
Abstract
Background:
Radiographic findings related to the cam and pincer variants of femoroacetabular impingement (FAI) include measurements of the alpha angle and lateral center-edge angle (LCEA). The function of these radiographic findings has been put into question because of high heterogeneity in reported studies.
Purpose:
The aim of this study was 3-fold: (1) to determine the prevalence of cam and pincer variants according to sex and age on anteroposterior (AP) pelvic radiographs from an asymptomatic nonathletic population, (2) to identify the most common radiographic signs of cam- and pincer-type variants, and (3) to determine if there are variations in the prevalence of these radiographic signs according to sex and age.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
There were 3 independent observers who retrospectively analyzed the 939 AP pelvic radiographs (1878 hips) of patients aged 18 to 50 years who did not have hip symptoms and who were not professional athletes. The prevalence of the cam and pincer variants according to the alpha angle and LCEA, respectively, and the presence of other radiographic signs commonly associated with these variables were determined in the overall population and by subgroup according to sex and age group (18-30, 31-40, and 41-50 years). Descriptive and inferential statistics were used to analyze the study sample.
Results:
The mean age of the included population was 31.0 ± 9.2 years, and 68.2% were male. The prevalence of the cam-type variant was 29.7% (558/1878), and that of the pincer-type variant was 24.3% (456/1878). The radiographic signs that were most associated with the cam and pincer variants were a pistol-grip deformity and the crossover sign, respectively. Significant differences (P < .001) in the prevalence of these variants were identified between men and women in both variants. No differences were observed in the alpha angle or LCEA according to sex or age.
Conclusion:
Radiographic findings suggestive of FAI had significant variations with respect to sex and age in this study sample. This study provides information to determine the prevalence of these anatomic variants in the general population.
Femoroacetabular impingement (FAI) is a clinical syndrome defined by pain and functional limitations of the hip in young adults and middle-aged populations and may contribute to the development of early hip osteoarthritis. 13 The anatomic characteristics associated with the development of this condition include loss of the cervicocephalic offset or asphericity of the femoral head (cam-type variant), focal or global acetabular overcoverage (pincer-type variant), and mixed characteristics (cam and pincer types), 3 with the latter having the highest prevalence in patients with FAI 39 ; however, it has not been established whether the same prevalence occurs in the general population. Over time, multiple imaging methods (eg, plain radiography, computed tomography [CT], magnetic resonance imaging [MRI], computed tomography arthrography, and magnetic resonance arthrography) have been used to determine the prevalence and morphological characteristics of these anatomic variants because a 2-dimensional static assessment of a 3-dimensional dynamic deformity can be imprecise. 52 Even so, plain radiography of the pelvis in its different projections has been the most widely used imaging method for the radiographic detection of these anatomic variations in studies with large samples. 59
The radiographic findings associated with FAI observed on plain film radiographs include the following for the cam-type variant: an increased alpha angle, a pistol-grip deformity (PGD) of the femoral head-neck, a low femoral head–to–femoral neck ratio (FHFNR), lateral flattening of the femoral head (LFFH; coxa recta), focal prominence of the femoral neck (FPFN), and coxa vara defined by the femoral neck-shaft angle (NSA; also called the caput-collum-diaphyseal angle). For the pincer-type variant, the findings include the following: an increased lateral center-edge angle (LCEA; Wiberg angle); a decreased acetabular index (AI; Tönnis angle); the crossover sign (COS; figure-of-8 sign); the posterior wall sign (PWS); excessive acetabular coverage (EAC) and its variant, os acetabuli; the ischial spine sign; coxa profunda; and protrusio acetabuli. 6,23,46
The utility of these radiographic signs has been put into question owing to the low reliability as well as the discrepancy between the results of radiography and those obtained by advanced imaging methods and intraoperative findings. 7,56 However, other studies support their use and highlight the good agreement with advanced imaging methods. 51,57
Although these morphological features may cause pain and dysfunction in some hips, many hips remain asymptomatic despite radiographic evidence of FAI-related features. 45 This has led clinicians to question the prevalence of FAI-related morphological features in asymptomatic patients. Few studies have determined whether there are differences in the prevalence of radiographic signs for FAI associated with sex and age. 26,28,55 After searching the available scientific literature, we did not find a study that determined the prevalence of these variants or the radiographic signs most commonly associated with them in the general population, in a population of the same ethnic group with a subgroup analysis regarding sex and age, or in asymptomatic patients who were not professional athletes. We hypothesized that there are significant differences regarding sex and age in the prevalence of cam and pincer variants as well as in their main associated radiographic signs in asymptomatic patients who were not professional athletes. Therefore, this study was intended to encompass 3 main issues: (1) to determine the prevalence according to sex and age of cam and pincer variants in a large sample of anteroposterior (AP) pelvic radiographs from an asymptomatic population, (2) to identify the most common radiographic findings in patients with cam- and pincer-type variants, and (3) to determine if there are variations in the prevalence of these radiographic signs in terms of sex and age.
Methods
This was a retrospective cross-sectional and descriptive study that adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. The study received ethics committee approval and was conducted in accordance with the World Medical Association’s 1964 Declaration of Helsinki and its revision in 2013. All of the images were obtained for other (medical) reasons and not for conducting the present study; therefore, informed consent was not obtained. All sensitive information was concealed to protect patient confidentiality.
Eligible for the study were 1154 AP pelvic radiographs from August 2017 to January 2020 of Mexican patients aged between 18 and 50 years. The medical indication for these radiographs was an evaluation of traumatic injuries. The study exclusion criteria were radiographs of suboptimal technical quality (ie, excessive pelvic or femoral rotation assessed by an obturator foramen index outside the range of 0.6-1.8, the greater trochanter was not in profile, or the lesser trochanter did not project onto the inner edge of the femur), poor positioning, tilting, and motion as well as the presence of bone abnormalities (which were ruled out by a musculoskeletal radiology specialist [G.E.-R.] who did not participate in the subsequent assessment or observation of radiographs).
Other exclusion criteria were hip, acetabular, or pelvic fractures; diseases that affected the proximal femur (tumors, infections, malformations, avascular necrosis of the hip, developmental dysplasia of the hip, malunion of a femoral neck fracture, hip osteoarthritis of grade 3 or 4 according to the Kellgren-Lawrence scale 20 ); presence of an orthopaedic implant (total or partial prostheses, plates, screws, intramedullary nails, K-wires, etc); patients who underwent pelvic osteotomy or extraction of an iliac crest autograft; a history of rheumatoid arthritis, juvenile idiopathic arthritis, congenital hip dysplasia, Legg-Calve-Perthes disease, slipped capital femoral epiphysis, trochanteric bursitis, septic arthritis of the hip, lumbar discopathy, sacroiliitis, long-term steroid use, chemotherapy or radiation, nonambulatory status, neuromuscular disorders, or hip dislocations; a history of hip, femoral, acetabular, or pelvic fractures or surgery; the presence of pain or functional limitations in one or both hips during an interview or physical examination (especially during flexion, adduction, or internal rotation); and those who reported being or having been high-performance athletes or who reported the trauma as occurring during a professional sports practice or competition. Patients who played sports recreationally were not excluded. Last, patients with an incomplete medical record were eliminated from the study.
Of the original 1154 radiographs, 215 (18.6%) were excluded from the study (Figure 1), resulting in 939 radiographs (1878 hips) for our analysis. A flow diagram of the study is presented in Figure 1.

Flow diagram of the study.
Orthopaedic radiology technicians with more than 15 years of experience were responsible for obtaining the images. A Proteus XR-a radiographic system (GE Healthcare) was used to obtain radiographs using the following technique: the patient was placed in a supine position with the hip extended and internally rotated 15°; the crosshairs of the beam were centered on the midway point between the superior border of the pubic symphysis and a line drawn connecting the anterior superior iliac spine. The following parameters were used to acquire the images: 65-80 kV, 65-80 mA, a thick focus, and a bucky. The focus-plate distance was 102 to 110 cm with a 35 × 43–cm cassette placed cross-sectionally and the tube perpendicular to the table. Advantage Workstation AW Volume Share 2 software (GE Healthcare) was used to assess the radiographs. The quality of the radiographs was considered adequate when the tips of the coccyx and pubic symphysis were in line and the distance between them was between 1 and 3 cm as well as when both teardrops, the iliac wing, and the obturator foramen were symmetric. This technique represents the method standardized by the emergency radiology service of our institution for the acquisition of an AP radiograph of the pelvis.
We performed 11 measurements: 6 measurements per observation (3 quantitative and 3 qualitative) catalogued as cam-type variants and another 5 measurements per observation (2 quantitative and 3 qualitative) for pincer-type variants. Patient identification details were removed from all radiographs to maintain confidentiality. Measurements were carried out by 3 observers independently (R.M.-A., A.T.-N., F.V.-C.). The observers were blinded to the age and medical history of the patients to whom the radiographs belonged as well as to the results of the other observers. Before performing the measurements, each observer was trained for 2 weeks on a previously established measurement protocol for each of the chosen parameters by the same musculoskeletal radiologist who applied the selection criteria of the study (G.E.-R.); a set of 20 radiographs was used to teach the observers how the measurements had to be performed (these patients were not part of the study population), and several face-to-face meetings were held to review them and refine the standardized definitions.
To evaluate intraobserver reliability, the raters were asked to repeat the measurements and radiographic observations 1 month after the first measurement; these were presented to the raters in a different order than on the first occasion. Finally, the 3 observers reviewed the differences at a consensus meeting using a nominal group technique in which the hierarchical position of the observers was the same.
Measurements and Determination of Cam-Type Variants
The alpha angle was measured with the use of a previously reported method by Nötzli et al. 35 Although designed for use on CT or MRI, it is also a reliable and valid method for plain radiography. 5 An alpha angle of <55° was considered normal, and an alpha angle of ≥55° was considered a cam-type variant (Figure 2A). 11
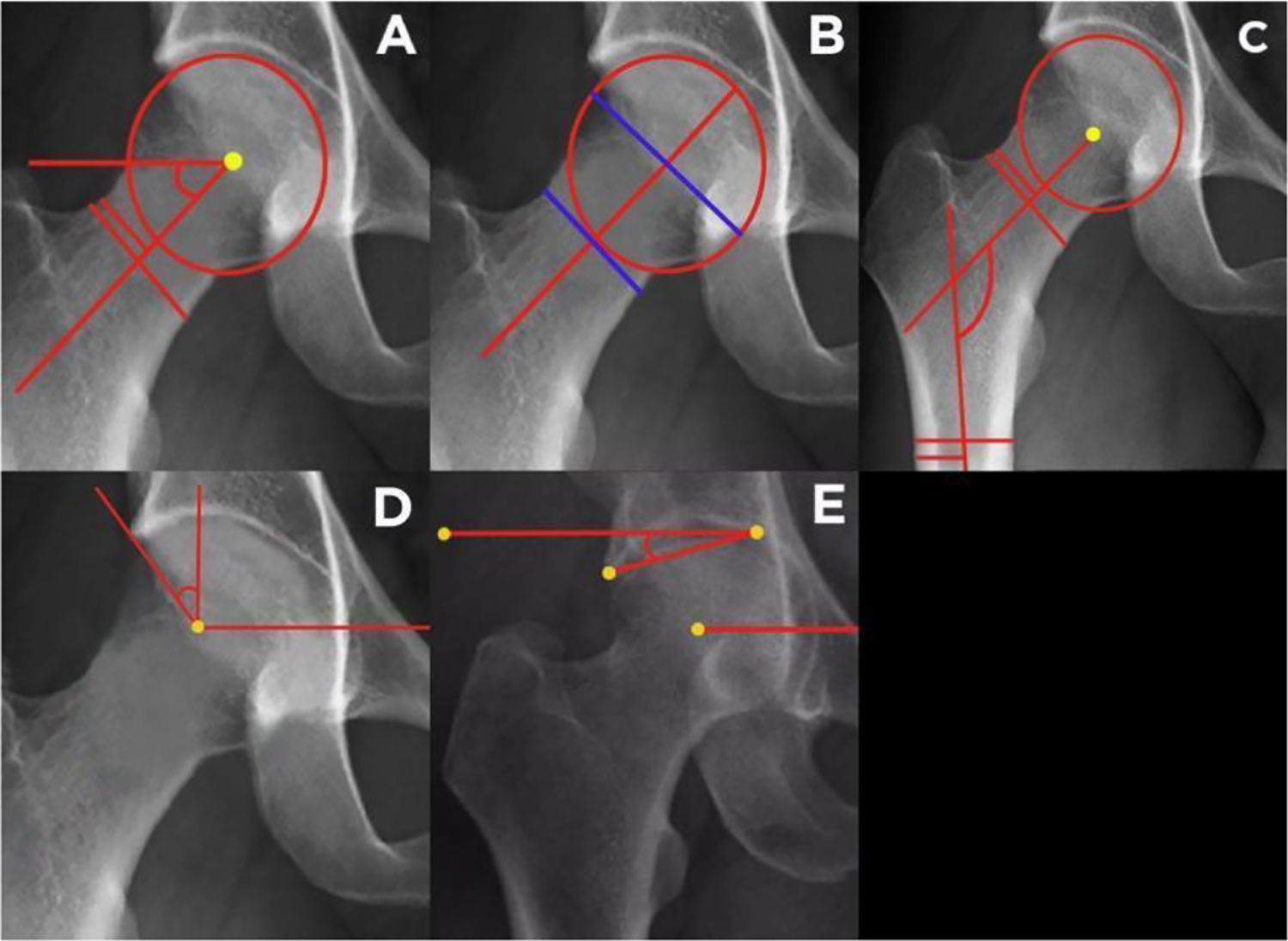
Methodology followed for the measurement of the angles and indexes used in the present study: (A) alpha angle, (B) femoral head–to–femoral neck ratio, (C) femoral neck-shaft angle, (D) lateral center-edge angle, and (E) acetabular index.
A PGD included the objective measurement of a low FHFNR and the subjective pistol-grip appearance. PGD was defined as a characterized loss of normal concavity morphology of the anterosuperior region of the head-neck junction, resulting in a nonspherical head that could be seen as an extended convex margin lateral to the epiphyseal scar (Figure 3A). Doherty et al 10 determined that PGD is associated with a low FHFNR and that the ratio of the maximal femoral head diameter divided by the minimal parallel femoral neck diameter differentiated hips with the deformity from those without it. A line was drawn through the femoral head center and a point in the middle of the femoral neck. Perpendicular to this line, another line was drawn at the maximum femoral head diameter, and another line was drawn at the minimum femoral neck diameter (Figure 2B). The ratio was the head diameter divided by the neck diameter. A ratio of ≤1.27 was considered abnormal. 6 Other suggestive signs of the cam variant are FPFN (defined as an exostosis in the femoral neck) 12 (Figure 3B) and LFFH (flattening along the femoral head-neck junction and, in severe cases, loss of differentiation between them) 23 (Figure 3C), both of which were determined by the presence of the deformity on radiographs by direct observation; however, it has been recognized that these are not present in all cases of cam-type variants. 23 The reviewers considered these signs to be either positive or negative, and disagreements were resolved by a consensus. Moreover, coxa vara was defined by the NSA (Figure 2C). An NSA of <125° was considered as coxa vara, which is recognized as a cause of FAI. 10

Radiographic signs analyzed in the present study for (A-C) cam- and (D-F) pincer-type variants: (A) pistol-grip deformity (left side), (B) focal prominence of the femoral head (both sides), (C) lateral flattening of the femoral head (both sides), (D) excessive acetabular coverage (right side) and os acetabuli (left side), (E) crossover sign (both sides), and (F) posterior wall sign (right side). In some images, mixed variants or some other radiographic signs of the same variant can be observed in the contralateral hip; however, they are not mentioned here because the purpose was only to highlight a specific deformity in each image.
Measurements and Determination of Pincer-Type Variants
A pincer variant was defined as any hip that had an LCEA of ≥40° (Figure 2D). This angle measures the lateral coverage of the acetabular roof with regard to the femoral head and has been shown to be a good predictor of the presence of a deformity, with a good intraobserver correlation index; in addition, it is the radiological parameter most used in previous studies to determine pincer-type variants. 46 An AI of <0° was considered to be consistent with acetabular overcoverage (Figure 2E). 42 The COS was positive when the anterior wall of the acetabulum crossed the posterior border of the acetabulum medial to the lateral rim of the weightbearing area (Figure 3E). 23 The presence of the PWS was also determined and considered positive when the posterior wall lay medial to the center of the femoral head (Figure 3F). 23 EAC was defined as the extension of the lateral acetabular rim in the inferior and/or lateral direction (Figure 3D, right hip) 23 or an unattached bone fragment lateral to the superolateral acetabular rim (Figure 3D, left hip). 6 The reviewers considered these signs to be either positive or negative. Definitions were obtained from the literature.
We considered the presence of a radiographic cam-type variant when there was an abnormal value of the alpha angle and an abnormal value of the LCEA for the pincer-type variant. If the observer identified a mixed deformity (alpha angle >55° and LCEA >40°), the observer was asked to report the radiographic findings present in the cam and pincer variants as independent signs (registering the combination of signs), which were classified as a mixed variant (without specifying the predominance of one type over the other or the equitable contribution).
Sample Size Calculation
To calculate the sample size, we used a formula to estimate a mean value (that of the alpha value) within an infinite population. A Z value of 1.96, a sigma (SD) of 5, and a delta (magnitude of error) of 0.5 were used in the calculation, which resulted in 384 participants. However, to have sufficient power to determine the prevalence according to sex (male and female) and age (18-30, 31-40, and 41-50 years), this division was based on the patterns of degenerative changes in the hip with age. We decided to increase the sample size to at least 1000.
Statistical Analysis
The average of the measurements made by the 3 observers was considered the final result, as no statistically significant differences were found between the results of the 3 observers. Quantitative variables are described as means and standard deviations. The Student t test and analysis of variance were used to compare quantitative variables. Qualitative variables are described as frequencies and percentages. The chi-square test was used to compare qualitative variables; to measure their strength of association, odds ratios (ORs) and 95% CIs were calculated. Intrarater and interrater reliability were calculated for qualitative observations using the Cohen and the Fleiss kappa coefficients, respectively. For quantitative observations, intrarater and interrater reliability were calculated using the intraclass correlation coefficient (ICC) between all pairs. The interpretation of concordance values was adapted as follows: κ <0.20, poor agreement; 0.21-0.40, fair agreement; 0.41-0.60, moderate agreement; 0.61-0.80, good agreement; and 0.81-1.00, very good agreement. Similarly, an ICC of ≥0.80 was considered good agreement. A significance level of .05 was decided a priori. Statistical analyses were performed using SPSS software Version 19.0 for Mac (IBM).
Results
Of the 939 radiographs (1878 hips) included in our analysis, 640 (1280 hips; 68.2%) of the radiographs were of men. The mean age of the participants was 31.0 ± 9.2 years. The distribution of the sample based on sex and age, as well as the mean age of each of these age groups, is shown in Table 1.
Sex and Age of the Hips
a Mean ± SD for that age group.
No significant differences were found when the mean values obtained from each of the observers were compared. Similarly, the results of the intraobserver and interobserver analyses resulted in good agreement (κ > 0.80 and ICC > 0.80) for all sets.
Cam-Type Variant
The mean alpha angle for the total population was 50.6° ± 5.2° (N = 1878). Based on measurement of the alpha angle, the overall prevalence of the cam-type variant was 29.7% (558/1878). The mean alpha angle in hips with versus without the cam variant was 63.8° ± 4.2° (n = 558) versus 43.2° ± 5.0° (n = 1320), respectively (P < .001). The mean alpha angle of the hips with the cam variant was not significantly different between men (64.1° ± 1.6°) and women (62.7° ± 4.1°).
In the 558 hips with the cam-type variant, the mean alpha angle according to age group and sex are shown in Table 2. There were no differences in the alpha angle when comparing men versus women for any age group as well as when comparing the different ages within the same sex.
Alpha Angle of the Cam Variant (n = 558) a
a Data are reported as mean ± SD in degrees.
Notably, the cam variant was present in 114 of 598 hips (19.1%) in women and 444 of 1280 hips (34.7%) in men (OR, 2.25 [95% CI, 1.78-2.85]; P < .001). The prevalence of this variant in the different age groups is shown in Table 3. Differences were found when comparing the prevalence of the cam-type variant between men and women; the cam variant was strongly associated with male sex for the 18- to 30-year (OR, 3.18 [95% CI, 2.01-5.02]; P < .001), 31- to 40-year (OR, 2.22 [95% CI, 1.47-3.34]; P < .001), and 41- to 50-year age groups (OR, 1.66 [95% CI, 1.12-2.46]; P = .01). The prevalence of the cam-type variant was also significant between the different age groups for women (P = .03) but not for men (P = .05).
Prevalence of the Cam Variant (N = 1878) a

a Data are reported as n (%). Bolded P values indicate statistically significant differences between the groups (P < .05).
The cam variant was found in 27.7% (260/939) and 31.7% (298/939) of the right and left femurs, respectively. None of the comparisons resulted in differences between the right and left femurs. We noted a bilateral presence of the deformity in 87 patients (174/558 hips), representing 31.2% of the total. Overall, the most prevalent sign was a PGD of the femoral head-neck (494/1878; 26.3%) when considering the objective and subjective measurements. In hips with the cam variant, PGD represented a prevalence of 88.5% (494/558). The second most prevalent sign was LFFH, which occurred in 11.3% (212/1878) of the general population and in 38.0% (212/558) of the population with the cam variant. Finally, FPFN was present in 3.5% (66/1878) of the general population and in 11.8% (66/558) of the population with the cam variant. Table 4 shows the distribution of these radiographic signs according to sex and age.
Prevalence of Radiographic Signs Associated With the Presence of the Cam Variant (n = 558) a

a Data are reported as n (%). Bolded P values indicate significant differences between the groups (P < .05). FPFN, focal prominence of the femoral neck; LFFH, lateral flattening of the femoral head; PGD, pistol-grip deformity.
There were significant differences in the prevalence of coxa vara when comparing men versus women (with men having a higher incidence) for any age group, as well as an increasing prevalence with older age regardless of sex. The variations in the prevalence of coxa vara according to sex and age are shown in Table 4.
Pincer-Type Variant
The mean LCEA for the total population was 36.4° ± 3.1° (N = 1878). In hips without the pincer variant (n = 1422; 75.7%), the LCEA was 29.4° ± 3.9°, and it was 49.6° ± 3.2° in hips with the pincer variant (n = 456; 24.3%). No significant differences were found when comparing men (51.2° ± 2.8°) versus women (46.7° ± 3.6°).
In the 456 hips with the pincer-type variant, the mean LCEA according to age group and sex are shown in Table 5. There were no differences in the LCEA when comparing men versus women for any age group or when comparing the LCEA of the different age groups for the same sex. As seen in hips with the cam variant, a greater prevalence of the pincer variant was observed in men (357/1280; 27.9%) than in women (99/598; 16.6%) (P < .0001).
LCEA of the Pincer Variant (n = 456) a

a Data are reported as mean ± SD in degrees. LCEA, lateral center-edge angle.
The distribution of the pincer variant according to sex and age group is shown in Table 6. The prevalence of the pincer-type variant was strongly associated with male sex in the 18- to 30-year (OR, 2.36 [95% CI, 1.40-3.97]; P < .001), 31- to 40-year (OR, 1.90 [95% CI, 1.23-2.94]; P < .01), and 41- to 50-year age groups (OR, 2.28 [95% CI, 1.54-3.38]; P < .001). Similarly, differences were found when comparing the prevalence of the pincer-type variant between the age groups within the same sex (P = .0003 for men; P < .05 for women).
Prevalence of the Pincer Variant (N = 1878) a

a Data are reported as n (%). Bolded P values indicate significant differences between the groups (P < .05).
The pincer variant was found in the right acetabulum in 22.9% (215/939) of the hips and in the left acetabulum in 25.7% (241/939) of the hips. We found no differences between the right and left acetabula. This variant was found bilaterally in 73 patients (146/456 hips), representing 32.0% of the total, and unilaterally in the remaining 68.0% (310/456) of hips. Table 7 shows the prevalence of the radiographic signs that predict the pincer variant. The most prevalent sign in the total population was the COS (320/1878; 17.0%), with 70.2% (320/456) in the pincer variant population, followed by the PWS in 8.5% (160/1878) of the total population and 35.1% (160/456) of the pincer variant population. EAC was found in 4.8% (91/1878) of the total population and 20.0% (91/456) of the pincer variant population. Notably, the COS was strongly associated with male sex in the 18- to 30-year age group (OR, 4.99 [95% CI, 1.75-14.18]; P = .001).
The mean AI for the total population was 3.29° ± 5.12° (N = 1878). Further, the mean value was 5.12° ± 2.67° for hips with a positive AI (n = 1502; 83.1%) and –3.40° ± 1.96° for those with a negative AI (n = 306; 16.9%) (P = .002). The mean AI of the hips with a negative AI was –4.98° ± 2.24° for men (256/1280; 20.0%) and –2.01° ± 1.03° for women (50/598; 8.4%) (P = .01). There were differences in the AI when comparing men versus women in the 31-40 and 41-50 year age groups (P < .05), but there were none when comparing the AI in different age groups within the same sex. Variations in the prevalence of a negative AI according to sex and age are shown in Table 7.
Prevalence of Radiographic Signs Associated With the Presence of the Pincer Variant (n = 456) a

a Data are reported as n (%). Bolded P values indicate significant differences between the groups (P < .05). AI, acetabular index; COS, crossover sign; EAC, excessive acetabular coverage; PWS, posterior wall sign.
Mixed Variant
In 390 (69.9%) of the hips, we found a mixed deformity; in 168 hips (17.9%), there was a unique cam-type variant, and in 66 hips (12.2%), there was a unique pincer-type variant. The most frequent combination of radiographic signs was PGD + COS in 217 hips (55.6%).
Discussion
We found significant differences regarding both cam- and pincer-type variations and their main radiographic signs when comparing by age and sex in hips from an asymptomatic and nonathletic population. Different systematic reviews have reported a highly variable prevalence (range, 5%-75%) of these variants. 8,11 A possible explanation for this high variability is the presence of heterogeneity among the baseline characteristics included in their analyses. This heterogeneity includes but may not be limited to ethnicity, sex, age, presence of symptoms, history of disease, physical activity, imaging methods, and the operational definition of each included variable. To be able to provide more accurate estimates, studies must decrease the degree of heterogeneity in the included population and/or perform subgroup analyses, considering important covariates such as symptoms or physical activity.
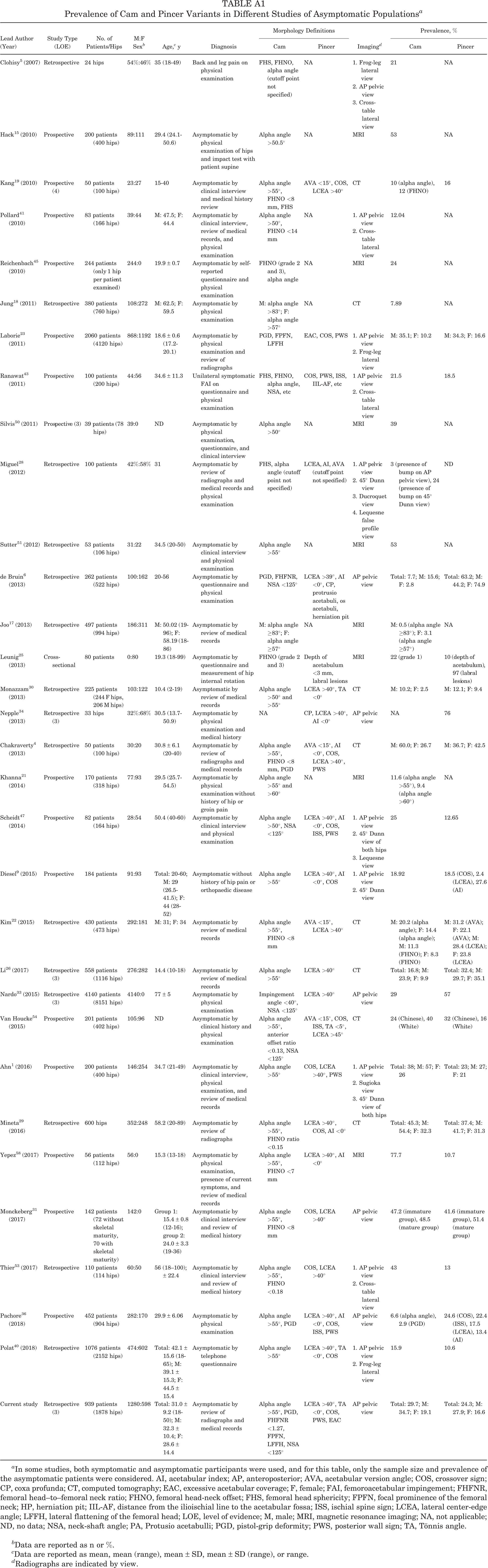
A previous systematic review reported that cam- and mixed-type variants were more prevalent among athletic, symptomatic, and male participants than among nonathletic, asymptomatic, and female participants. 27 Similarly, several studies and reviews have reported the presence of radiographic signs suggestive of FAI in selected cohorts of asymptomatic patients. 11 However, about half of the studies had small samples, without subgroup analysis by sex or age, and with highly heterogeneous selection criteria. In Appendix Table A1, we share a comparison of the characteristics of the studies evaluating asymptomatic participants.
Cam-Type Variant
In a systematic review published in 2015, the prevalence of cam-type FAI in asymptomatic participants was reported as 23.1%. 11 Another systematic review evaluating asymptomatic participants reported a prevalence of 22.4%, 27 and 2 other studies reported a prevalence between 27% and 29%. 33,45 Their results are very similar to ours (29.7%). Regarding sex and age, our study supports previous findings of a greater prevalence in male patients. 18,25,41 Differences in the prevalence of the cam-type variant within age groups have not been widely studied. Some findings in adolescent and young adult cohorts have demonstrated increasing prevalence with older age until full skeletal development. 20,37,44,48,49 However, the majority of the participants in these studies maintained constant physical activity. In another study in an elderly population, the prevalence was reported to be 5%, however those authors could have had a different definition of the variant than the one used in the present study. 33 Mineta et al 29 reported a significant increase in alpha angle values and the prevalence of the cam variant as age increased in a cohort of Japanese patients. Considering they used 40 years as the cutoff age (to decide whether a patient belonged to the young group or the old group), combined the values of men and women, and had a sample consisting of mostly elderly patients, their results are difficult to compare with ours. 29
Our study represents the largest one comparing prevalence between age groups, and although this was not a longitudinal study, our findings suggest a significant increase in the prevalence of cam-type FAI as age increases in women. These findings confirm previous data reported by our research team in contemporary osteological specimens with known sex and age. 32 Nonetheless, these suggestions should be confirmed with more comprehensive and longitudinal studies.
Another study reported a decreasing prevalence in the cam-type variant as age increased in both sexes. 16 However, that study did not perform subgroup analysis by age or sex. 6,16,29 Previous studies have suggested that the cam variant is an acquired phenomenon, particularly in men during the second growth spurt, and that it is highly influenced by exercise-related loads applied to the hip during this phase. 55
The 3 radiographic signs of cam-type FAI demonstrated a constant prevalence across age and sex, resulting in no significant differences in sex. This is in contrast to the findings of a previous study that demonstrated a higher prevalence of PGD in male versus female patients (26.13% vs 4.95%, respectively) without further analysis by age. 6
We found differences across age groups for PGD, LFFH, and coxa vara in male hips. As there are no previous studies with these comparisons, we cannot compare our results, however clear differences in the prevalence of these 2 signs were seen in the total population, with PGD being the most prevalent (26.3%). Our findings are comparable with those from another study that found a higher prevalence of increased alpha angle than that of PGD in asymptomatic participants. 59 In our study, 88.5% of participants with an alpha angle of >55° had a PGD. Notably, this is the sign most strongly associated with hip pain. 22
Therefore, we consider PGD, along with the alpha angle, as the most important radiographic sign for the screening of cam-type FAI. Nonetheless, comparative studies with symptomatic and asymptomatic participants are needed to truly determine the screening or diagnostic value of these variables. Another study found the prevalence of these signs to be very similar to our findings (PGD: 21.5% in men and 3.3% in women; FPFN: 10.3% in men and 2.6% in women; and LFFH: 14.4% in men and 6.2% in women), although they did not perform a subgroup analysis by age. 11 A previous study reported that the NSA decreases with age, causing an increase in the prevalence of coxa vara; its values were also lower in female patients. 6 These results are consistent with ours, in which a significant increase in the prevalence of coxa vara was found with increasing age, for both male and female hips.
Pincer-Type Variant
A recent systematic review reported that approximately two-thirds of asymptomatic patients have morphological characteristics of pincer-type FAI on imaging. 11 This high prevalence may be inaccurate to some extent because the morphological characteristics were poorly defined among the studies and the accuracy of the radiographic markers and imaging tools were also questionable. 46 These factors could explain the majority of the variability across studies that have evaluated the prevalence of this variant. Other studies have reported a prevalence of 15.2% and 27% for male patients and 19.4% and 21% for female patients, 1,14 which is similar to the results obtained in the current study (27.9% for male hips, 16.6% for female hips) probably because of the similar selection criteria.
Pincer-type FAI has been reported as being more common among middle-aged active women. 38 In contrast, some other studies have not found differences between sexes. 4,26,34 A study by Laborie et al 23 reported a higher prevalence of this variant in men versus women (34% vs 17%, respectively). Therefore, uncertainty remains regarding sex-based differences.
Our study suggests that the prevalence of this variant increases with age in both male and female patients. This has been similarly reported by Li et al 26 in a population aged between 12 and 19 years. However, we cannot further compare our findings because the other 2 studies that made this comparison were performed in a young population. 11,30
Regarding radiographic signs of pincer-type FAI, we found that COS was the most prevalent (17.0% in the overall population and 70.2% in hips with the pincer variant). In a 2016 systematic review, 27 the COS was positive in 28.5% of the asymptomatic participants, and other studies have reported a prevalence of 30%, 24.6%, 20%, and 18.5% in White American, Indian, Korean, and Brazilian populations, respectively. 1,2,36,54 Additionally, 1 recent study determined that the COS was well-correlated with findings obtained by MRI and with other radiographic findings commonly associated with pincer-type FAI. 57 In contrast, other studies have not found significant correlations between this radiographic sign and acetabular retroversion or chondral degeneration. The PWS and EAC have not been thoroughly studied and seem to be less prevalent than the COS. In this regard, a previous study reported similar findings to ours, as the authors found a higher prevalence of os acetabuli in male patients, although they did not perform an age subanalysis. 6
Regarding the AI as another marker for acetabular overcoverage, Lepage-Saucier et al 24 reported a mean AI of 6° without sex-based differences, Chakraverty et al 4 found a mean AI of 4.4° in young asymptomatic men and women, and Mineta et al 29 reported lower AI values in men older than 40 years. In our study, we identified the same pattern as Mineta et al and the differences were significant.
Strengths and Limitations
Our study was strengthened by the large sample size of hips from an asymptomatic population, which was based on an a priori power sample calculation. Thus, we determined the minimum number of participants required with appropriate methodology to ensure internal validity, which was reinforced by intraobserver and interobserver reliability and by high external validity from our rigorous selection criteria.
The main limitation of our study was that the data were obtained from plain radiographs, and we used only 1 projection, which might not have been sensitive enough to detect all FAI-related morphological abnormalities. Although radiographs were taken according to a standardized protocol, there was some degree of variation as a result of individual technique. This variability was minimized with the standardized technique being performed at a single institution. We recognize that an important limitation of the study was the determination of the cam-type variant on AP pelvic radiographs, as it has been established by previous studies that the most sensitive radiographic projection for this deformity is the 45° Dunn view.
Our study has some further limitations. We only included Hispanic people; therefore, the external validity of our study is limited to this population, and further studies in other ethnic groups are required to confirm our findings. Moreover, this was a noncontrolled retrospective and descriptive study. This renders impossible a true analysis of the diagnostic value of the variants and signs analyzed or a correlation of our findings with the symptoms and personal history of participants.
Another limitation was that we classified a patient as asymptomatic based on a retrospective analysis of the interview and physical examination performed in the past; although the majority of clinical evaluations were carried out by one of the authors (R.M.-A.), this did not happen in all cases. In all cases, the symptoms taken into account were pain and functional limitations, and an exploration of provocation maneuvers specific to FAI were not performed in all cases. Finally, this was a cross-sectional study, and suggestions of time-dependent changes in the prevalence of the studied variables need to be compared with further findings of longitudinal studies.
Conclusion
We demonstrated by radiographic findings that the characteristics suggestive of FAI, both the cam and pincer variants, were common in a population of healthy young adults, especially in men, with a high degree of coexistence between most of the findings. As the available literature on the cause of FAI suggests that it is multifactorial, we believe that these findings may reflect anatomic variations rather than true pathological abnormalities. This is the first study to determine the true prevalence of cam and pincer variants as well as their more commonly associated radiographic signs distributed by sex and age. The findings contribute to the increasing knowledge on the prevalence of cam and pincer FAI according to sex and age, demonstrating that they can exist in an asymptomatic population. This will help clinicians correlate the radiographic findings and demographic data of the patient within the context of pain and limitations in the hip.
Footnotes
Acknowledgment
The authors acknowledge Neri Alvarez-Villalobos, MD, PhD, from the Research Division, Department of Statistics, School of Medicine, University Hospital “Dr José Eleuterio González,” Universidad Autónoma de Nuevo León, for his technical guidance in conducting and analyzing the study.
Final revision submitted August 3, 2020; accepted August 10, 2020.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the ethics and research committee of the School of Medicine, University Hospital “Dr José Eleuterio González,” Universidad Autónoma de Nuevo León (registration No. AH14-008).
Appendix
Prevalence of Cam and Pincer Variants in Different Studies of Asymptomatic Populations a
| Lead Author (Year) | Study Type (LOE) | No. of Patients/Hips | M:F Sex b | Age, c y | Diagnosis | Morphology Definitions | Imaging d | Prevalence, % | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Cam | Pincer | Cam | Pincer | |||||||
| Clohisy 5 (2007) | Retrospective | 24 hips | 54%:46% | 35 (18-49) | Back and leg pain on physical examination | FHS, FHNO, alpha angle (cutoff point not specified) | NA | 1. Frog-leg lateral view 2. AP pelvic view 3. Cross-table lateral view |
21 | NA |
| Hack 15 (2010) | Prospective | 200 patients (400 hips) | 89:111 | 29.4 (24.1-50.6) | Asymptomatic by physical examination of hips and impact test with patient supine | Alpha angle >50.5° | NA | MRI | 53 | NA |
| Kang 19 (2010) | Prospective (4) | 50 patients (100 hips) | 23:27 | 15-40 | Asymptomatic by clinical interview and medical history review | Alpha angle >55°, FHNO <8 mm, FHS | AVA <15°, COS, LCEA >40° | CT | 10 (alpha angle), 12 (FHNO) | 16 |
| Pollard 41 (2010) | Prospective | 83 patients (166 hips) | 39:44 | M: 47.5; F: 44.4 | Asymptomatic by clinical interview, review of medical records, and physical examination | Alpha angle >50°, FHNO <14 mm | NA | 1. AP pelvic view 2. Cross-table lateral view |
12.04 | NA |
| Reichenbach 45 (2010) | Prospective | 244 patients (only 1 hip per patient examined) | 244:0 | 19.9 ± 0.7 | Asymptomatic by self-reported questionnaire and physical examination | FHNO (grade 2 and 3), alpha angle | NA | MRI | 24 | NA |
| Jung 18 (2011) | Retrospective | 380 patients (760 hips) | 108:272 | M: 62.5; F: 59.5 | Asymptomatic by physical examination | M: alpha angle >83°; F: alpha angle >57° | NA | CT | 7.89 | NA |
| Laborie 23 (2011) | Prospective | 2060 patients (4120 hips) | 868:1192 | 18.6 ± 0.6 (17.2-20.1) | Asymptomatic by physical examination and review of radiographs | PGD, FPFN, LFFH | EAC, COS, PWS | 1. AP pelvic view 2. Frog-leg lateral view |
M: 35.1; F: 10.2 | M: 34.3; F: 16.6 |
| Ranawat 43 (2011) | Prospective | 100 patients (200 hips) | 44:56 | 34.6 ± 11.3 | Unilateral symptomatic FAI on questionnaire and physical examination | FHS, FHNO, alpha angle, NSA, etc | COS, PWS, ISS, IIL-AF, etc | 1 AP pelvic view 2. Cross-table lateral view |
21.5 | 18.5 |
| Silvis 50 (2011) | Prospective (3) | 39 patients (78 hips) | 39:0 | ND | Asymptomatic by physical examination, questionnaire, and clinical interview | Alpha angle >50° | NA | MRI | 39 | NA |
| Miguel 28 (2012) | Retrospective | 100 patients | 42%:58% | 31 | Asymptomatic by review of radiographs and medical records and physical examination | FHS, alpha angle (cutoff point not specified) | LCEA, AI, AVA (cutoff point not specified) | 1. AP pelvic view 2. 45° Dunn view 3. Ducroquet view 4. Lequesne false profile view |
3 (presence of bump on AP pelvic view), 24 (presence of bump on 45° Dunn view) | ND |
| Sutter 51 (2012) | Retrospective | 53 patients (106 hips) | 31:22 | 34.5 (20-50) | Asymptomatic by clinical interview and physical examination | Alpha angle >55° | NA | MRI | 53 | NA |
| de Bruin 6 (2013) | Retrospective | 262 patients (522 hips) | 100:162 | 20-56 | Asymptomatic by questionnaire and physical examination | PGD, FHFNR, NSA <125° | LCEA >39°, AI <0°, CP, protrusio acetabuli, os acetabuli, herniation pit | AP pelvic view | Total: 7.7; M: 15.6; F: 2.8 | Total: 63.2; M: 44.2; F: 74.9 |
| Joo 17 (2013) | Retrospective | 497 patients (994 hips) | 186:311 | M: 50.02 (19-96); F: 58.19 (18-86) | Asymptomatic by review of medical records | M: alpha angle ≥83°; F: alpha angle ≥57° | NA | MRI | M: 0.5 (alpha angle ≥83°); F: 3.1 (alpha angle ≥57°) | NA |
| Leunig 25 (2013) | Cross-sectional | 80 patients | 0:80 | 19.3 (18-99) | Asymptomatic by questionnaire and measurement of hip internal rotation | FHNO (grade 2 and 3) | Depth of acetabulum <3 mm, labral lesions | MRI | 22 (grade 1) | 10 (depth of acetabulum), 97 (labral lesions) |
| Monazzam 30 (2013) | Retrospective | 225 patients (244 F hips, 206 M hips) | 103:122 | 10.4 (2-19) | Asymptomatic by review of medical records | Alpha angle >50° and >55° | LCEA >40°, TA <0° | CT | M: 10.2; F: 2.5 | M: 12.1; F: 9.4 |
| Nepple 34 (2013) | Retrospective (3) | 33 hips | 32%:68% | 30.5 (13.7-50.9) | Asymptomatic by physical examination and medical history | NA | CP, LCEA >40°, AI <0° | AP pelvic view | NA | 76 |
| Chakraverty 4 (2013) | Retrospective | 50 patients (100 hips) | 30:20 | 30.8 ± 6.1 (20-40) | Asymptomatic by review of radiographs and medical records | Alpha angle >55°, FHNO <8 mm, PGD | AVA <15°, AI <0°, COS, LCEA >40°, PWS | CT | M: 60.0; F: 26.7 | M: 36.7; F: 42.5 |
| Khanna 21 (2014) | Prospective | 170 patients (318 hips) | 77:93 | 29.5 (25.7-54.5) | Asymptomatic by physical examination without history of hip or groin pain | Alpha angle >55° and >60° | NA | MRI | 11.6 (alpha angle >55°), 9.4 (alpha angle >60°) | NA |
| Scheidt 47 (2014) | Prospective | 82 patients (164 hips) | 28:54 | 50.4 (40-60) | Asymptomatic by clinical interview and physical examination | Alpha angle >50°, NSA <125° | LCEA >40°, AI <0°, COS, ISS, PWS | 1. AP pelvic view 2. 45° Dunn view of both hips 3. Lequesne view |
25 | 12.65 |
| Diesel 9 (2015) | Prospective | 184 patients | 91:93 | Total: 20-60; M: 29 (26.5-41.5); F: 44 (28-52) | Asymptomatic without history of hip pain or orthopaedic disease | Alpha angle >55° | LCEA >40°, AI <0°, COS | 1. AP pelvic view 2. 45° Dunn view |
18.92 | 18.5 (COS), 2.4 (LCEA), 27.6 (AI) |
| Kim 22 (2015) | Retrospective | 430 patients (473 hips) | 292:181 | M: 31; F: 34 | Asymptomatic by review of medical records | Alpha angle >55°, FHNO <8 mm | AVA <15°, LCEA >40° | CT | M: 20.2 (alpha angle); F: 14.4 (alpha angle); M: 11.3 (FHNO); F: 8.3 (FHNO) | M: 31.2 (AVA); F: 22.1 (AVA); M: 28.4 (LCEA); F: 23.8 (LCEA) |
| Li 26 (2017) | Retrospective (3) | 558 patients (1116 hips) | 276:282 | 14.4 (10-18) | Asymptomatic by review of medical records | Alpha angle >55° | LCEA >40° | CT | Total: 16.8; M: 23.9; F: 9.9 | Total: 32.4; M: 29.7; F: 35.1 |
| Nardo 33 (2015) | Retrospective (3) | 4140 patients (8151 hips) | 4140:0 | 77 ± 5 | Asymptomatic by physical examination | Impingement angle <40°, NSA <125° | LCEA >40° | AP pelvic view | 29 | 57 |
| Van Houcke 54 (2015) | Prospective | 201 patients (402 hips) | 105:96 | ND | Asymptomatic by clinical history and physical examination | Alpha angle >55°, anterior offset ratio <0.13, NSA <125° | AVA <15°, COS, ISS, TA <5°, LCEA >45° | CT | 24 (Chinese), 40 (White) | 32 (Chinese), 16 (White) |
| Ahn 1 (2016) | Prospective | 200 patients (400 hips) | 146:254 | 34.7 (21-49) | Asymptomatic by clinical interview, physical examination, and review of medical records | Alpha angle >55° | COS, LCEA >40°, PWS | 1. AP pelvic view 2. Sugioka view 3. 45° Dunn view of both hips |
Total: 38; M: 57; F: 26 | Total: 23; M: 27; F: 21 |
| Mineta 29 (2016) | Retrospective | 600 hips | 352:248 | 58.2 (20-89) | Asymptomatic by review of radiographs | Alpha angle >55°, FHNO ratio <0.15 | LCEA >40°, COS, AI <0° | CT | Total: 45.3; M: 54.4; F: 32.3 | Total: 37.4; M: 41.7; F: 31.3 |
| Yepez 58 (2017) | Prospective | 56 patients (112 hips) | 56:0 | 15.3 (13-18) | Asymptomatic by physical examination, presence of current symptoms, and review of medical records | Alpha angle >55°, FHNO <7 mm | LCEA >40°, AI <0° | MRI | 77.7 | 10.7 |
| Monckeberg 31 (2017) | Prospective | 142 patients (72 without skeletal maturity, 70 with skeletal maturity) | 142:0 | Group 1: 15.4 ± 0.8 (12-16); group 2: 24.0 ± 3.3 (19-36) |
Asymptomatic by clinical interview and review of medical history | Alpha angle >55°, FHNO <8 mm | COS, LCEA >40° | AP pelvic view | 47.2 (immature group), 48.5 (mature group) | 41.6 (immature group), 51.4 (mature group) |
| Thier 53 (2017) | Retrospective | 110 patients (114 hips) | 60:50 | 56 (18–100); ± 22.4 | Asymptomatic by clinical interview and review of medical history | Alpha angle >55°, FHNO <0.18 | COS, LCEA >40° | 1. AP pelvic view 2. Cross-table lateral view |
43 | 13 |
| Pachore 36 (2018) | Prospective | 452 patients (904 hips) | 282:170 | 29.9 ± 6.06 | Asymptomatic by physical examination | Alpha angle >55°, PGD | LCEA >40°, AI <0°, COS, ISS, PWS | AP pelvic view | 6.6 (alpha angle), 2.9 (PGD) | 24.6 (COS), 22.4 (ISS), 17.5 (LCEA), 13.4 (AI) |
| Polat 40 (2018) | Retrospective | 1076 patients (2152 hips) | 474:602 | Total: 42.1 ± 15.6 (18-65); M: 39.1 ± 15.3; F: 44.5 ± 15.4 | Asymptomatic by telephone questionnaire | Alpha angle >55° | LCEA >40°, TA <0°, COS | 1. AP pelvic view 2. Frog-leg lateral view |
15.9 | 10.6 |
| Current study | Retrospective (3) | 939 patients (1878 hips) | 1280:598 | Total: 31.0 ± 9.2 (18-50); M: 32.3 ± 10.4; F: 28.6 ± 14.4 | Asymptomatic by review of radiographs and medical records | Alpha angle >55°, PGD, FHFNR <1.27, FPFN, LFFH, NSA <125° | LCEA >40°, TA <0°, COS, PWS, EAC | AP pelvic view | Total: 29.7; M: 34.7; F: 19.1 | Total: 24.3; M: 27.9; F: 16.6 |
a In some studies, both symptomatic and asymptomatic participants were used, and for this table, only the sample size and prevalence of the asymptomatic patients were considered. AI, acetabular index; AP, anteroposterior; AVA, acetabular version angle; COS, crossover sign; CP, coxa profunda; CT, computed tomography; EAC, excessive acetabular coverage; F, female; FAI, femoroacetabular impingement; FHFNR, femoral head–to–femoral neck ratio; FHNO, femoral head-neck offset; FHS, femoral head sphericity; FPFN, focal prominence of the femoral neck; HP, herniation pit; IIL-AF, distance from the ilioischial line to the acetabular fossa; ISS, ischial spine sign; LCEA, lateral center-edge angle; LFFH, lateral flattening of the femoral head; LOE, level of evidence; M, male; MRI, magnetic resonance imaging; NA, not applicable; ND, no data; NSA, neck-shaft angle; PA, Protusio acetabulli; PGD, pistol-grip deformity; PWS, posterior wall sign; TA, Tönnis angle.
b Data are reported as n or %.
c Data are reported as mean, mean (range), mean ± SD, mean ± SD (range), or range.
d Radiographs are indicated by view.