
Abstract
Background:
The posterior meniscofemoral ligament (pMFL) of Wrisberg attaches to the posterior horn of the lateral meniscus and the lateral intercondylar aspect of the medial femoral condyle and passes posteriorly to the posterior cruciate ligament (PCL). The pMFL plays a role in recovery after PCL injuries and offers stability to the lateral meniscus, promoting normal knee function.
Purpose/Hypothesis:
The aim of the magnetic resonance imaging (MRI) arm of this study was to evaluate the prevalence of the pMFL in Polish patients. The purpose of the systematic review and meta-analysis was to evaluate the clinical relevance of the pMFL in knee surgery. It was hypothesized that extensive variability exists in reports on the prevalence, function, and clinical significance of the pMFL.
Study Design:
Cross-sectional study and systematic review; Level of evidence, 3.
Methods:
A retrospective MRI investigation was conducted on 100 randomly selected lower limbs of Polish patients (56 male, 44 female) performed in 2019 to determine the prevalence of the pMFL. Additionally, an extensive literature search of major online databases was performed to evaluate all reported data on the pMFL. Assessments of article eligibility and data extraction were completed independently by 2 reviewers, and all disagreements were resolved via a consensus. A quality assessment of the included articles was performed using the Anatomical Quality Assessment tool.
Results:
In the MRI arm of this study, the pMFL was observed in 73 of the 100 limbs. In the meta-analysis, 47 studies were included, totaling 4940 lower limbs. The pooled prevalence of the pMFL was found to be 70.4% (95% CI, 63.4%-76.9%); the mean length was 27.7 mm (95% CI, 24.8-30.5 mm) and the mean widths were 4.5, 6.1, and 4.1 mm for the meniscal and femoral attachments and midportion, respectively. The mean pMFL thickness was 2.3 mm (95% CI, 1.8-2.7 mm).
Conclusion:
Despite the variability in the literature, the pMFL was found to be a prevalent and large anatomic structure in the knee joint. The shared features of this ligament with the PCL necessitate the consideration of its value in planning and performing arthroscopic procedures of the knee.
Keywords
The posterior meniscofemoral ligament (pMFL) of Wrisberg (Figures 1 and 2) attaches to the posterior horn of the lateral meniscus and the lateral intercondylar aspect of the medial femoral condyle and passes posteriorly to the posterior cruciate ligament (PCL). ** While initially considered a vestigial structure, efforts have been made in recent years to quantify the prevalence of the pMFL and to describe its morphometry and biomechanics. 5,7,31,32,69 Studies have reported that the pMFL (when present) plays a role in recovery after PCL injury by supporting and protecting the injured ligament; it also provides stability to the lateral meniscus, and because of its cooperation with the anterior meniscofemoral ligament (aMFL) of Humphrey, supports normal knee function. 5,7,32,69

The posterior meniscofemoral ligament (pMFL) of Wrisberg in a right knee. (A) Posterior view of the knee joint (the pMFL highlighted with red and marked with black arrow). (B) Coronal magnetic resonance imaging scan of the knee joint. PCL, posterior cruciate ligament; PHLM, posterior horn of the lateral meniscus (the pMFL marked with white arrow).
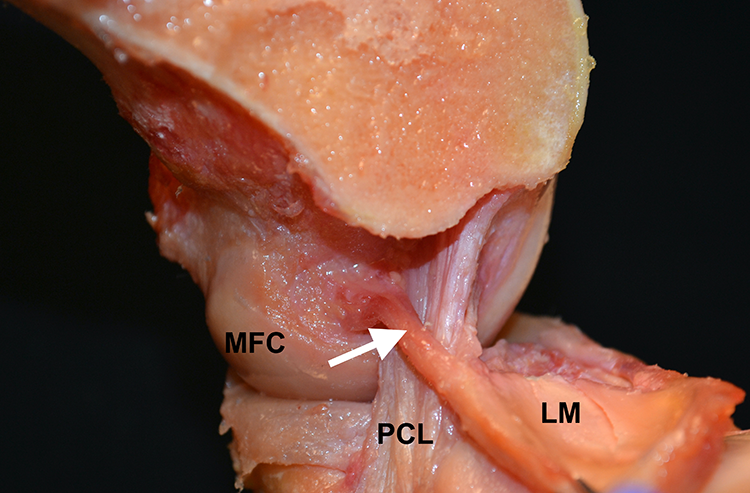
Cadaveric specimen of a right knee with the femur midsagittally resected, the lateral femoral condyle removed, and the posterior meniscofemoral ligament of Wrisberg (arrow) attached to the lateral meniscus (LM) and passing posteriorly to the posterior cruciate ligament (PCL). MFC, medial femoral condyle.
Nevertheless, many discrepancies in the characterization of the pMFL still exist, especially in terms of the structure’s prevalence, biomechanical function, and clinical relevance. 32,37,49,60,69,74 As there are currently no studies on the prevalence of the pMFL in the Polish population, we decided to conduct a magnetic resonance imaging (MRI) investigation addressing this issue. Moreover, understanding the anatomic and biomechanical properties of the pMFL may help to identify the ligament in imaging studies and during arthroscopic surgery, thus improving navigation and orientation (Figure 3). Therefore, we also aimed to systematically review the pMFL anatomy and its clinical relevance in knee surgery. We hypothesized that extensive variability exists in reports on the prevalence, function, and clinical significance of the pMFL.

Left knee viewed from the anterolateral arthroscopic portal with the posterior meniscofemoral ligament of Wrisberg visible (arrow).
Methods
MRI Study
A retrospective analysis of 100 (56 male, 44 female; mean age, 41.5 ± 13.8 years) randomly selected lower limb MRI scans performed in 2019 61 was completed by 2 of the researchers (P.A.P. and W.W.) with experience in musculoskeletal imaging. A consensus method was utilized to resolve any discrepancies in the evaluation. Patients had been referred for MRI to evaluate the cause of chronic knee pain. All patients were Polish. The MRIs were obtained on 3.0-T scanners with a dedicated 16-channel knee coil in the standard extended position; see Appendix Table A1 for MRI parameters. The patient inclusion criteria for this section of the study were as follows: (1) age older than 18 years, (2) no acute knee trauma, (3) no limb deformities and/or anomalies, and (4) no history of knee surgery. This study was approved by the ethics committee of our institution.
Chi-square tests were performed to evaluate significant (P < .05) differences among subgroups. Calculations were conducted using SPSS Version 25 (IBM).
Systematic Review and Meta-analysis
Search Strategy
The protocol of this meta-analysis was registered in the PROSPERO database (CRD42020185088). A comprehensive search of relevant online databases (PubMed, Embase, ScienceDirect, Web of Science, and Google Scholar) was conducted for publications up to April 2020 to accumulate reported data on the pMFL. The following search terms were employed: “posterior meniscofemoral ligament OR Wrisberg ligament OR ligamentum meniscofemorale posterius OR ligamentum Wrisberg OR anterior meniscofemoral ligament OR Humphrey ligament OR ligamentum meniscofemorale anterius OR ligamentum Humphry OR amfl OR pmfl.” No date or language restrictions were imposed. After the initial search, every associated reference list was also considered for inclusion. The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines 42 were carefully followed.
Eligibility Assessment
Articles were independently assessed for their relevance by 2 authors (P.A.P. and M.A.R.). The following inclusion criteria were utilized: (1) studies with complete and unambiguous data on the pMFL prevalence and/or morphometrics; (2) cadaveric, MRI, or arthroscopic investigations; and (3) studies performed on ≥5 lower limbs. Criteria for exclusion were as follows: (1) conference abstracts, case reports, book reviews, review articles, and letters to the editor; (2) overlapping, incomplete, or nonextractable data; (3) nonhuman studies; and (4) fetal studies. In the morphometric analyses, only the studies performed on adult specimens were included. All article languages were considered; any non-English reports were translated by medical professionals fluent in the original language of the publication as well as English.
Data Extraction
Two of the authors (P.A.P. and D.P.Ł.) independently extracted all available relevant data on the pMFL from the included studies. All inconsistencies in this independent extraction were solved via a consensus among the reviewers, with the involvement of the original study authors when necessary and possible.
Bias Assessment
The Anatomical Quality Assessment (AQUA) tool 41 was used to assess the quality and potential for bias of the studies included in the meta-analysis. Each study was assessed on the following 5 domains as having a low, high, or unclear risk of bias: (1) participant characteristics and objectives, (2) study design, (3) characterization of methods, (4) descriptive anatomy, and (5) reporting of results.
Statistical Analysis
A statistical analysis was conducted to compute the pooled prevalence utilizing MetaXL 5.3 (EpiGear) 42 ; morphometric calculations were performed using Comprehensive Meta-Analysis 3.0 (Biostat) (random-effects model). The chi-square test and I 2 statistic were utilized to assess the heterogeneity of the included studies. A Cochran Q with P < .10 indicated significant heterogeneity. The I 2 statistic was interpreted according to the following criteria: 0%-40%, may not be important; 30%-60%, may indicate moderate heterogeneity; 50%-90%, may indicate substantial heterogeneity; and 75%-100%, may represent considerable heterogeneity. 43 Extensive subgroup analyses (modality, geographic origin, sex, and side) were performed to identify the sources of heterogeneity. In addition, a sensitivity analysis of studies performed on ≥100 lower limbs was conducted. Statistically significant differences were determined using confidence intervals; any overlap between the confidence intervals was suggestive of non-significant differences.
Results
MRI Study
The pMFL was identified in 73 of the 100 limbs assessed via MRI. No significant differences were observed among the subgroups (Table 1).
MRI-Based Prevalence of the Posterior Meniscofemoral Ligament a

a No significant differences were observed among the analyzed subgroups (P > .05 for all). MRI, magnetic resonance imaging.
Meta-analysis
Study Identification and Characterization
Overall, 44 articles (46 studies, with 2 articles describing 2 modalities) and our MRI study were included in this meta-analysis, with a total of 4940 lower limbs (Appendix Table A2 and Figure 4). There were 17 studies from Europe, 14 from Asia, 12 from North America, and 4 from South America. Additionally, 2 studies were purely arthroscopic, 32 were cadaveric, and 13 were radiological. One study 16 did not report the pMFL prevalence, and only relevant morphometric data were included. During the eligibility assessment, studies with equivocal data were identified and excluded from the quantitative analysis.
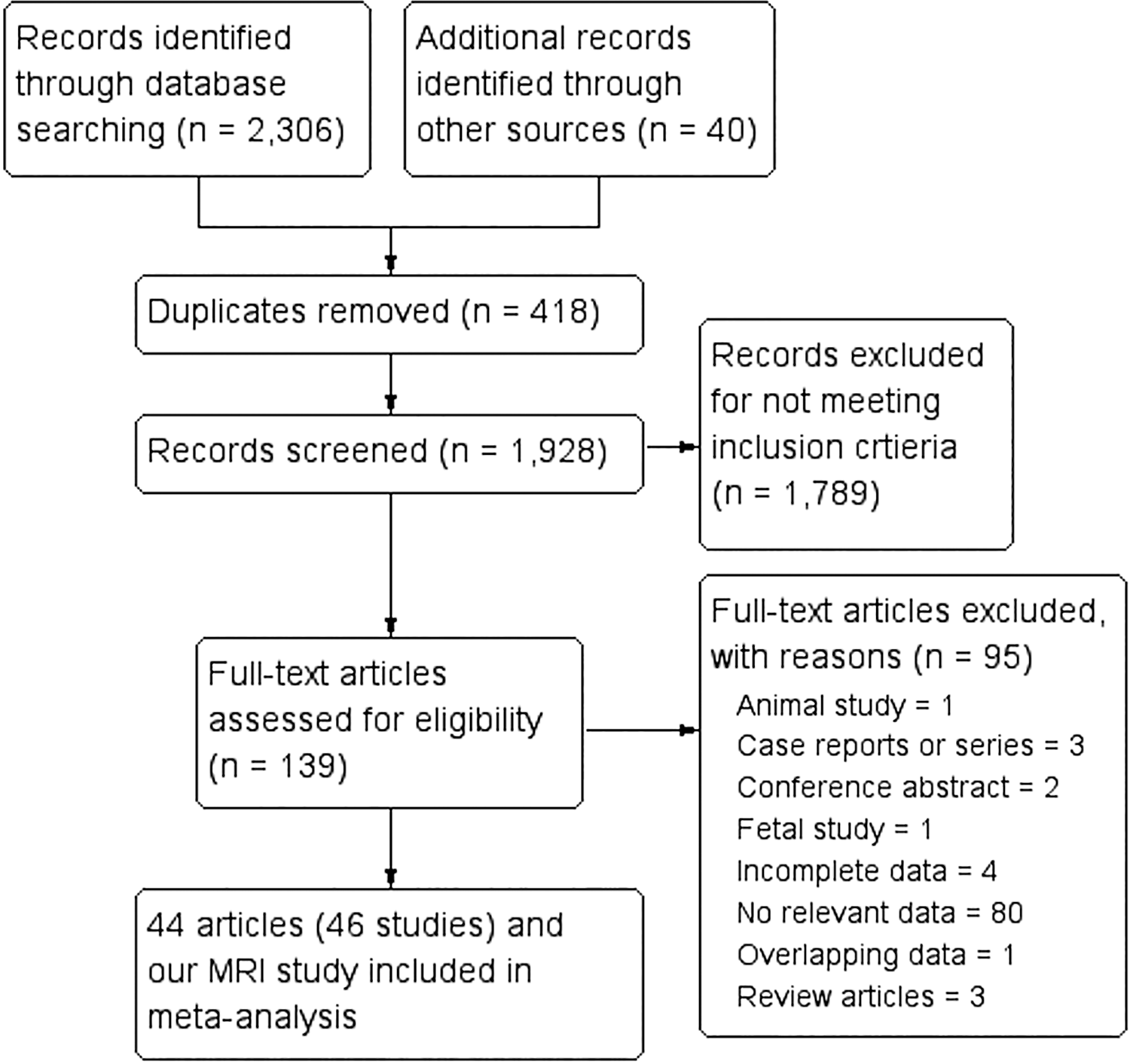
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart of study identification, evaluation, and inclusion into the meta-analysis. MRI, magnetic resonance imaging.
Bias Assessment
Results of the assessment of heterogeneity and bias within the included studies are shown in Appendix Table A3 and Appendix Figure A1. In 4 of the AQUA domains (participant characteristics and objective(s), study design, descriptive anatomy, and reporting of results), the risk was evaluated as low, with only a few exceptions. The high-risk sources of bias primarily pertained to 1 domain (methodology characterization), which has previously been identified as a source of variability. 11,32
Prevalence of the pMFL
Overall, 46 studies (4910 lower limbs) reported the pMFL prevalence (pooled prevalence: 70.4% [95% CI, 63.4%-76.9%]) (Table 2 and Figure 5). The pMFL was more frequently identified in cadaveric studies (74.1% [95% CI, 67.2%-80.5%]) compared with arthroscopic studies (41.1% [95% CI, 0.0%-100.0%]). The prevalence of the pMFL among MRI studies was 66.5% (95% CI, 52.7%-79.1%). Studies from Asia presented the highest prevalence (81.6% [95% CI, 74.6%-87.7%) and North America the lowest (55.5% [95% CI, 44.0%-66.6%]) (Table 2).
Prevalence of the Posterior Meniscofemoral Ligament by Study Type, MRI Strength, and Geographic Region a

a MRI, magnetic resonance imaging.
b 3.0 T and <1.5T MRI subgroups are not the only parts of the Radiological subgroup (there are 2 studies performed using more than one scanner

Forest plot for the overall pooled prevalence of the posterior meniscofemoral ligament of Wrisberg.
The pMFL prevalence was slightly higher in male patients than in female patients (78.2% vs 77.7%, respectively) (Table 3), and the pMFL was more often found on the right side than the left side (72.3% vs 68.7%, respectively) (Table 4). However, these differences were not statistically significant.
Prevalence of the Posterior Meniscofemoral Ligament in Relation to Sex

Prevalence of the Posterior Meniscofemoral Ligament With Respect to Side

Pooling of pMFL Morphometric Data
The pMFL was a pooled mean length of 27.7 mm (95% CI, 24.8-30.5 mm) (Table 5). The width of the pMFL ranged from 4.1 mm (95% CI, 3.6-4.5 mm) to 6.1 mm (95% CI, 5.1-7.1 mm), depending on the level of the measurement (Table 5). Its overall thickness was reported to be 2.3 mm (95% CI, 1.8-2.7 mm) (Table 5). The pMFL:PCL cross-sectional area ratio was 14.1% (95% CI, 10.2%-17.9%) (Table 6).
Morphometric Analysis of the Posterior Meniscofemoral Ligament

Analysis of the Cross-sectional Areas of the pMFL a

a PCL, posterior cruciate ligament; pMFL, posterior meniscofemoral ligament.
Discussion
The primary findings of this study demonstrated that the pMFL was a large (length: 27.7 mm; midportion width: 4.1 mm; thickness: 2.3 mm) and prevalent (70.4%) structure, suggesting a significant biomechanical role and necessitating an increased awareness of its presence during arthroscopic procedures (Figure 3). The pMFL was most commonly reported in cadaveric studies (74.1%) likely because of the superior visualization of this method. Noteworthy is the fact that comparable, albeit slightly lower, results were obtained via MRI (66.5%) and arthroscopic (41.1%) studies, confirming that available clinical diagnostic methods are of significant benefit to physicians. The results of this meta-analysis are supported by findings of the MRI arm of our study, which showed a pMFL prevalence of 73.0% in the studied population.
Our meta-analysis reported a higher pMFL prevalence in studies using 3.0-T MRI scanners compared with those with a magnetic strength ≤1.5 T. Such results are supported by Ebrecht et al, 19 who suggested that 3.0-T MRI is especially valuable in clearly depicting the anatomy of the pMFL, including its different attachments on the femoral condyle. Physicians should be made aware that visualization of the MFLs is challenging because they can be mistaken for meniscal tears or rare anatomic variants, such as ring-shaped lateral menisci. 21
Since its identification, this ligament has continued to demonstrate function beyond anteroposterior passive resistance and rotatory laxity. 4,26 Such a hypothesis is supported by reports that the presence of the pMFL correlates with a smaller PCL cross-sectional area. 7,69
One should remember that in the case of tears of the posterior root of the lateral meniscus, in contrast to the medial meniscus, the lateral root may have an additional attachment to the femur via the MFLs. 22 Therefore, while posterior root tears of the medial meniscus are reported to be comparable with total medial meniscectomy in terms of functional decline, observed as increased contact pressure in the medial compartment of the knee, in the case of lateral meniscal tears, such a situation is observed only when both the posterior root attachment of the lateral meniscus and MFLs are damaged. 3,22,23
Moreover, the pMFL, together with the aMFL, has been shown to maintain tension on the posterior horn of the lateral meniscus. This tensioning function of the MFLs facilitates the optimal contact area between the lateral meniscus, tibial plateau, and lateral femoral condyle. 4,26 Noteworthy is the fact that the prevalence of extrusion of the lateral meniscus after a tear of its posterior root was observed to be significantly lower when the MFLs were anchoring the posterior root. 13 An intact pMFL has also been reported to prevent lateral meniscal extrusion when its posterior root is damaged in mathematical models. 8 Therefore, acting as a modulator of tibiofemoral pressure, the pMFL may prevent early degenerative changes in the knee joint. 6,22,26
A biomechanical study has also confirmed the cooperative function between the lateral meniscus posterior root and MFLs, in which in situ resection of these structures significantly increased valgus flexion angles. 56 Furthermore, the forces on the MFLs and lateral meniscus posterior root changed reciprocally throughout knee flexion; resection of MFLs significantly decreased the forces generated by the lateral meniscus. Therefore, in the case of posterior lateral meniscal detachment, clinicians must repair it and attempt to preserve the MFLs because they may produce additional stability and thus secure the restored root attachment. Such an approach preserves natural meniscal function and may improve joint stability, therefore improving clinical outcomes. 56 However, there is no established method to repair or reconstruct the pMFL.
Trauma to the posterior horn of the lateral meniscus often occurs with a torn anterior cruciate ligament (ACL). 18,59,73 Importantly, injuries to these 2 elements frequently present with bone bruising of the lateral femoral condyle and an impression fracture of the posterior tibial plateau. 9,10,23 In such a situation, it is necessary to perform ACL reconstruction with lateral meniscus root repair to maintain normal knee biomechanics. 26 Additionally, it has been reported that in cases with an unstable posterior root attachment of the lateral meniscus, the ACL graft is subjected to increased forces, which may lead to reconstruction graft overload and failure. 24,26,72
Interestingly, Pula et al 63 reported no difference in lateral meniscal extrusion rates between patients with isolated ACL tears and patients with ACL and lateral meniscus posterior root tears. It is noteworthy that all included patients had MFLs, which could have stabilized the lateral meniscus and prevented measurable extrusion. The main limitation of that study was the lack of a group with torn or absent MFLs 63 ; further studies will be needed to address this.
In the case of a discoid meniscus with an abnormally short and thick pMFL (“Wrisberg ligament type”) that has no posterior tibial attachment, its normal mobility can be altered. Such a variant can cause locking or snapping of the knee joint as a hypermobile posterior root is pulled into the intercondylar notch. 44
The supportive functions of the pMFL are highlighted in the case of a PCL tear in which this ligament may avoid tearing because it is attached to the mobile lateral meniscus and can then maintain improved knee stability, despite an inefficient PCL. 34,68 For instance, an intact pMFL was demonstrated to reduce posterior drawer in the case of a PCL tear, possibly acting as a passive secondary restraint or through a neurosensory feedback loop. 32,33,34,68 Moreover, the pMFL can have a supporting role in PCL healing and shows features of posttraumatic hypertrophy. 30 Interestingly, in the history of arthroscopic surgery, this ligament may have been viewed as unnecessary tissue that impeded procedures and was frequently removed. 7 Animal studies have emphasized the significant role of the pMFL as an important secondary restraint to posterior translation of the tibia. 51 Together, the available data suggest that the best results of PCL reconstruction may be obtained when the pMFL is preserved. However, more studies are needed to fully evaluate this issue.
Given the significance of the pMFL in PCL injury management, Ebrecht et al 19 established a classification system to provide more effective surgical guidelines: type I indicated the absence of the pMFL, either without any oblique fibers (Ia) or with PCL-like fibers inserting at the femur but fixating to the tibia and not the lateral meniscus (Ib). Type II indicated the presence of the pMFL, subdivided as having an insertion in the upper third of the medial femur (IIa), middle third (IIb), or lower third (IIc). This classification may possess clinical relevance, as demonstrated by Ahn et al, 2 who reported that symptomatic patients presenting with a posterocentrally shifted discoid lateral meniscus tended to have a significantly thicker pMFL with a higher femoral attachment. Furthermore, inadequate identification of this ligament may propagate false diagnoses, such as meniscal tears, especially by younger surgeons. 55 For this reason, it is important to develop a complete anatomic understanding of the region, especially considering possible gap sizes or partial volume effects, which may obscure a small pMFL on MRI. 69
This study was predominantly limited by the lack of methodology characterization among the studies reviewed, a factor that was classified as a source of bias. However, it is important to acknowledge that anatomic studies performed using various methodologies provide findings subject to less bias than clinical studies, which may have an inherent bias related to the study design or the intentions of the researchers. Moreover, extensive subgroup analyses were performed to reduce bias related to various modalities among the included studies.
Conclusion
Despite the variability in the published literature, the pMFL was a highly prevalent and large anatomic structure in the knee joint. The shared features of this ligament with the PCL were highlighted to necessitate the consideration of its value in planning and performing arthroscopic procedures of the knee.
Footnotes
Final revision submitted September 14, 2020; accepted October 9, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.G. has received consulting fees from Anika Therapeutics. R.F.L. has received research support from Smith & Nephew; consulting fees from Arthrex, Ossur, Smith & Nephew, and Linvatec; and royalties from Arthrex, Ossur, and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto. Ethical approval for this study was obtained from Jagiellonian University Medical College. This project was funded using the statutory funds of the Jagiellonian University Medical College.
Acknowledgment
The authors acknowledge Ewa Mizia, MD, PhD for her support and consultation throughout the study.
Notes
Appendix
Risk of Bias of the Included Studies According to the AQUA Checklist a
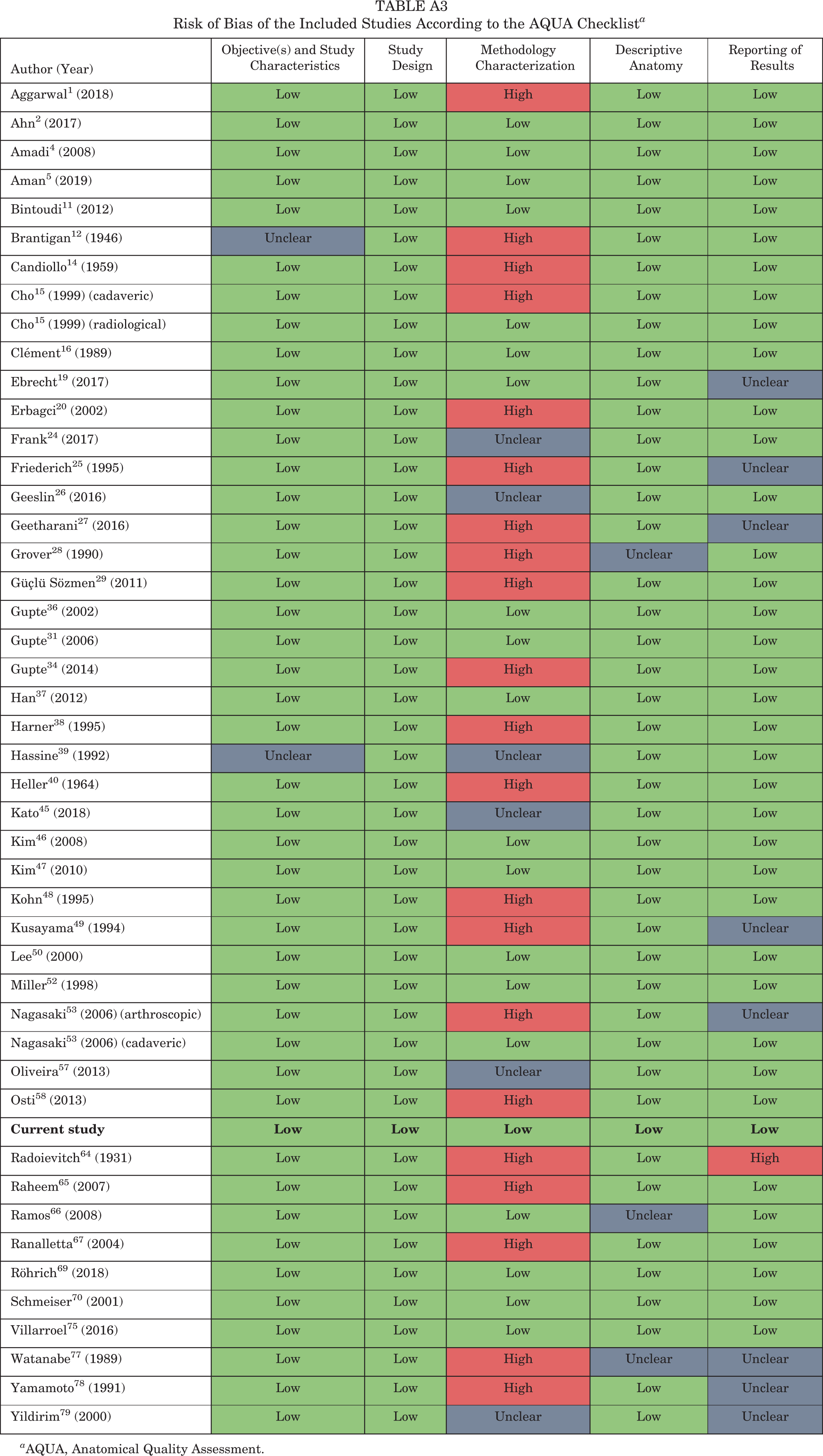
| Author (Year) | Objective(s) and Study Characteristics | Study Design | Methodology Characterization | Descriptive Anatomy | Reporting of Results |
| Aggarwal 1 (2018) | Low | Low | High | Low | Low |
| Ahn 2 (2017) | Low | Low | Low | Low | Low |
| Amadi 4 (2008) | Low | Low | Low | Low | Low |
| Aman 5 (2019) | Low | Low | Low | Low | Low |
| Bintoudi 11 (2012) | Low | Low | Low | Low | Low |
| Brantigan 12 (1946) | Unclear | Low | High | Low | Low |
| Candiollo 14 (1959) | Low | Low | High | Low | Low |
| Cho 15 (1999) (cadaveric) | Low | Low | High | Low | Low |
| Cho 15 (1999) (radiological) | Low | Low | Low | Low | Low |
| Clément 16 (1989) | Low | Low | Low | Low | Low |
| Ebrecht 19 (2017) | Low | Low | Low | Low | Unclear |
| Erbagci 20 (2002) | Low | Low | High | Low | Low |
| Frank 24 (2017) | Low | Low | Unclear | Low | Low |
| Friederich 25 (1995) | Low | Low | High | Low | Unclear |
| Geeslin 26 (2016) | Low | Low | Unclear | Low | Low |
| Geetharani 27 (2016) | Low | Low | High | Low | Unclear |
| Grover 28 (1990) | Low | Low | High | Unclear | Low |
| Güçlü Sözmen 29 (2011) | Low | Low | High | Low | Low |
| Gupte 36 (2002) | Low | Low | Low | Low | Low |
| Gupte 31 (2006) | Low | Low | Low | Low | Low |
| Gupte 34 (2014) | Low | Low | High | Low | Low |
| Han 37 (2012) | Low | Low | Low | Low | Low |
| Harner 38 (1995) | Low | Low | High | Low | Low |
| Hassine 39 (1992) | Unclear | Low | Unclear | Low | Low |
| Heller 40 (1964) | Low | Low | High | Low | Low |
| Kato 45 (2018) | Low | Low | Unclear | Low | Low |
| Kim 46 (2008) | Low | Low | Low | Low | Low |
| Kim 47 (2010) | Low | Low | Low | Low | Low |
| Kohn 48 (1995) | Low | Low | High | Low | Low |
| Kusayama 49 (1994) | Low | Low | High | Low | Unclear |
| Lee 50 (2000) | Low | Low | Low | Low | Low |
| Miller 52 (1998) | Low | Low | Low | Low | Low |
| Nagasaki 53 (2006) (arthroscopic) | Low | Low | High | Low | Unclear |
| Nagasaki 53 (2006) (cadaveric) | Low | Low | Low | Low | Low |
| Oliveira 57 (2013) | Low | Low | Unclear | Low | Low |
| Osti 58 (2013) | Low | Low | High | Low | Low |
|
|
|
|
|
|
|
| Radoievitch 64 (1931) | Low | Low | High | Low | High |
| Raheem 65 (2007) | Low | Low | High | Low | Low |
| Ramos 66 (2008) | Low | Low | Low | Unclear | Low |
| Ranalletta 67 (2004) | Low | Low | High | Low | Low |
| Röhrich 69 (2018) | Low | Low | Low | Low | Low |
| Schmeiser 70 (2001) | Low | Low | Low | Low | Low |
| Villarroel 75 (2016) | Low | Low | Low | Low | Low |
| Watanabe 77 (1989) | Low | Low | High | Unclear | Unclear |
| Yamamoto 78 (1991) | Low | Low | High | Low | Unclear |
| Yildirim 79 (2000) | Low | Low | Unclear | Low | Unclear |
a AQUA, Anatomical Quality Assessment.