
Abstract
Background:
Biceps tendon pathology is commonly associated with rotator cuff tears. A multitude of different biceps tenodesis techniques have been studied, with limited clinical data on arthroscopic biceps tenodesis techniques incorporated into rotator cuff repairs.
Purpose:
To evaluate the outcomes of an arthroscopic biceps tenodesis incorporated into a supraspinatus tendon repair.
Study Design:
Case series; Level of evidence, 4.
Methods:
Patients undergoing surgical treatment of supraspinatus tendon tears with concomitant biceps tendon pathology were prospectively enrolled from 2014 to 2015. A total of 32 patients underwent combined biceps tenodesis and rotator cuff repair; of these, 19 patients were evaluated for a mean of 2.0 years. The primary outcome measures were the American Shoulder and Elbow Surgeons Standardized Shoulder Assessment Form (ASES; patient self-report and physician assessment sections), visual analog scale (VAS) pain score, responses to specific biceps-related assessments, and biceps specific physical exam findings.
Results:
Patient-reported ASES scores improved from 45.9 preoperatively to 91.6 at the 2-year follow-up (P < .001). Pain VAS scores improved from 5.2 preoperatively to 0.7 at the 2-year follow-up (P < .001). Preoperatively, 18 patients had a positive Speed test; all were negative at 5 months postoperatively, and 21 patients had bicipital groove tenderness preoperatively, which resolved in all 21 patients at 5 months postoperatively. At the 2-year follow-up, 2 patients had cramping arm pain and 4 patients noticed a change in arm contour. There were no reoperations. No complications occurred in the study group.
Conclusion:
Arthroscopic biceps tenodesis incorporated into a supraspinatus tendon repair was a safe and reliable option for biceps pathology with a concomitant rotator cuff tear.
Lesions of the long head of the biceps (LHB) tendon and anchor commonly occur in association with rotator cuff pathology. 3,5 Chen et al 3 found that 76% of patients with rotator cuff tears had LHB pathology (tendinosis, tearing, or instability). The primary treatment strategies for biceps pathology include tenotomy and tenodesis. The advantages of a tenotomy can include shorter operative time and a faster return to activity, but the risks include a cosmetic Popeye deformity, 10,12 cramping biceps pain, and decreased supination strength. 16,22
Biceps tenodesis may reduce the risk of cramping pain and deformity but necessitates a longer operative time and can also include additional postoperative restrictions as well as a longer rehabilitation time. 9 However, if performed with a concomitant rotator cuff repair, postoperative restrictions are often the same regardless of whether a tenotomy or tenodesis is performed. Tenodesis is often preferred in younger active patients; however, studies have shown variable results. 4 Multiple tenodesis fixation techniques have been described, including interference screws, 8 suture anchors, 2 keyholes, 11 bone tunnels, 20 and sutures into soft tissue. Further, several tenodesis locations have been described, including incorporation into the rotator cuff, 2,7 conjoint tendon, transverse humeral ligament, suprapectoral region, and subpectoral region. 13 Most techniques require an additional surgical implant, which increases cost. Some techniques also require an additional surgical approach. A technique that combines biceps tenodesis with arthroscopic rotator cuff repair has been described 2,6,7,14,15,17 with clinical outcomes being reported by Checchia et al 2 and DeVito et al. 6 Of these, most techniques use the anterolateral anchor of a double-row repair, with the exception of Checchia et al and George. 7
The purpose of this study was to assess the outcomes after arthroscopic biceps tenodesis incorporated into a supraspinatus tendon repair, as these procedures are often performed concurrently. It was hypothesized that this arthroscopic technique for the treatment of concomitant biceps tendon and supraspinatus tendon pathology would significantly improve American Shoulder and Elbow Surgeons Standardized Shoulder Assessment Form (ASES) scores.
Methods
Study Population
Institutional review board approval was obtained for this study. Patients with clinical and imaging findings consistent with a supraspinatus tendon tear and biceps tendon pathology were recruited for study enrollment on a prospective basis. Inclusion criteria were as follows: age older than 18 years, repairable supraspinatus tendon tear, and concomitant biceps tendon symptomatology as well as pathology at the time of arthroscopy. Exclusion criteria were as follows: rotator cuff arthropathy, irreparable rotator cuff tears, revision rotator cuff repairs, and/or prior LHB tenotomy/tenodesis.
Outcome Evaluation
Enrolled patients were evaluated preoperatively as well as at 5-month, 1-year, and 2-year postoperative intervals. We created LHB-specific assessment forms for subjective patient outcomes as well as physical examination findings. The patient-reported assessments were completed at the above intervals and included the visual analog scale (VAS) for pain, the ASES, 19 and the created subjective biceps form (Figure 1). The senior author (C.W.U.) completed the ASES physician assessment form and the created biceps examination form (Figure 2) both preoperatively and at 5 months postoperatively.

Subjective long head of the biceps scoring questionnaire. Reported by patient at 5 months, 1 year, and 2 years postoperatively.

Physical examination maneuvers performed by the treating surgeon at 5 months postoperatively.
Surgical Technique
A diagnostic arthroscopy was performed through a standard posterolateral portal. An anterior portal was created, and the superior labrum/biceps complex probed; the biceps was pulled into the joint with the probe to evaluate groove pathology and instability. Partial rotator cuff tears were debrided and marked with a spinal needle as well as a No. 0 Prolene suture (Ethicon). Before addressing biceps pathology, the arthroscope was reintroduced through the posterior portal into the subacromial space, a lateral portal was created, and an extensive subacromial bursectomy was performed. Full-thickness rotator cuff tears were debrided of degenerative tissue, and high-grade partial supraspinatus tears were completed with an arthroscopic shaver. The arthroscope was then placed back into the glenohumeral joint through the posterior portal. If biceps pathology was identified (eg, medial instability, synovitis, partial-thickness tearing, superior labral anterior-posterior tear), an 18-gauge spinal needle was inserted through the anterior supraspinatus and then through the center of the biceps tendon. The needle was inserted an estimated 2 cm from the origin of the biceps tendon. If the supraspinatus was retracted more than 2 cm, the needle was passed through the retracted supraspinatus first and then levered to lateralize the supraspinatus tendon before piercing the biceps. A passing No. 0 Prolene suture was then placed in the spinal needle through the supraspinatus and biceps tendons and retrieved with a grasper and taken out of the anterior portal (Figure 3, A and B). The No. 0 Prolene was then exchanged with a No. 2 FiberWire (Arthrex) using a shuttle relay technique. An arthroscopic crab claw was then brought from the lateral portal through the supraspinatus tear to retrieve the FiberWire from the anterior intra-articular cannula. The biceps tendon was then tenotomized at its base (Figure 3, C and D).

Right shoulder viewed from posterior. (A and B) An 18-gauge spinal needle was placed through the anterior supraspinatus and biceps tendon. A No. 0 Prolene suture was placed through the spinal needle and retrieved through the anterior portal. (C and D) The No. 0 Prolene suture has shuttled No. 2 FiberWire through the rotator cuff and intact biceps tendon. A crab claw was placed from the lateral portal through the supraspinatus tear, pulling the intra-articular portion of the FiberWire suture out the lateral portal. The biceps tendon was then tenotomized. (E) After an anchor was placed, the previously placed FiberWire (black line) was used to shuttle the anchored suture through the biceps and supraspinatus tendon. (F) The suture, tied in simple (shown) or mattress fashion, incorporated the biceps tenodesis into the rotator cuff repair. (G) Final intra-articular view of biceps tenodesis and supraspinatus repair. (H) Final tenodesis and repair viewed from subacromial space.
The arthroscope was reintroduced through the posterior portal into the subacromial space; moreover, the anterior portal was reintroduced into the subacromial space over a switching stick. The 2 tails of the FiberWire shuttling suture were then docked in the anterior portal using a crochet hook. The rotator cuff repair and biceps tenodesis were then performed. Double-loaded biocomposite 5.5-mm corkscrew anchors (Arthrex) were placed, working anterior to posterior medial (double row) or midfootprint (single row) depending on tendon tissue loss. The shuttling suture tail exiting from intra-articular through the rotator cuff tear previously docked in the anterior cannula was then delivered out the lateral portal along with the most anterior anchor suture. The most anterior anchor suture was then shuttled through the biceps and torn supraspinatus by using a shuttle relay loop tied in the FiberWire shuttling stitch and pulling it out the anterior portal (Figure 3E). The remaining anchor sutures were passed and then tied arthroscopically. Smaller tears and large tears with tissue loss were repaired with a single-row simple suture configuration, while larger tears with minimal tissue loss were repaired with a double-row horizontal mattress configuration and suture bridge construct (Figure 3, F-H). All patients underwent a subacromial decompression. Distal clavicle excision was performed for patients with clinically symptomatic acromioclavicular joint arthritis.
Postoperatively, patients performed pendulums, saws, and table slides with no lifting of more than a coffee cup for 6 weeks. This was followed by 8 weeks of physical therapy including range of motion, scapular stabilization, and rotator cuff strengthening. Progression to full activities was allowed at 5 to 6 months postsurgically.
Statistical Analysis
ASES and VAS score differences from pre- to 2 years postoperatively were found to follow a normal pattern as assessed via the Shapiro-Wilk test for normality, QQ-plot, box plot, and histogram. The paired t test was used with a P value of .05 to statistically test whether the changes in ASES and VAS scores were significant from pre- to 2 years postoperatively. Cramping and strength were compared pre- and 2 years postoperatively using the McNemar test of agreement.
Results
Overall, 47 patients were recruited for the study between June 2014 and September 2015. Of these, 32 patients underwent combined arthroscopic biceps tenodesis incorporated into supraspinatus tendon repair. Nineteen were available for follow-up at 2 years (mean, 2.03 years; range, 1.87–2.17 years). The mean age was 63.0 years, and 82% were men. There were 4 high-grade partial tears, 11 complete tears involving just the supraspinatus, and 4 multitendon tears.
Results from the questionnaire are represented in Table 1. The mean ASES scores improved significantly (P < .001) from pre- to 2 years postoperatively. The mean increase in ASES score from preoperatively to 2 years postoperatively was 45.7 (95% CI, 32.74-54.55). The VAS pain scores decreased significantly from preoperatively to the 2-year follow-up (P < .001). These results demonstrated a mean decrease in pain of 4.5 (95% CI, 2.81-5.57).
Results of Patient-Reported Outcome Measures a

a Data are presented as mean ± SD or number of patients. ASES, American Shoulder and Elbow Surgeons Standardized Shoulder Assessment Form; VAS, visual analog scale.
There was no significant change in cramping “arm” pain from preoperatively to the 2-year follow-up (P = .10). In terms of elbow flexion and supination strength, there was no significant decrease from pre- to 2 years postoperatively (P = .31). No patient reported any difference in contour of the biceps compared with the contralateral side preoperatively. At 2 years, 4 patients reported a difference in contour compared with the nonoperative side.
Pertinent LHB examination maneuvers were recorded by the treating physician both pre- and 5 months postoperatively, as shown in Figure 2. A total of 21 patients were available for both pre- and postoperative testing. The results are shown in Table 2. Statistical significance was not able to be calculated for this group. There were no reoperations or complications in the study group.
Physical Examination Results at 5 Months a
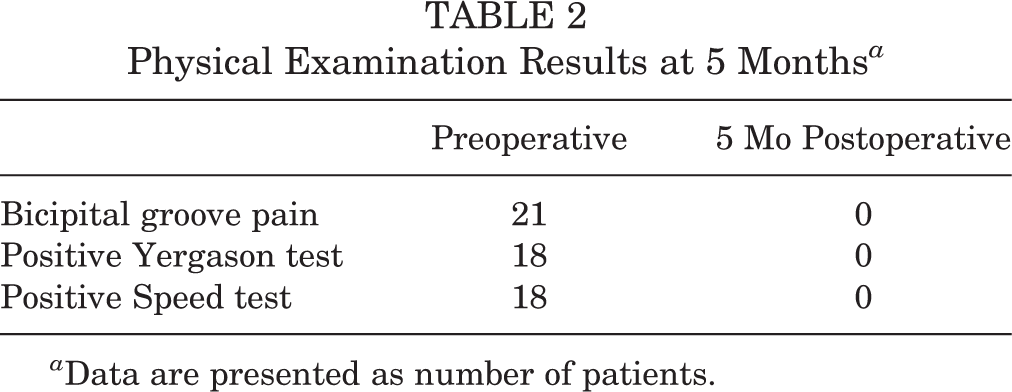
a Data are presented as number of patients.
Discussion
The most important finding of this study is that the technique of incorporating biceps tenodesis into the rotator cuff repair is safe and effective. There were no clinically apparent ruptures of the LHB or need for revision. The low rate of biceps-related cramping and groove pain demonstrates the effectiveness of the technique. Four patients reported a change in arm contour at 2 years. Of these 4 patients, 1 also reported cramping arm pain and loss of elbow strength, while another patient reported only loss of elbow strength. The change in contour is potentially secondary to lengthening the muscle tendon unit (see below) but could represent late rupture.
This arthroscopic technique of combining biceps tenodesis with rotator cuff repair has several advantages over other techniques. First, this technique is more cost-effective than most other techniques because the tenodesis does not require additional implants. Second, it can be performed with a single- or double-row rotator cuff repair. Third, it avoids potential risks of an open distal incision, including cosmesis concerns, stress riser–induced humerus fracture, infection, and neurovascular injury. A disadvantage is that this biceps tenodesis technique cannot be used without a concomitant supraspinatus repair.
There are 2 theoretical explanations for the successful pain relief and restoration of function in the presence of biceps groove pathology. First, in comparison with subpectoral biceps tenodesis, in which all pathological proximal biceps tissue is excised, this suprapectoral biceps tenodesis does not excise the groove pathology. This proximal rotator cuff repair incorporating the biceps tenodesis technique intentionally lengthens the LHB musculotendinous unit, thereby unloading it relative to the short head of the biceps, but not so much as to create a Popeye deformity. Second, the technique also likely eliminates groove pain from distal biceps pathology by eliminating the sliding motion of the LHB in the groove and allowing it to “scar down” into the bicipital groove. Anecdotally, the senior author has observed appropriate stability in the groove in instances in which a shoulder arthroplasty has been performed in these patients.
Checchia et al 2 reported the results of a similar arthroscopic biceps tenodesis incorporated into a supraspinatus tendon repair technique. The case series reported the outcome of 15 patients, of which 11 had an excellent outcome, 3 a good outcome, and 1 an unsatisfactory outcome according to University of California, Los Angeles (UCLA) shoulder scores at 32 months. One Popeye deformity was reported. The only biceps-specific outcome was the presence or absence of a Popeye deformity. One advantage of our series is the expanded biceps-specific questions. Our series had 4 changes in arm contour compared with 1 Popeye deformity in their series. A technique paper utilizing a similar arthroscopic biceps tenodesis incorporated into a supraspinatus tendon repair was published by George. 7 No outcomes were reported.
DeVito et al 6 performed a retrospective case-control study comparing biceps tenodesis techniques in patients with concomitant rotator cuff repairs. Techniques involved anchor fixation in the bicipital groove versus inclusion of the tenodesis in the most anterior anchor of the lateral row of the rotator cuff repair. There were no significant differences between the groups, but no biceps-specific outcomes were reported. The technique in our series has the advantage over this lateral-row technique of not requiring a double-row repair.
Brady et al 1 retrospectively reviewed an arthroscopic technique utilizing an interference screw proximal to the bicipital groove. This multicenter study of 1083 patients revealed an overall revision rate of 4.1% and a revision rate for biceps tenodesis–specific concerns of 0.4%. A total of 915 patients (84.5%) had concomitant rotator cuff repairs. VAS pain scores decreased from 6.47 to 1.08. UCLA shoulder scores improved from 14.9 to 30.1, and Simple Shoulder Test scores improved from 2.7 to 10.2. This study demonstrated a low revision rate and good outcome score improvement with a biceps tenodesis performed above the groove.
Sanders et al 21 retrospectively compared biceps tenodesis locations as well as techniques with or without release of the transverse humeral ligament. Tenodesis techniques above the groove had a significantly higher revision rate (20.6%) compared with tenodesis below the groove rate of (7.7%). Techniques that released the transverse humeral ligament had a significantly lower revision rate (6.8%) compared with techniques that did not release the ligament (20.6%).
Cho et al 4 performed a retrospective comparison of LHB tenotomy versus all arthroscopic intracuff tenodesis. In the tenodesis group, the LHB was sutured to the supraspinatius tendon but not tied into an anchor as in our study. There were no significant differences between the 2 groups. A total of 26.8% of the patients who had a tenotomy had a Popeye deformity compared with 16.7% of the patients who had tenodesis, which trended toward but did not reach statistical significance.
Patzer et al 18 performed a biomechanical cadaveric study comparing the load to failure for different biceps tenodesis techniques. The load to failure for anchors was about 50% of the interference screw load to failure. There was no load-to-failure difference between suprapectoral or subpectoral locations.
Limitations
There are several weaknesses associated with this study. First, it is a case series without a comparison group. Second, the number of patients is relatively small. Third, the patients had concomitant rotator cuff repairs, and it is difficult to discern how much improvement is attributable to the rotator cuff repair versus the biceps tenodesis. Fourth, objective data were collected for only 5 months. Fifth, 13 patients were lost to follow-up, creating the possibility of transfer bias. Finally, there were no follow-up ultrasounds, magnetic resonance imaging, or second-look surgeries to confirm healed rotator cuff and biceps tendons.
Conclusion
Arthroscopic biceps tenodesis incorporated into a supraspinatus tendon repair was a safe, reliable, and cost-effective option for biceps pathology with a concomitant rotator cuff tear.
Footnotes
Final revision submitted August 21, 2020; accepted September 30, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.M.V. has received education payments from Medwest. A.G.G. has received education payments from Arthrex, DJO, and Medwest; consulting fees from Smith & Nephew; and speaking fees from Arthrex, Ossur, and Smith & Nephew. C.W.U. has received education payments from Medwest, consulting fees from Stryker, and nonconsulting fees from Arthrex, and has stock/stock options in Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Borgess Medical Center (reference No. 2014-1372).