10, 2020; accepted July 31, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.G. has received education payments from Arthrex and Goode Surgical, consulting fees from JRF, and honoraria from JRF and Vericel. D.G.J. has received education payments from Arthrex; consulting fees from Acumed, Amniox Medical, Aastrom BioSciences, and Medical Device Business Services; speaking fees from Aastrom BioSciences and Linvatec; honoraria from Flexion, Musculoskeletal Transplant Foundation, and Vericel; and hospitality payments form Aesculap and Zimmer Biomet. J.D.P. has received education payments from Pylant Medical. D.C.C. has received consulting fees from Arthrosurface and DePuy, honoraria from JRF, and hospitality payments from Steelhead Surgical. W.D.B. has received consulting fees from Arthrex, Encore Medical, JRF, DePuy/Medical Device Business Services, and Orthalign; has received royalties from DePuy, Smith & Nephew, and Zimmer Biomet; and has stock/stock options in Orthalign. B.J.C. has received education payments from Medwest; consulting fees from Acumed, Aesculap Biologics, Anika Therapeutics, Arthrex, Bioventus, Flexion Therapeutics, Geistlich Pharma, Smith & Nephew, Vericel, and Zimmer Biomet; speaking fees from Arthrex and Lifenet Health; hospitality payments from GE Healthcare; honoraria from Vericel; and royalties from Arthrex and DJO. J.F. has received education payments from Crossroads Orthopedics; consulting fees from Aastrom Biosciences, Aesculap, Arthrex, Collagen Matrix, Exactech, DePuy, Organogenesis, and RTI Surgical; nonconsulting fees from Arthrex and Vericel; honoraria from JRF and Vericel; royalties from DePuy and Organogenesis; and hospitality payments from Skeletal Kinetics. J.E.F. has received education payments from Peerless Surgical, Linvatec, and Zimmer Biomet and consulting and nonconsulting fees from Smith & Nephew. A.H.G. has received consulting fees from Aastrom, Flexion, JRF, Smith & Nephew, and Vericel; nonconsulting fees from Aastrom and LifeNet Health; honoraria from Fidia Pharma, JRF, and Vericel; and royalties from Organogenesis. A.J.K. has received grant support from Exactech; consulting fees from Arthrex, JRF, and Responsive Arthroscopy; honoraria from JRF, MTF, and Vericel; and royalties from Arthrex. C.L. has received consulting fees from Aastrom, Sanofi-Aventis, Vericel, and Zimmer Biomet; nonconsulting fees from Aesculap, Arthrosurface, and Vericel; and honoraria from Arthrosurface, JRF, and Vericel. B.R.M. has received education payments from Arthrex; consulting fees from Arthrex, BioMarin Pharmaceutical, DePuy, and Exactech; and nonconsulting fees from Arthrex. P.R.M. has received hospitality payments from Arthrex. R.M. has received education payments from Arthrex and SportsTek Medical, nonconsulting fees from Arthrex, and royalties from Zimmer Biomet. T.S.M. has received education support from Arthrex and consulting fees and honoraria from JRF. M.T.P. has received consulting fees, speaking fees, and royalties from Arthrex; royalties from Arthrosurface; honoraria from Flexion; and consulting fees and honoraria from JRF. S.A.R. has received consulting fees from Flexion Therapeutics, nonconsulting fees from Smith & Nephew, honoraria from Fidia Pharma, and royalties from Zimmer Biomet. E.D.S. has received education payments from Arthrex and hospitality payments from Axogen and Liberty Surgical. C.J.W. has received consulting fees and nonconsulting fees from Smith & Nephew, royalties from Arthrosurface, and hospitality payments from Arthrex and Stryker. R.J.W. has received education payments, nonconsulting fees, consulting fees, and royalties from Arthrex. A.B.Y. has received education payments from Arthrex and Medwest, consulting fees from Aastrom Biosciences and Olympus, and honoraria from JRF. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.