
Abstract
Background:
Various technologies have been developed to quantify the pivot shift, as it is regarded as a key indicator of anterolateral rotatory laxity of the knee.
Purpose:
To determine the usefulness of a commercially available triaxial accelerometer (Kinematic Rapid Assessment [KiRA]) in numerically quantifying the pivot shift in patients under anesthesia with an anterior cruciate ligament (ACL)–deficient knee.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
Both knees of 50 patients (26 male [mean age, 30.4 years], 24 female [mean age, 26.6 years]) under anesthesia were assessed immediately before unilateral ACL reconstruction by an orthopaedic fellow and 1 of 3 experienced knee surgeons. The pivot-shift grade and 2 KiRA outputs (range of acceleration and slope of acceleration change) were compared.
Results:
The surgeon and fellow recorded the same pivot-shift grade for 45 of 50 patients (90%). Data from the 5 patients with no agreement and 1 patient with extreme outlying data were excluded from subsequent analysis. Using the KiRA range and slope data, the surgeon identified the injured knee in 74% and 76% of patients, respectively, while the fellow’s rate of injured knee identification was 74% and 80%, respectively. A correlation could be found only between pivot-shift grade and surgeon-derived range data (ρ = 0.40; P < .01) but not slope data or any fellow-derived outputs. Using the surgeon-derived range data, there was a significant difference between a grade 3 pivot (>5 m/s2) and a grade 1 or 2 pivot (<5 m/s2) (P = .01).
Conclusion:
Although a correlation between KiRA output data and pivot-shift grade was found when the device was used by an experienced surgeon, there was no correlation when used by a well-trained but less experienced orthopaedic fellow. Furthermore, the KiRA output data identified the ACL-deficient knee correctly in only 74% of patients. Although a threshold acceleration range value could be identified, above which the value was associated with a grade 3 pivot shift, this was dependent on the examiner, and distinction between other grades could not be made.
Clinical examination of the anterior cruciate ligament (ACL)–injured and ACL-reconstructed knee involves assessment of anterior tibial translation using the Lachman or anterior drawer test and anterolateral tibial translation using tests, such as the pivot-shift test. For the diagnosis of an ACL rupture, the Lachman test has been shown to have good sensitivity (85%) and high specificity (90% to 95%), whereas the pivot-shift test has been shown to have poor sensitivity but an even higher specificity. 4,27 Assessment of pivot-shift severity is important, as it is correlated with patient outcomes after ACL reconstruction, unlike postoperative measurements of anterior knee laxity, which do not. 20 More recently, a high-grade preoperative pivot shift has been suggested as an indication for an additional anterolateral procedure in the setting of ACL reconstruction. 8
Although other clinical classifications have been described, 15 the pivot-shift test is typically graded on a scale from 0 to 3 (0, no pivot; 1, pivot glide; 2, clunk; 3, explosive/gross clunk) per the International Knee Documentation Committee. 12,14 However, not only is such grading subjective and dependent on what the examiner feels, but there is also considerable variation in how the test is performed in terms of the technique, the magnitude of the applied loads, and the speed at which the limb is moved. 20 In an attempt to address these inconsistencies and more reliably quantify the pivot shift, various technologies have been developed. Some have used instrumented boots or footplates and navigation systems, 7,11,21,23 but the limitations of these devices are cost; size of the equipment; and, in the case of navigation, the associated morbidity of pin sites, making them impractical for daily clinical use. Other approaches have included the use of accelerometers, electromagnetic sensors, and image analysis of surface markers, and all have shown promise. 11,28,29
The Kinematic Rapid Assessment (KiRA; OrthoKey) is one such device, which is based on a noninvasive triaxial accelerometer device attached to the proximal tibia. The range and rate of change of acceleration (jerk) during the pivot shift can be recorded. The reliability and validity of the KiRA to quantify the pivot shift have been tested. In a study of 66 patients under anesthesia with chronic unilateral ACL deficiency who were examined by a single observer (expert surgeon), statistically significant differences between the normal and abnormal knees were found for maximum and minimum acceleration values, acceleration range, and jerk. 22 Intratester reliability was fair to good for most parameters, although it was better for the affected limb than the normal limb. In a subsequent study, statistically significant differences in maximum acceleration were found between the ACL-deficient knee and the contralateral knee. 5 There was a definite learning curve, and the ability to correctly identify the injured knee improved with experience in using the device, from a specificity of 50% to 90%. There were no statistically significant differences in the values obtained by an experienced surgeon, a resident, and a student. In a more recent study of patients under anesthesia who were examined by a single observer (senior surgeon), the authors reported a correlation between the acceleration range and the grade of pivot shift. 13 The results of these 3 studies point to the possible utility of the KiRA device to assign a numerical value to the pivot shift. What is lacking, however, is evidence to show that the KiRA device can or cannot correctly identify the pivot-shift grade in the hands of users with varying levels of clinical experience.
The purpose of this study was therefore to evaluate the ability of the KiRA device, in the hands of multiple users, to correctly identify the ACL-injured knee in the patient under anesthesia and to assign a numerical score to the pivot shift that correlates with expert clinical rating.
Methods
Ethical approval was granted by the institutional research ethics committee to conduct this study. Data were collected between September 4 and November 24, 2017.
Recruitment and Exclusion Criteria
Patients undergoing primary ACL reconstruction by 1 of 3 experienced knee surgeons were considered for inclusion in this study. Patients were excluded if they had any additional ligamentous injury with laxity in the affected knee, a known displaced meniscal tear, or any previous ligament injury with resultant laxity or ligament surgery in the contralateral knee. All participants gave informed consent before participation.
Examiners
There were 4 examiners involved in this study: 3 were the operating surgeons (J.A.F., B.M.D., T.S.W.), and 1 was a fellowship-trained orthopaedic surgeon (R.J.N.) (the orthopaedic fellow). Each surgeon performed the test on one’s own patients, and the orthopaedic fellow acted as an independent examiner and performed the same test on all participants.
Assessment Device
As described previously, the KiRA device is a triaxial accelerometer fixed to the proximal lateral leg using an elastic strap (Figure 1). Acceleration data from the device are transferred to a tablet computer running the associated proprietary software. Two parameters are displayed in real time, and these are averaged over the 3 repetitions: (1) the range between the maximum and minimum acceleration (m/s2) and (2) the slope, which is described by the manufacturers as representing the mean of the jerk (with jerk being the rate of change in acceleration) (Figure 2).
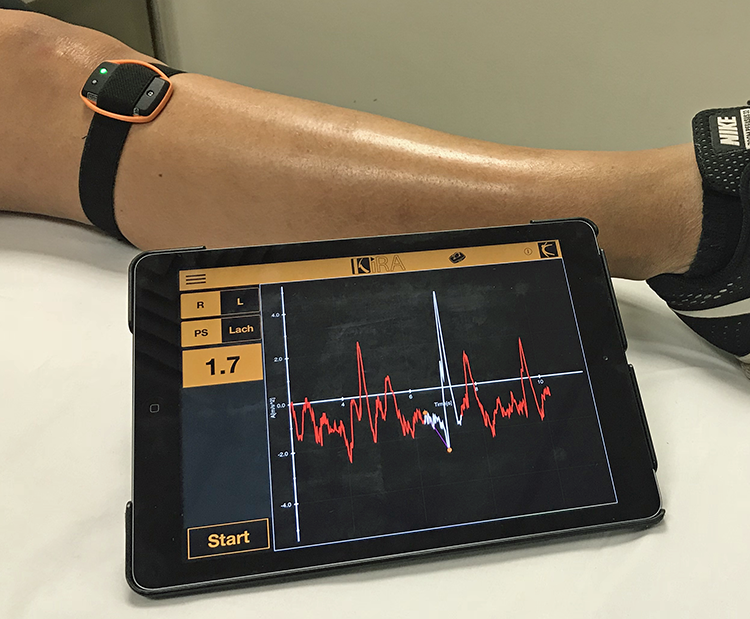
The KiRA (OrthoKey) accelerometer attached to the proximal leg. The tablet displays and records the acceleration data. KiRA, Kinematic Rapid Assessment.

KiRA (OrthoKey) acceleration data output for an anterior cruciate ligament–deficient left knee. The white component of the graph represents the pivot episode being analyzed by the software, with the superior orange dot representing maximum acceleration (m/s2) and the inferior representing minimum acceleration (m/s2). Data output of 7.4 and 5.1 for left and right, respectively, represent the difference between maximum and minimum acceleration (ie, the range). The purple line connecting these is the mean of the rate of change of acceleration or jerk (m/s3) (ie, the slope). IKDC, International Knee Documentation Committee; KiRA, Kinematic Rapid Assessment; L, left; Lach, Lachman; PS, pivot shift; R, right.
Procedure
All examiners were shown a video supplied by the manufacturer demonstrating the recommended technique for performing the pivot-shift test using the KiRA device. This involves flexing the knee from the extended position with the tibia internally rotated while applying a valgus and vertical compressive force to the joint.
Testing was carried out after induction of general anesthesia and before application of the tourniquet. The accelerometer was positioned and fixed to the proximal tibia between the Gerdy tubercle and the tibial tuberosity, in accordance with the manufacturer’s instructions. The device was applied by the orthopaedic fellow in all cases.
One examiner performed the test on both knees (nonaffected knee first), and the other acted as an observer. Both knees were tested to determine whether the KiRA device could correctly identify the ACL-deficient knee. The examiner was unable to see the screen of the tablet during testing. Repeated pivot-shift maneuvers were performed until consistent traces of acceleration on the tablet were noted by the observer, as recommended by Berruto et al. 5 If the observer perceived any inconsistency between limbs in the speed or force being used, the test was repeated. The examiner made a judgment about the grade of the pivot shift using the International Knee Documentation Committee classification described earlier (ie, grade 0-3) but did not share this with the other examiner until both had completed their assessment. The orthopaedic fellow completed the assessment first, followed by the operating surgeon.
To ensure that all examiners were familiar with the testing protocol, a pilot study involving 20 patients was conducted, based on the recommendations from the manufacturer and other published studies, 5,22 to ensure familiarization with the device and standardization of the pivot-shift test procedure. During pilot testing of the device, it was observed that all assessors tended to perform the test more slowly in the ACL-deficient knee as compared with the contralateral knee. Slowing the test in the contralateral knee to the same speed as the ACL-deficient knee appeared to improve the ability of the KiRA to correctly identify the ACL-deficient knee. Significant force during testing on the injured or uninjured limb, even if the speed was comparable, also changed the output recorded by the KiRA. Therefore, during the study, every effort was made to ensure that the examiner used the same force and speed of testing on both sides.
Statistical Analysis
Statistical analysis of the data was performed using SPSS (Version 20.0.0; IBM Corp). The number of occasions in which the operating surgeon and the orthopaedic fellow agreed on the pivot-shift grading was calculated and presented as a percentage agreement. Given that the clinical grading was the reference point against which the KiRA output data were being compared, only data from participants for whom the operating surgeon and the orthopaedic fellow agreed on the pivot-shift grading were included in the subsequent analysis.
The agreement between assessors for the KiRA outputs of range and slope was assessed using Spearman ρ and an intraclass correlation coefficient (3,1) for the entire cohort, where (3,1) refers to the pooling of the 3 senior surgeons for comparison with the fellow. This analysis was then repeated for 3 groups of the cohort based on the clinical grading (1, 2, or 3; there were no cases of grade 0). One-way analysis of variance was performed to determine whether the KiRA outputs (range and slope) were significantly different among the clinical grading categories (1, 2, or 3). This was conducted separately for the orthopaedic fellow and the operating surgeons. Owing to multiple comparisons, the Bonferroni correction was applied with statistical significance set at P < .01.
Results
A total of 59 patients were initially assessed in the operating room. Four were excluded after assessment when it was established that they had ligamentous laxity in the contralateral knee. A further 5 were subsequently excluded for intraoperative identification of a displaced bucket-handle meniscal tear. This left 50 participants for analysis: 26 male (mean age, 30.4 years) and 24 female (mean age, 26.6 years).
The operating surgeon and the orthopaedic fellow recorded the same pivot-shift grade clinically for 45 of 50 patients (90%). The data from the 5 patients for whom there was not agreement were excluded from subsequent analysis of the KiRA data.
Initial review of the KiRA output data identified 1 patient with extreme outlier data, which were excluded from subsequent analysis. Overall, there was no significant correlation between the surgeon and fellow data for range (ρ = 0.12; P = .4) or slope (ρ = 0.11; P = .5).
When the surgeon performed the assessment, KiRA range data correctly identified the injured knee in 74% of patients. Surgeon-derived KiRA slope data correctly identified the injured knee in 76% of patients. When the fellow performed the assessment, the percentages were 74% and 80%, respectively.
Surgeon-derived range data showed a correlation between pivot-shift grade and range (ρ = 0.40; P < .01), whereas data for the orthopaedic fellow showed no correlation. When the surgeon-derived range data were analyzed by pivot-shift grade, there was a significant difference between the knees with a grade 3 pivot shift and those with a grade 1 or 2 (P = .01) (Table 1). Furthermore, an acceleration range >5 m/s2 indicated a grade 3 pivot shift, and a range <5 m/s2 indicated a grade 1 or 2. There was no significant difference in range between grade 1 and 2 pivot shift. No relationship was identified for the fellow-derived data, for whom the range was around 5 m/s2 for all grades of pivot shift.
Clinical Pivot-Shift Grade and KiRA Acceleration Range Stratified by Examiner a
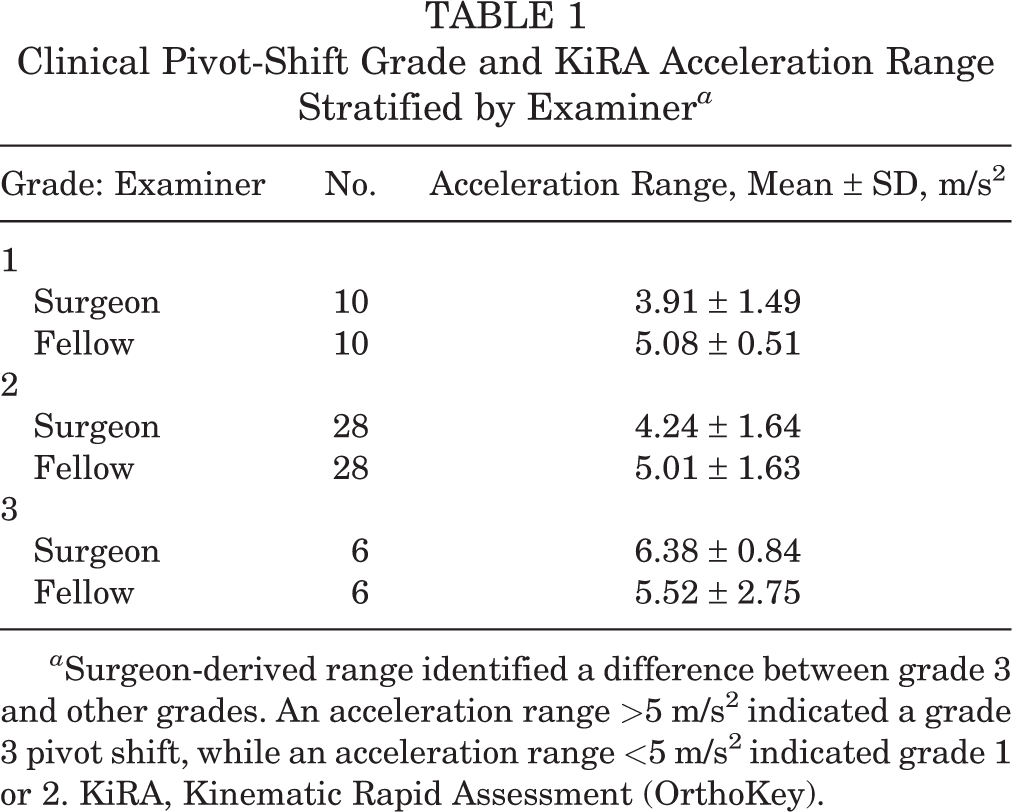
a Surgeon-derived range identified a difference between grade 3 and other grades. An acceleration range >5 m/s2 indicated a grade 3 pivot shift, while an acceleration range <5 m/s2 indicated grade 1 or 2. KiRA, Kinematic Rapid Assessment (OrthoKey).
There was no correlation between pivot-shift grade and slope for either the surgeon or the fellow.
Discussion
Overall, the results of this study do not support the use of the KiRA device alone to assign a numerical value to the pivot-shift phenomenon. This was despite testing the device in what might be considered the ideal situation—a patient under anesthesia with an ACL-deficient knee and a normal contralateral knee and after pilot testing and formal instruction in using the device. The KiRA acceleration range and slope data identified the ACL-deficient knee correctly in only 74% to 80% of patients, less than the previously reported rates for standard clinical tests. 4,27 There was some correlation between certain KiRA output data and clinical pivot-shift grade. When the device was used by experienced orthopaedic surgeons, acceleration range showed a moderate correlation with the pivot-shift grade but not when used by a well-trained but less experienced orthopaedic fellow. However, acceleration slope showed no correlation with the pivot-shift grade, regardless of whether the surgeon or fellow used the device. Furthermore, there was no correlation between the surgeon- and fellow-derived outputs for range and slope.
Although the results of this study do not support the routine use of the KiRA device for quantifying the pivot shift, they are nonetheless consistent with previous studies that have been more positive about the potential value of using the device. Lopomo et al 22 reported that when used by an experienced surgeon, the KiRA device correctly identified the injured knee in 70% of patients based on the slope value and in 80% based on the range value. Berruto et al 5 examined 100 patients with ACL-deficient knees using the KiRA and stated that the efficacy of the device was related to its learning curve, achieving 50% specificity in identifying the ACL-deficient knee after 20 uses of the device but 90% specificity by the conclusion of the study. In a recent study of 295 patients under anesthesia with ACL-deficient knees who were examined by an expert surgeon, Helfer et al 13 reported that the side-to-side difference in the tibial acceleration range, as measured using KiRA, was correlated with the pivot-shift grade. This is in keeping with the findings of the current study that surgeon-derived acceleration range data were correlated with the pivot-shift grade, albeit with a lower coefficient value (0.40 vs 0.57).
There is valid interest in being able to assign a numerical value to the pivot-shift phenomenon. With increasing interest in the role of the anterolateral structures of the knee in the setting of ACL rupture and the potential value of anterolateral repair, augmentation, or reconstruction, having a numerical value of anterolateral rotatory laxity may help the clinician to decide when additional surgery to an ACL reconstruction is warranted. Such a numerical value may also be a useful tool in assessing the success of an intervention in restoring stability to the knee. However, the results of the current study and previous similar studies show that the KiRA device does not at present provide a tool that meets this purpose. The ideal device should be able to be used by a range of examiners and not be dependent on all examiners using a close-to-identical pivot-shift testing technique, although the overall method of performing the pivot-shift test needs to be consistent among examiners (eg, starting the test in extension and the leg in internal rotation). In addition, the ideal device should be able to be used with the same certainty in patients who are awake as for those under anesthesia. At a minimum, it should have a very high specificity in identifying the ACL-deficient knee, but to be truly useful, it should be able to distinguish among all 4 grades (0-3) of the pivot shift and, ideally, provide a numerical assessment of the pivot shift on a continuous scale. The KiRA device output data in this study were able to distinguish between grade 3 and other grades of pivot shift but not between grades 1 and 2. The International Anterolateral Complex Consensus Group Meeting suggested that a high-grade pivot shift may be an “appropriate indication” for the addition of a lateral augmentation procedure. 8 Moreover, it is interesting that a grade ≥2 pivot shift was one of the inclusion criteria in a recent randomized controlled trial by Getgood et al, 9,10 who compared the 2-year outcomes of a large cohort considered to be at high risk of reinjury after ACL reconstruction. Therefore, if a grade 2 pivot shift is to be used as an indication for a lateral augmentation procedure, then it is important that a device be able to distinguish between grades 1 and 2.
The modest and somewhat inconsistent correlations between the KiRA outputs and the pivot-shift grade that have been reported may reflect the fact that the clinical grading of the pivot-shift test is a complex and subjective assessment and that there are variations in technique among examiners. It includes assessment of the translation of the lateral tibial plateau, with an evaluation of the inherent resistance to this translation, as well as an assessment of the velocity of tibial reduction. 3,15,17,26 Examiners feel; see; and, in some cases, hear the pivot shift, and terms, such as pivot glide, shift, and clunk, are used to imply increasing levels of severity. The KiRA, however, measures only parameters of acceleration. Nonetheless, in a cadaveric model and with examination by 12 expert surgeons, parameters of acceleration have been reported to be best correlated with the grade of pivot shift, although it was also recognized that the acceleration component of the pivot shift is not an intuitive concept and still not completely understood. 1,2 In an earlier study using electromagnetic motion capture sensors in patients who were awake, Labbe et al 18 found that acceleration and velocity of tibial translation were the features that were most useful for distinguishing among different recordings of the pivot-shift phenomenon.
Using microelectromechanical system sensors that integrate an accelerometer, gyroscope, and magnetometer attached to the tibia and the femur, Labbe et al 19 subsequently found a very strong correlation between the decrease in femoral acceleration and clinical pivot-shift grade (r = 0.84; P < .0001) and a strong correlation between the decrease in tibial acceleration and clinical pivot-shift grade (r = 0.69; P < .001). However, Kopf et al 16 used a similar system but did not find any correlation between acceleration parameters and pivot-shift grade. Labbe et al 19 attributed the different findings of the 2 studies to the use of ratios between the ACL-deficient and ACL-intact knees in the Kopf et al study. Interestingly, in the Labbe et al 19 study, femoral acceleration decrease was significantly different for each pair of pivot-shift grades except for grade 0 versus 1 and grade 2 versus 3, not dissimilar to the current study where there was a significant difference between the acceleration range data between grade 3 and grades 1 or 2 but not for other pairwise comparisons. Using more complicated analyses and support vector machine classifiers, Borgstrom et al 6 reported an accuracy of 77% in identifying the pivot-shift grade when inertial sensors were attached to the thigh and leg of patients who were anesthetized. The accuracy within 1 grade was 98%. In addition, the accuracy with which the system was able to diagnose whether a knee was ACL deficient was 97%. Thus, it appears that the use of sensors on both the leg and the thigh may improve the utility of systems using inertial sensors or similar sensors.
As noted earlier, for any device to be useful, it needs to have broad applicability. Specifically, it should be able to be used by examiners of varying levels of expertise and experience and still generate consistent outputs. In a study using 2 cadaveric models, an electromagnetic tracking system, and 25 examiners of varying training and experience, Naendrup et al 24 demonstrated that, despite teaching and repetition being associated with improvements in the performance of the pivot-shift test, a high degree of variability persisted. External rotation during tibial reduction accounted for most of the variability, and it was concluded that more uniform technique and improved teaching are needed. 25 The current study used 2 levels of examiner expertise and experience (experienced orthopaedic surgeons and a qualified orthopaedic surgeon undertaking fellowship training), and a pilot study included video training and efforts to ensure a consistent pivot-shift examination technique among examiners. Nonetheless, even when the KiRA device was used in apparently ideal conditions (ie, patients under anesthesia with unilateral ACL deficiency), the results suggested that it does not, at present, have broad applicability. There was no correlation between the surgeon- and fellow-derived range or slope KiRA output data, despite the efforts made to ensure that all examiners used a consistent technique. It is also worth noting that the orthopaedic fellow used the device on more patients (140 knees) than did any of the surgeons and could therefore have been expected to have overcome any learning curve. Using 3 surgeons rather than 1 could be seen as a limitation in that it may have increased the variability in the use of the device. However, we believe that this approach reflects the reality of clinical practice and gives a better indication of the broader applicability of the device.
In the current study, the examiners were blinded to the KiRA output on the tablet. This was done to assess the generalizability of the device by ensuring that the examiner did not change technique in response to the acceleration trace on the tablet. The observer did, however, indicate when a consistent trace was being generated (and that testing could be stopped) in an effort to create a best-case scenario for assessment of the device.
Conclusion
This study found that the KiRA could correctly identify the ACL-deficient knee in only 74% of patients. A small correlation was identified between range of acceleration data and the clinical pivot-shift grading but only with the experienced examiners. Although a threshold acceleration range value could be identified, above which the value was associated with a grade 3 pivot shift, this was also dependent on the examiner, and distinction between other grades could not be made. Overall, the KiRA device does not presently appear to have broad applicability in grading the pivot shift. It should, however, be recognized that clinical grading of the pivot shift is a complex subjective assessment of many factors and reflects more than just acceleration of the tibia during the maneuver.
Footnotes
Final revision submitted July 20, 2020; accepted August 4, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.A.F. has received consulting fees from Smith & Nephew Endoscopy. B.M.D. has received speaking fees from Arthrex and Stryker. T.S.W. has received consulting fees from Medacta; speaking fees from Arthrex, Stryker, and Medacta; and royalties from Medacta. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Epworth HealthCare (No. EH2017-203).