
Abstract
Background:
Shoulder and elbow injuries are major problems in baseball players. Tightness of the upper extremities has been reported as a risk factor for shoulder and elbow injuries in elementary and junior high school baseball players. However, few studies have been conducted on the relationship between decreased hip range of motion (ROM) and shoulder and elbow injuries.
Purpose/Hypothesis:
This study aimed to prospectively examine the relationship between hip ROM and throwing-related shoulder and elbow injuries in elementary and junior high school baseball players. The hypothesis was that players with unrestricted ROM in the hip would have a reduced risk of upper extremity injuries.
Methods:
The study included 263 baseball players (mean ± SD age, 10.5 ± 1.3 years; range, 7-14 years). The following physical parameters were assessed: (1) hip flexion ROM measured in the supine position and (2) hip internal and external rotation in the prone position. After the season, players completed questionnaires regarding shoulder and/or elbow injuries. For comparison, the players were classified as injured (not able to play for ≥8 days because of shoulder and/or elbow problems) or noninjured.
Results:
During the season, 52 players had shoulder and/or elbow injuries. When the injured and noninjured groups were compared, hip flexion on the dominant side (121.5° ± 12.0° vs 126.7° ± 9.8°, respectively; P < .01), hip flexion on the nondominant side (119.6° ± 11.7° vs 126.0° ± 9.9°, respectively; P < .01), and internal rotation on the dominant side (52.5° ± 11.3° vs 56.8° ± 10.8°, respectively; P = .01) were significantly reduced in the injured group.
Conclusion:
We identified preseason decreases in flexion bilaterally and internal rotation on the dominant side as risk factors for shoulder and elbow injuries in elementary and junior high school baseball players. Further studies are required to prevent disabilities in elementary and junior high school baseball players through development of prevention and intervention programs.
Shoulder and elbow injuries are major problems in baseball players. 5,12,21 Previous studies have shown that 30% of elementary school baseball players experience injuries during a season. 12 Other prospective studies have reported risk factors for shoulder and elbow injuries including elbow varus and shoulder external rotation (ER) torque (at peak external shoulder rotation during pitching), 1 high pitch velocity, 2 glenohumeral internal rotation (IR) deficit, shoulder ER insufficiency, 23 deficits in preseason supraspinatus, prone ER strength, 3 and imbalance in muscle strength around the shoulder. 14 The significant risk factors specifically for elbow injury include a history of elbow pain, 13 being a pitcher or catcher, 13 pitching >100 innings in 1 year, 7 training >16 h/wk, 13 and posterior shoulder tightness. 18,22 Comprehensive evidence is available regarding upper limb parameters that are risk factors for shoulder and elbow injuries. However, limited evidence is available regarding lower limb characteristics that serve as risk factors for shoulder and elbow injuries. Furthermore, the existing prospective studies about lower limb risk factors have evaluated junior high school students, 6 but none have included elementary school students. Therefore, this study aimed to prospectively investigate the relationship between hip range of motion (ROM) and the incidence of shoulder and elbow injuries in elementary and junior high school baseball players. We hypothesized that players with unrestricted ROM in the hip would have a reduced risk of upper extremity injuries.
Methods
Study Design and Participants
The study enrolled young baseball players belonging to the Gunma Prefecture Elementary and Junior High School Baseball Federation who participated in medical check-ups held in February 2018 and February 2019 at our institution. The study was approved by an institutional review board; all methods were conducted following the relevant guidelines and regulations, and informed consent was obtained from all players and their parents.
In accordance with a previous study, 19 players were included if they (1) participated in preseason workouts as active players, (2) had no restrictions on baseball activities, and (3) participated in medical check-ups in both 2018 and 2019; players were excluded if they had (1) previous injuries to the throwing arm or (2) an inability to throw or restricted throwing activity due to a shoulder or elbow problem. Players who participated in the check-ups in both 2018 and 2019 were surveyed during the 2019 check-ups as to whether they had sustained a shoulder or elbow injury during the 2018 season (Figure 1). The questionnaire about shoulder or elbow injuries was completed by the players themselves and their parents or coaches (Appendix). A shoulder or elbow injury was defined as any shoulder or elbow condition that resulted in players being considered disabled for ≥8 days. 16,19,20 Based on their replies, players were categorized into injured and noninjured groups.

Flowchart of the players included in this study.
Medical Check-ups
The participants underwent a baseline medical examination that evaluated the preseason condition of their shoulders and elbows. At the check-ups, we questioned the participants about their age and dominant arm and measured their weight and height. Data on hip ROM were collected by 2 orthopaedic surgeons (N.H., H.S.) using a reliable and previously validated technique according to a previous study. 14 Using a digital protractor (iGaging), the examiners evaluated each player’s hip ROM in flexion, IR, and ER on both sides. The examiners were blinded to the participants’ hand dominance in order to avoid a confirmation bias.
Hip ROM Measurements
Flexion
Players were instructed to lie in a supine position. One examiner stabilized the pelvis of the player, while the other examiner flexed the player’s hip joint on the measurement side, keeping the knee on that side flexed. Notably, the contralateral limb was maintained in full extension.
Internal/External Rotation
Players were instructed to lie in a prone position. One examiner stabilized the athlete’s pelvis, while the other examiner bent the knee on the measurement side at 90° and rotated the hip joint internally and externally with 0° of flexion. The contralateral limb was maintained in full extension. The angles between the perpendicular and the lower leg were considered IR and ER, respectively.
Statistical Analysis
Baseline characteristics and the results of univariate analysis are reported as mean ± SD. All tests were 2-sided, with P < .05 considered significant. The analysis was performed using an independent t test for continuous variables to compare baseline characteristics between the groups. Multivariable logistic regression analysis, using variables with P < .1 in univariate analysis, was used to identify potential risk factors for elbow or shoulder injuries. Before performing a logistic regression analysis, we performed a Pearson correlation coefficient test to avoid multicollinearity. To identify the risk factors for shoulder and elbow injuries and to calculate odds ratios and 95% CIs, we performed a logistic regression analysis after adjusting for significant variables determined from univariate analyses. These analyses were performed using the IBM SPSS Statistics software program (Version 26; IBM Japan). A previous statistical power analysis for logistic regression indicated that a total of 70 participants would be needed to detect statistical significance depending on a statistical power of 80% at an α level of .05 (assumptive incidence rate, 20%; odds ratio, 2.5). 23
Results
A total of 387 players attended check-ups in 2018, of whom 263 returned in 2019. Of the 263 players (age, 10.5 ± 1.3 years; range, 7-14 years) who completed the questionnaire, 52 players (20%) had shoulder and elbow injuries during the season. Among the participants were 245 boys and 18 girls.
Univariate Analysis
Age, height, and weight in the injured group were significantly greater than those in the noninjured group. When the injured and noninjured groups were compared, hip flexion on the dominant side (121.5° ± 12.0° vs 126.7° ± 9.8°, respectively; P < .01), hip flexion on the nondominant side (119.6° ± 11.7° vs 126.0° ± 9.9°, respectively; P < .01), and IR on the dominant side (52.5° ± 11.3° vs 56.8° ± 10.8°, respectively; P = .01) were significantly reduced in the injured players (Table 1).
Comparison of Variables Between the Injured and Noninjured Groups a

a Data are reported as mean ± SD. Bolded P values indicate statistically significant between-group differences (P < .05). ROM, range of motion.
Multivariate Analysis
Among variables with P < .1 based on results of univariate analyses, height and weight were significantly correlated with age (P < .001; r, 0.810 and 0.746, respectively). Thus, height and weight were removed from the explanatory variables for the logistic model. A logistic regression analysis showed that older age (P < .01; odds ratio, 1.40) and decreased hip flexion ROM on the dominant side (P = .04; odds ratio, 0.94) were significantly associated with the incidence of injuries (Table 2).
Results of the Multivariate Analysis a
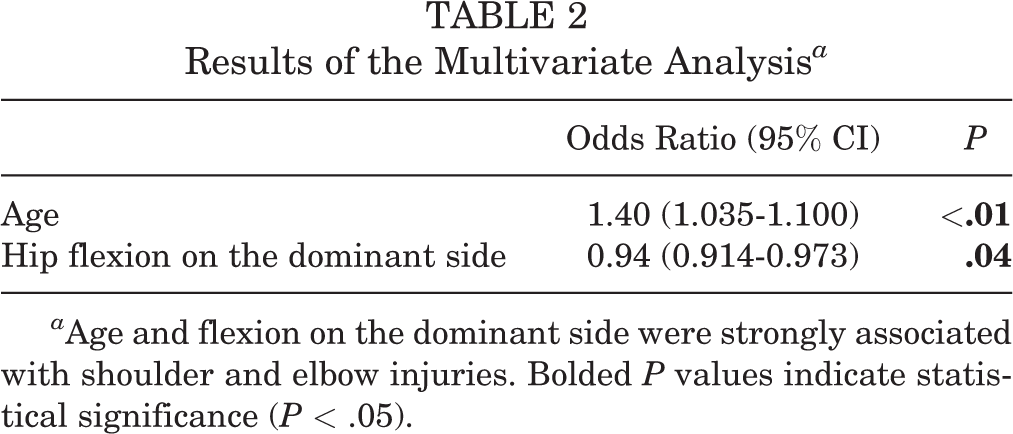
a Age and flexion on the dominant side were strongly associated with shoulder and elbow injuries. Bolded P values indicate statistical significance (P < .05).
Discussion
The main findings of this study were that older age and limitations in preseason hip flexion ROM were independent risk factors for shoulder and elbow injuries during the season. In addition, we found that greater height and weight, decreased hip flexion on the nondominant side, and decreased IR on the dominant side were significant risk factors for shoulder and elbow injuries. To the best of our knowledge, this is the first prospective study to provide evidence that a hip ROM deficit could affect shoulder and elbow injuries in elementary and junior high school baseball players.
Pitching-related shoulder disorders can occur when the kinetic chain generated from the lower limb is not smoothly performed. 8 –10 Davis et al 4 reported that opening the stepping leg more than usual increased the IR torque of the shoulder joint. A narrow step width resulted in unstable pitching form and abnormal trunk movement. 4 Furthermore, pitching is a total body movement, and the rotation movement of each body part becomes remarkable after the translation movement of the lower limb. Therefore, it was presumed that the load on the shoulder and elbow joints generated during pitching was affected by lower limb movement. 15 Li et al 11 reported that limitations in hip joint ROM led to problems associated with the kinetic chain. Saito et al 16 reported that the ROM of hip joint flexion and IR of the hip were less in patients with elbow pain on both sides than in patients without elbow pain. In a study of 57 professional baseball players, Scher et al 17 reported that the nondominant hip joint IR was less in athletes with than in athletes without a history of shoulder and elbow pain. The evidence from these studies is very important for protecting baseball players from preventable shoulder and elbow injuries; however, these studies have 2 limitations. First, they were cross-sectional studies. Therefore, it is unknown whether the decrease in hip joint ROM caused shoulder and elbow injuries or resulted from those injuries. Second, injury was defined as “whether or not you have noticed elbow tenderness during a medical examination or elbow pain during a pitch in the past month” 16 and “shoulder pain history.” 17 These definitions seem extremely restrictive for the investigation of risk factors.
In the current study, shoulder or elbow injury was defined as any condition resulting in the pitcher’s being considered disabled for ≥8 days; this definition has been applied in previous studies 15,19,20 and might be more meaningful for investigating risk factors. Endo and Sakamoto, 6 in a prospective study of 39 junior high school students, reported that hip ER in the nondominant side was significantly less before the season among participants with shoulder and elbow pain than in participants without this pain. However, those authors defined an injury as feeling pain in the midst of a pitching motion during the season, which is different from the criteria we used. They also defined the season as April through July, which means that baseball games and practices that took place after August were not considered. The baseball season generally runs from spring to fall, and a survey is best conducted after all baseball events have been completed. We determined injury incidence for the 1-year baseball season in a manner based on previous studies. 15,19,20
Previous studies have reported that the risk of arm injury among pitchers increases with age, height, and weight. 12,21 In a prospective study, Lyman et al 12 reported that age and weight were developmental risk factors for elbow injury in 9- to 12-year-old baseball players. Their hypothesis focused on the secondary ossification centers that are the most vulnerable points in the young elbow; these centers begin to ossify between the ages of 2 and 11 years and do not fuse to the long bones until as late as 17 years of age. 12 This may explain why the rate of throwing-related elbow injuries increases with age. A high body weight may place more burden on a pitcher’s immature skeleton, thereby exacerbating elbow weakness and resulting in an increased likelihood of elbow injury. Taller pitchers likely have longer arms, which weigh more than do shorter arms, resulting in more weight being maintained by the shoulder joint during pitching. 12 This creates a higher torque on the shoulder joint and could be the source of shoulder pain.
The current study had several limitations. First, we did not evaluate external load factors, such as total number of pitches and number of innings pitched. This should be examined in future studies. Second, we did not conduct imaging tests, such as radiography, computed tomography, or magnetic resonance imaging, to detect pathologic factors in the participants’ hip joints. Instead, this study relied on medical check-ups in order to avoid unnecessary radiation exposure. Third, the data about shoulder and elbow injuries were self-reported by the young participants and may have been subject to recall bias. Fourth, the relationship between the severity of injuries and amount of baseball load is unclear in this study because data on injury severity were not collected.
Conclusion
We observed that preseason decreases in bilateral flexion and dominant-side IR were risk factors for shoulder and elbow injuries in elementary and junior high school baseball players. In the future, we intend to prevent disabilities in elementary and junior high school baseball players by developing prevention and intervention programs.
Footnotes
Acknowledgment
The authors thank the personnel, players, coaches, and staff of the Gunma Prefecture High School Baseball Federation for their assistance and cooperation in this study.
Final revision submitted June 10, 2020; accepted July 1, 2020.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Gunma University Hospital (ref No. 1003 2015-01-28).
Authors
Noritaka Hamano, MD, PhD (Gunma University Graduate School of Medicine, Maebashi, Gunma, Japan); Hitoshi Shitara, MD, PhD (Gunma University Graduate School of Medicine, Maebashi, Gunma, Japan); Tsuyoshi Tajika, MD, PhD (Gunma University Graduate School of Medicine, Maebashi, Gunma, Japan); Takuro Kuboi, MD (Gunma University Graduate School of Medicine, Maebashi, Gunma, Japan); Tsuyoshi Ichinose, MD, PhD (Gunma University Graduate School of Medicine, Maebashi, Gunma, Japan); Tsuyoshi Sasaki, MD, PhD (Gunma University Graduate School of Medicine, Maebashi, Gunma, Japan); Takanori Kitagawa, MD, PhD (Gunma University Graduate School of Medicine, Maebashi, Gunma, Japan); Hiroki Kobayashi, MD (Gunma University Graduate School of Medicine, Maebashi, Gunma, Japan); Atsushi Yamamoto, MD, PhD (Gunma University Graduate School of Medicine, Maebashi, Gunma, Japan); Tsutomu Kobayashi, MD, PhD (Gunma University Graduate School of Medicine, Maebashi, Gunma, Japan); Kenji Takagishi, MD, PhD (Gunma University Graduate School of Medicine, Maebashi, Gunma, Japan); Hirotaka Chikuda, MD, PhD (Gunma University Graduate School of Medicine, Maebashi, Gunma, Japan); Fumitaka Endo, MD (Gunma University Graduate School of Medicine, Maebashi, Gunma, Japan); Masataka Kamiyama, MD (Gunma University Graduate School of Medicine, Maebashi, Gunma, Japan); Daisuke Shimoyama, MD (Gunma University Graduate School of Medicine, Maebashi, Gunma, Japan); Shuhei Takanime, MD (Gunma University Graduate School of Medicine, Maebashi, Gunma, Japan); Ryosuke Miyamoto, MD (Gunma University Graduate School of Medicine, Maebashi, Gunma, Japan); Kurumi Nakase, MD (Gunma University Graduate School of Medicine, Maebashi, Gunma, Japan).