
Abstract
Background:
While previous studies have established several techniques for suture anchor repair of the acetabular labrum to bone during arthroscopic surgery, the current literature lacks evidence defining the appropriate number of suture anchors required to effectively restore the function of the labral tissue.
Purpose/Hypothesis:
To define the location and size of labral tears identified during hip arthroscopy for acetabular labral treatment in a large multicenter cohort. The secondary purpose was to differentiate the number of anchors used during arthroscopic labral repair. The hypothesis was that the location and size of the labral tear as well as the number of anchors identified would provide a range of fixation density per acetabular region and fixation method to be used as a guide in performing arthroscopic repair.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
We used a multicenter registry of prospectively collected hip arthroscopy cases to find patients who underwent arthroscopic labral repair by 1 of 7 orthopaedic surgeons between January 2015 and January 2017. The tear location and number of anchors used during repair were described using the clockface method, where 3 o’clock denoted the anterior extent of the tear and 9 o’clock the posterior extent, regardless of sidedness (left or right). Tear size was denoted as the number of “hours” spanned per clockface arc. Chi-square and univariate analyses of variance were performed to evaluate the data for both the entire group and among surgical centers.
Results:
A total of 1978 hips underwent arthroscopic treatment of the acetabular labrum; the most common tear size had a 3-hour span (n = 820; 41.5%). Of these hips, 1645 received labral repair, with most common repair location at the 12- to 3-o’clock position (n = 537; 32.6%). The surgeons varied in number of anchors per repair according to labral size (P < .001 for all), using 1 to 1.6 anchors for 1-hour tears, 1.7 to 2.4 anchors for 2-hour tears, 2.1 to 3.2 anchors for 3-hour tears, and 2.2 to 4.1 for 4-hour tears.
Conclusion:
Variation existed in the number of anchor implants per tear size. When labral repair involved a mean clockface arc >2 hours, at least 2 anchor points were fixated.
Open dislocation and hip arthroscopic techniques are utilized to address structural abnormalities, relieve pain, improve the functional ability of patients during activity, and preserve the hip joint from further structural damage. 23 Commonly performed procedures to address chondrolabral pathologies during surgical intervention include debridement, repair, and/or reconstruction of acetabular labral tears. 11,16 Previous studies of open and arthroscopic surgery for treatment of labral tears with repair versus selective or total debridement have demonstrated superiority of repair on clinical outcomes. 1,14,15,18,19 Histologic evidence of healing has been shown in a limited amount of studies evaluating labral repairs. 2,22 No current standard exists defining the minimal number of fixation points for repair of the acetabular labrum.
Previous studies have established several techniques for suture anchor refixation or repair of the acetabular labrum to bone during arthroscopic and open hip preservation surgery. 9,20,25,26 Current techniques preserve the chondrolabral junction and reconstitute the labrum in a new anatomic footprint to efficiently preserve blood flow and increase the likelihood of healing. 5,20 These techniques strive to reduce the risk of drill and anchor penetration while restoring the chondrolabral interface. 5,26 While care has been shown in developing anatomic repairs, the current literature lacks basic scientific evidence defining the appropriate number of suture anchors required to effectively preserve the function of the labral tissue.
Blankenbaker et al 4 introduced the concept of using a clockface to localize labral injury along the acetabular rim at the time of arthroscopy, in which the arc of the acetabulum involved in repair is described qualitatively using a clockface. The primary purpose of this study was to use the clockface method to define the location and size of acetabular labral tears identified during hip arthroscopy in a large multicenter cohort. Our secondary purpose was to identify the number of anchors used during labral repair, stratified by tear classification. The hypothesis was that the location and size of the labral tear as well as the number of anchors identified in this study would provide a range of fixation density per acetabular region and fixation method, which could be used as a guide in performing arthroscopic repair of the acetabular labrum.
Methods
A multicenter registry of prospectively collected hip arthroscopic cases was used to determine the location and size of labral tears and the number of anchors performed during arthroscopic labral repair from January 2015 to January 2017. The database registry is maintained by the MASH (Multicenter Arthroscopic Study of the Hip) study group, composed of 7 board-certified orthopaedic surgeons in the United States (J.J.C., S.J.N., A.B.W., J.P.S., D.M., T.J.E., D.S.C.) with >300 cases completed before enrollment and annual case volumes of >100 cases. At each participating center, institutional review board approval was granted for a priori collection and storage of agreed-upon deidentified clinical data points.
An a priori set of labral repair details was agreed on by all investigators for the purposes of record keeping (Table 1). The investigators decided upon prospective clinical decision-making per the standard of care in their own practices. Surgeons recorded the extent of anteromedial and posterolateral labral injury, describing the arc of the acetabulum involved in repair per the clockface method. 4 As a standard, the 3-o’clock position was used to denote the anterior extent and the 9-o’clock position the posterior extent, regardless of sidedness (left or right). The size of the tear was described using the number of “hours” spanned by the clockface arc. The number of anchors per repair was also recorded on the clockface according to tear location and extent. All anchors were single-loaded. The pattern of anchor passage through the labrum was not recorded, and no a priori intra- or interrater analysis was performed for clockface classification of labral tears.
MASH Study Group Labral Repair Data Points (Determined Intraoperatively) a

a MASH, Multicenter Arthroscopic Study of the Hip.
b The arc of the acetabulum involved in repair was described qualitatively using a clockface, where the 3-o’clock position was used to denote the anterior extent and the 9-o’clock position the posterior extent, regardless of sidedness (left or right). Size was described as number of clockface “hours.”
c Labral tear complexity was determined qualitatively by all investigators according to an agreed-on system of classification: mild = no disruption of labral base or capsulolabral tissue / minimal intrasubstance damage; moderate = disruption of capsulolabral or labral base tissue / minimal intrasubstance damage; severe = disruption of labral base and capsulolabral integrity / severe intrasubstance damage.
The research data for the current study were deidentified so that patients could not be identified directly or through linked identifiers. A retrospective data analysis was performed for all patients who had acetabular labral pathology addressed by hip arthroscopy. Inclusion criteria were patients who had undergone arthroscopic labral treatment and the intraoperative size and location of the labral tear recorded descriptively using the clockface method. 4 Patients with incomplete or missing data were excluded from the respective analyses.
Statistical Analysis
Demographic information was attained, while descriptive analysis was performed for the location and size (clockface description) of the tear and number of anchors used in the repair for each size. A chi-square analysis was performed to establish the prevalence of categorical data that included the location and size of the labral tear. Univariate analyses of variances were performed to determine the effect of the surgical center on the number of anchors used for surgical repair. All statistical analysis was performed with an a priori alpha set to P < .05. All data were analyzed using common statistical software (SPSS Statistics Version 25; IBM).
Results
Patients
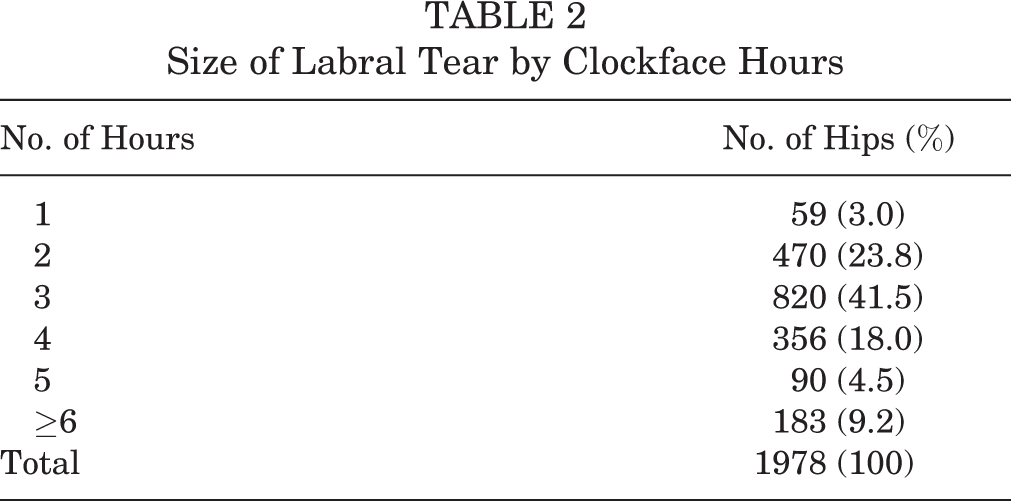
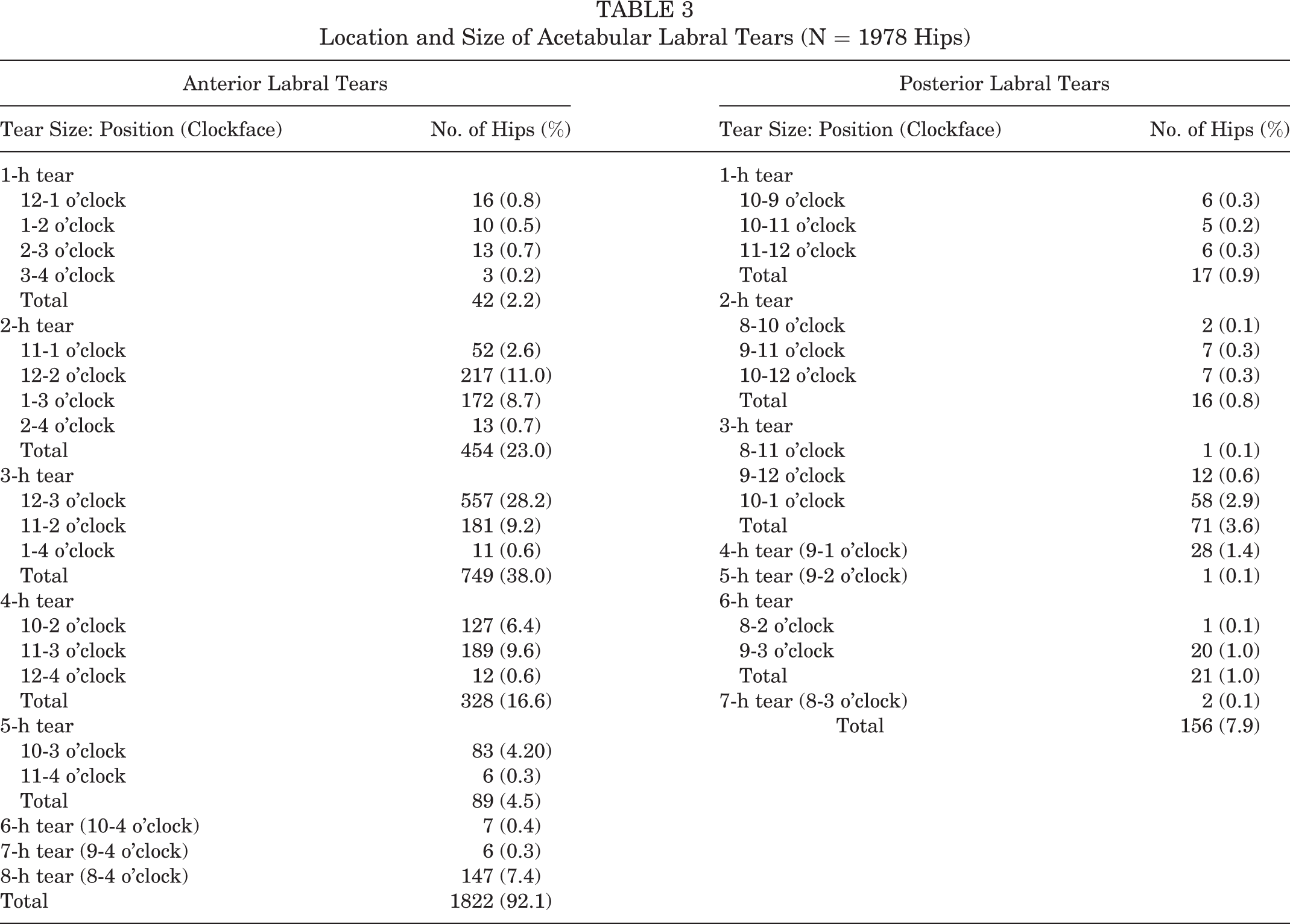
A total of 1978 hips (1201 female and 777 male) were included in this study; the mean ± SD patient age was 33.7 ± 12.7 years, and the mean body mass index was 25.5 ± 4.7. The circumferential size of the observed labral tears during arthroscopic intervention ranged between 1 and 8 clockface hours and is presented in Table 2. Of these hips, there were 1822 (92.1%) classified as anterior labral tears and 156 (7.9%) as posterior labral tears by the treating orthopaedic surgeon. Data regarding the location and size of labral tears for all included hips are presented in Tables 3 and 4.
Size of Labral Tear by Clockface Hours
Location and Size of Acetabular Labral Tears (N = 1978 Hips)
Size of Labral Pathology (Clockface Hours Spanned) for Patients With Labral Repair

Size and Location of Labral Repairs
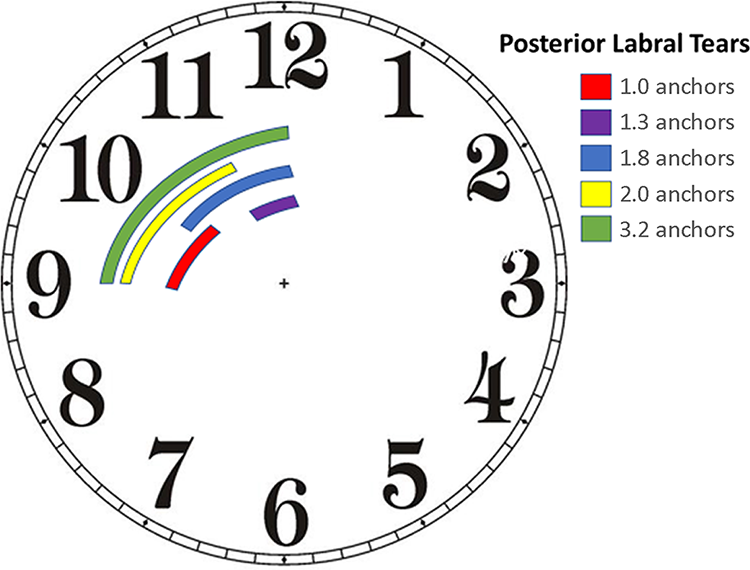
Acetabular labral tears in 1645 hips (83.0%) underwent repair. The circumferential size of the most prevalent labral tears (in the number of hours spanned) is presented in Table 4. The most common size was 3 hours, accounting for 774 patients (47.0%) who underwent labral repair. Of the 1645 anterior labral tears present in this study, 1523 (92.6%) were repaired, with the most prevalent locations represented in Figure 1. Of the 156 posterior labral tears, 122 (78.0%) were repaired, with the most prevalent locations presented in Figure 2.
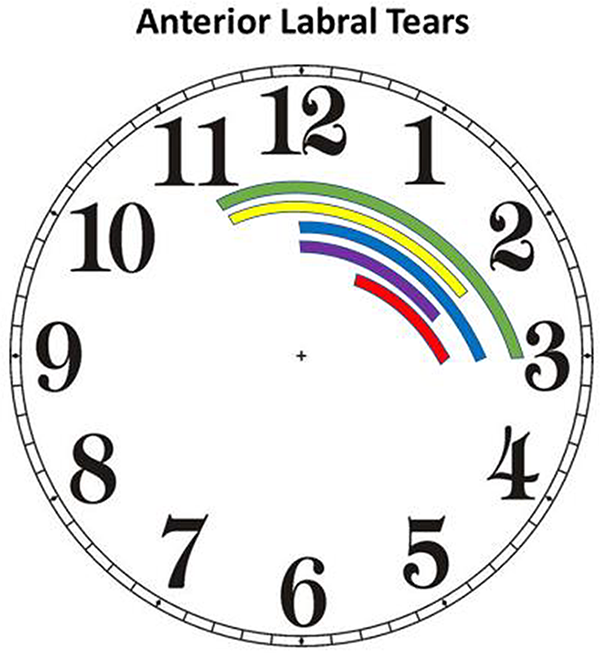
The most prevalent anterior labral tears. The colored bars indicate the most common locations for the tears as seen intraoperatively and described using the clockface method.

The most prevalent posterior labral tears. The colored bars indicate the most common locations for the tears as seen intraoperatively and described using the clockface method.
As shown in Table 5, the primary location of tears, as seen in 537 hips (32.6%), was in the anterior position between 12 and 3 o’clock. The most common repairs to the anterior and superior labrum were in tears located between 12 and 2 o’clock (n = 200; 12.2%), 11 and 3 o’clock (n = 175; 10.6%), 11 and 2 o’clock (n = 164; 10.0%), and 1 and 3 o’clock (n = 163; 9.9%). The most common location of posterior labral tears occurred between 10 and 1 o’clock and accounted for 51 (41.8%) posterior tears that were repaired.
Location, Size, and Number of Anchors for Acetabular Labral Repairs (n = 1645) a

a Dashes indicate none reported.
Anchor Density per Tear Size
The mean labral repair required a mean 2.7 ± 0.9 anchors across all surgical centers, with 2.8 ± 0.7 and 2.4 ± 0.7 anchors used to repair anterior and posterior labral tears, respectively, as shown in Table 5. Figures 3 and 4 describe the numbers of anchors used for anterior and posterior labral tears of varying sizes.

Allocation of anchors used for anterior labral tears of varying sizes.
Allocation of anchors used for posterior labral tears of varying sizes.
There was variance in the usage of anchors according to the size of the tear and the specific surgeon, as shown in Table 6. For 1-hour tears, the surgeons used a mean of 1 to 1.6 anchors, F(5, 36) = 5.72; P = .001. For tears spanning 2 hours, surgeons averaged 1.7 to 2.4 anchors per repair, F(7, 423) = 4.84; P < .001. The tears that spanned 3 hours averaged 2.1 to 3.2 anchors per repair, F(7, 767) = 36.86; P < .001, and tears that spanned 4 hours averaged 2.2 to 4.1 anchors per repair, F(7, 299) = 35.93; P < .001.
Surgeon Allocation of Anchors According to Labral Tear Size a

a Tear size was classified according to clockface hours. Dashes indicate none reported.
Anchor Types
In total, 1636 hips (99.5%) underwent labral repair surgery that had the type of anchor used for fixation recorded within the database. The most common type of anchor across all surgeons was a PEEK (polyether ether ketone) anchor, accounting for 76.0% of cases (1239/1636). An all-suture fixation was performed in 22.0% (356/1636) of hips, with about 3.0% (42/1636) receiving biocomposite anchors. Of the 7 participating surgeons, 6 predominately used PEEK anchors for labral refixation. There was a significant effect for the points of fixation per labral tear across all surgeons, F(2, 1633) = 95.73; P < .001. Repairs with PEEK anchors averaged 2.6 ± 0.82 anchors per repair versus 3.3 ± 0.94 sutures per repair for the all-suture technique.
Discussion
The current study was successful in stratifying a large multicenter cohort of patients undergoing arthroscopic treatment for acetabular labral tears based on size, location, and number of anchors utilized during labral repair. We were able to establish a range of anchor density per acetabular region, as utilized by 7 high-volume hip arthroscopic specialists. The repairs were recorded in areas of the acetabulum known to be most involved with labral damage. The results showed that most labral repairs were performed for labral damage between the clockface hours of 9 and 3 o’clock, with the highest percentage between 12 and 3 o’clock. This zone of damage is consistent with published evidence concerning typical intra-articular zones of damage found in patients with 3 and without 10,24 femoroacetabular impingement. Factors that may affect the number of suture anchors used in the clinical setting include technical limitations of labral and bone stock available for anchor placement, suture anchor size and design variations, and cost of implants.
The current study adds to the practical and scientific body of knowledge by reporting on the way that independent expert surgeons select the number of suture anchors during acetabular labral repair. Despite an increase in the application of acetabular labral repair techniques, no peer-reviewed evidence exists concerning the appropriate selection of number of anchors used in the clinical setting. The clinical rationale for labral repair did not specify an appropriate number of anchors across varying tear sizes. 12 The histology of labral healing after repair in a sheep model using a single anchor for an experimentally created zone of injury of 1.5 cm showed healing. 21 Placement of additional suture anchors has been shown to increase the likelihood of penetrating the articular acetabulum as well as the psoas canal. 17,7 In a load-to-failure study, Koh and Gupta 13 reported on a 2-anchor labral repair construct under simulated weightbearing in a cadaveric model without convincing rationale for the number of anchors selected. Clinical evidence for multianchor repair is also sparse. Early clinical series demonstrated superiority of labral repair versus debridement for treatment of acetabular labral tears during arthroscopic surgery, without supplying evidence for the exact number of suture anchors used in the repair group. 15 More recently, Menge et al 19 reported improvements in the labral repair and debridement groups during arthroscopic femoroacetabular impingement surgery with minimal 10-year follow-up; again, no data were presented concerning the number of anchors used for the repair group. In a recent review, Domb et al 8 presented an evidence-based, decision-making algorithm for treatment of labral injury but did not comment on the number of anchors required for repair. Likewise, studies that rely on large governmental or insurance payer data repositories lack information concerning the manner of repair. 6 Therefore, expert opinion (level 5 evidence) is the sole determinant of the number of suture anchors used during acetabular labral repair. The current study does not answer what the appropriate number of anchors should be for each labral repair but rather reports the mean number used for tear size by high-volume hip arthroscopic specialists.
The range of mean suture anchors (1-4.1) deployed by investigators in this study followed logical patterns of deployment. For larger segments of labral damage, more anchors were used. The decision to use >1 anchor is a clinically relevant one for cost and technical reasons. While variations in the number of anchors existed across all acetabular arcs, when ≥2 hours of distance on the clockface (eg, 1 to 3 o’clock) were damaged, all investigators selected at least 2 suture anchors. Anchors used by investigators in this study varied in diameter, length, and knotless or standard design, with no correlational analysis conducted in the current study to account for these variations. Centers in which investigators used smaller or all-suture anchors trended toward a higher number of anchors per repair, while those with larger anchor diameters trended toward fewer. Despite the lack of current evidence mandating multianchor repair, single-anchor labral repairs were performed in the minority of the patients in this cohort (2.9%). The data presented here do not provide an explanation for this trend, although reasoning may suggest that investigators selected the best construct for achieving healing of labral tissue to bone.
Ideally, surgeons would rely on higher levels of evidence concerning the appropriate number of suture anchors for use in specific clinical settings, but barriers exist. Construction and execution of applicable basic biomechanical studies require better understanding of the true biomechanical environment and in vivo milieu of a human hip labral repair site than what currently exists. In addition, the practical limitations of surgical care preclude the use of a prospective randomized clinical trial without first establishing a safe number of anchors for use in assigning groups. A cohort cross-sectional study of patients contemporaneously treated with arthroscopic labral repair by multiple high-volume surgeons allows for accurate description of real-world decision making.
The strengths of the current study include the careful selection of high-volume surgeons to include in the study, the a priori consensus on data recording, and the lack of bias in choice of suture anchor number, type, or location. This design allowed each investigator to treat patients according to the best practice standards within one’s practice without incentive for using greater or fewer numbers of suture anchors. To our knowledge, this study allows the first description of real-world implant selection patterns of high-volume hip arthroscopic surgeons. Additional follow-up of these patients and their clinical outcomes could help describe the appropriate number of anchors.
Several limitations must be considered when interpreting the results of the current study. Clinical objections to the cross-sectional study design include the lack of clinical follow-up, lack of radiographic or histologic evidence of healing, and lack of verification of anchor integrity, suture passage pattern, or method of labral takedown and preparation. Additionally, no a priori intra- or interrater analysis was performed for the clockface classification method used by each orthopaedic surgeon involved in the current study. Given these important deficiencies, data from this study should not be used to establish standard of care in anchor selection for future cases. The lack of interrater reliability of the clockface classification as well as the lack of validated arthroscopic distance measures for zones of labral injury are also limitations. By not reporting outcome data, the current study prevents drawing any meaningful conclusions to the appropriate number of anchors during labral repair. Given the absence of superior studies available that might address these design and implementation limits, the current study provides clinicians with previously unavailable information concerning the practice patterns of experts in the field.
Conclusion
The current study was successful in assessing a large multicenter cohort of patients undergoing arthroscopic treatment for acetabular labral tears based on size, location, and number of anchors utilized during labral repair. The results of this study establish a range of acceptable anchor density per acetabular region. The results show that most labral repairs were performed for labral damage between the clockface hours of 9 and 3 o’clock, with the highest percentage between 12 and 3 o’clock. For tears of 1 clockface hour, orthopaedic surgeons averaged 1 to 1.6 anchors per repair; 2-hour tears, 1.7 to 2.4 anchors; and 3-hour tears (the most common), 2.11 to 3.21 anchors. For tears spanning 4 clockface hours, surgeons averaged between 2.2 and 4.1 anchors per repair.
Footnotes
Final revision submitted August 11, 2020; accepted August 27, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.J.C. has received faculty/speaking fees and royalties from Arthrex and Breg. S.J.N. has received consulting fees from Ossur and Stryker (paid to institution) and royalties from Stryker. A.B.W. has received education payments and consulting fees from Allosource and Stryker. J.P.S. has received education payments from Liberty Surgical, consulting fees from Stryker, and hospitality payments from Arthrosurface and Arthrex. D.M. has received consulting fees from Zimmer Biomet and royalties from Arthrocare and Smith & Nephew. T.J.E. has received education payments from Arthrex and Medacta and consulting fees and honoraria from Medacta. A.J.S. has received education payments from Arthrex, educational consulting fees from Smith & Nephew, and royalties from Thieme; has stock/stock options in Johnson & Johnson; and holds patents US12398960 and US14457743. D.S.C. has received research grants from Arthrex and consulting fees, speaking fees, and royalties from ConMed Linvatec and Zimmer Biomet. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Allegheny Health Network (study No. 2017-130-WPH).