
Abstract
Background:
Guidelines for return to driving after anterior cruciate ligament reconstruction (ACLR) have not been established.
Purpose:
To review the literature pertaining to driving after ACLR and provide evidence-based guidelines to aid clinicians in counseling patients about driving after ACLR.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic review was performed according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Two independent reviewers searched PubMed, EMBASE, and the Cochrane Library using the terms anterior cruciate ligament, ACL, drive, and driving. Studies reporting on functional recovery after ACLR were included when data regarding return to driving were reported.
Results:
Five studies were included. Two studies included patients who underwent right-sided ACLR. Of these, 1 study evaluated bone-patellar tendon-bone autograft and reported that brake response time (BRT) returned to normal approximately 4 to 6 weeks postoperatively. The other study found that BRT returned to normal 3 weeks after allograft ACLR, but 6 weeks elapsed after autograft ACLR before values were not significantly different than controls. One study reported that patients who underwent left-sided hamstring tendon autograft ACLR demonstrated BRTs similar to controls within 2 weeks, while those with right-sided ACLR had significantly slower BRTs until 6 weeks postoperatively. Another study including patients who underwent either right- or left-sided ACLR and employed a manual transmission simulator found that 4 to 6 weeks should elapse after ACLR with hamstring tendon autograft. Survey data from 1 study demonstrated that the mean time for patients to resume driving was 13 and 10 days after right- and left-sided ACLR, respectively.
Conclusion:
BRT returned to normal values approximately 4 to 6 weeks after right-sided ACLR and approximately 2 to 3 weeks after left-sided ACLR. According to 1 study in this review, ACLR laterality should be disregarded for patients who drive manual transmission automobiles, as a 4- to 6-week time period was required for driving ability to reach the level of healthy controls. Future studies should aim to elucidate the influence of graft choice and transmission type on return to driving after ACLR.
Anterior cruciate ligament reconstruction (ACLR) is among the most commonly performed orthopaedic surgeries in the United States. 25,33 Recovery of function after ACLR has been studied extensively in the literature. 3,9,19,40 ACL rupture is commonly sustained during a sports activity, and the decision to undergo ACLR is largely influenced by a patient’s desire to continue playing sports. Thus, studies assessing postoperative functional recovery after ACLR have focused primarily on the ability to return to sports.
Driving is an important activity of daily living. Accordingly, patients who undergo ACLR frequently ask their surgeons when it is safe to return to driving. Driving a motor vehicle is a complex task that requires adequate strength, reaction time, coordination, and proprioception. Several factors must be considered when counseling surgical patients on the issue of driving postoperatively. An extended period of driving restrictions may have a negative impact on a patient’s quality of life. However, if one’s ability to drive is functionally impaired, patients may pose a safety risk to themselves and other drivers.
Currently, there are no established guidelines regarding the appropriate amount of time to allow for recovery before driving should be resumed after ACLR. The purpose of this study was to review the current literature pertaining to driving after ACLR. In turn, we hope to provide an evidence-based overview to aid clinicians in counseling patients who want to return to driving after ACLR.
Methods
A systematic review was performed according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Two independent reviewers (H.S.S. and D.H.P.) searched PubMed, EMBASE, and the Cochrane Library using the terms anterior cruciate ligament, ACL, drive, and driving. The authors sought to include all studies investigating return to driving after ACLR. Studies reporting on general functional recovery after ACLR were included when data regarding return to driving were included. Articles published in languages other than English were excluded.
After removing duplicate search results, titles were screened, and abstracts were reviewed. Full-text articles were then assessed for eligibility. Data were extracted and cross-checked for accuracy by the same 2 reviewers. Data of interest included patient characteristics, surgical details (laterality, concomitant injuries and procedures, graft type, and graft-fixation technique), rehabilitation protocol, method for assessing recovery of driving ability, and all results of the reported return-to-driving evaluations.
Results
Study Details
Our initial search returned 87 studies (Figure 1). After applying our criteria, 5 studies 13,28,29,37,39 with a total of 281 patients who underwent primary ACLR were included in our review (Table 1). Four studies 13,28,37,39 used automobile-simulation devices to evaluate various parameters in 99 patients who underwent ACLR. One study surveyed 182 patients to quantify the time to early functional recovery (including driving in 148 patients) in the first 12 weeks after ACLR. 29
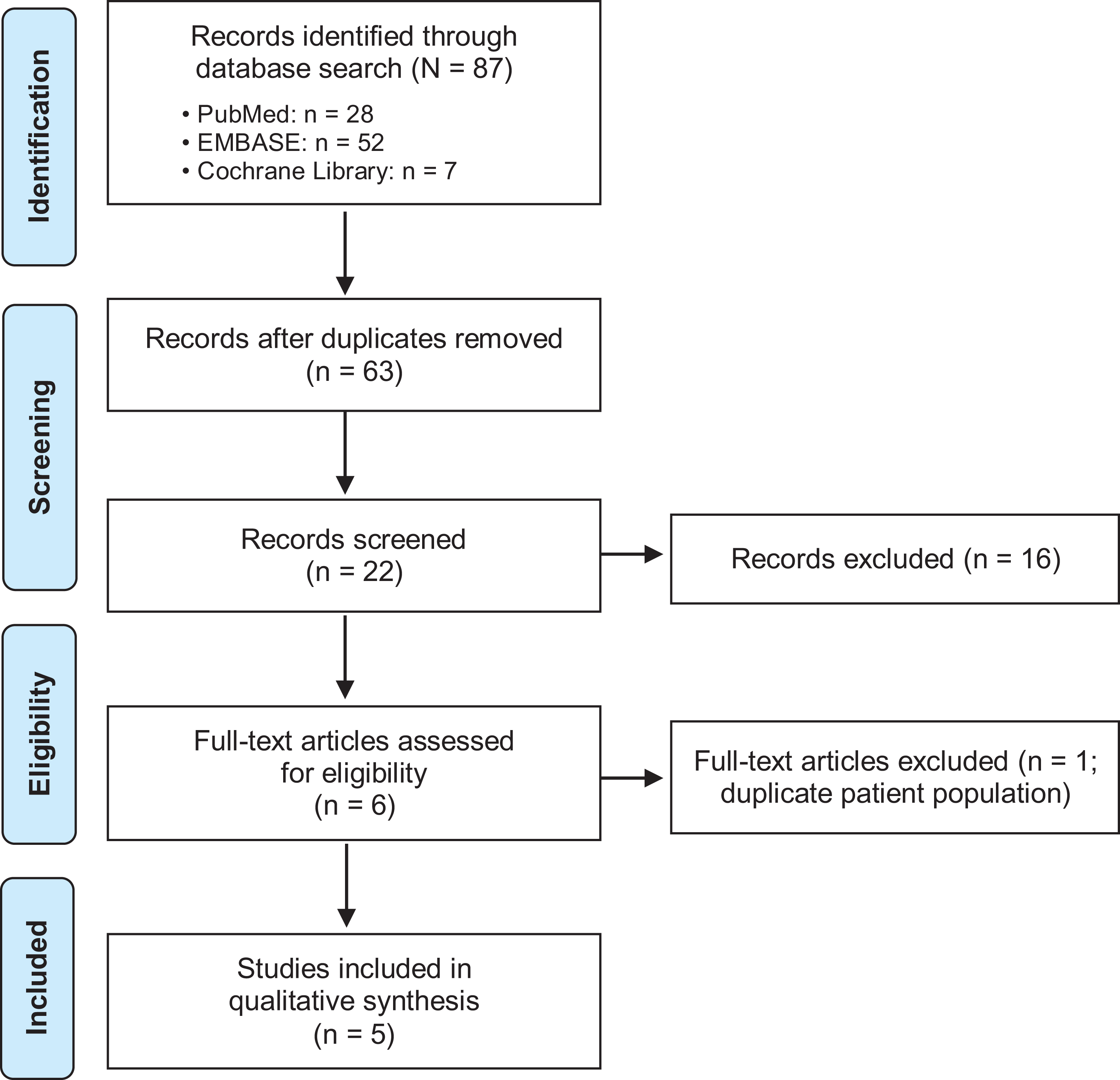
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart for the selection of the included studies.
Details of the Included Studies

a Mean ± SD. ACLR, anterior cruciate ligament reconstruction; BTB, bone--patellar tendon--bone autograft; HS, hamstring; LOE, Level of evidence; TA, tibialis anterior allograft.
Surgical Details
Two studies 13,39 included only patients who underwent right-sided ACLR, while the remaining 3 studies 28,29,37 included both right- and left-sided ACLR cases with comparative analyses. The presence or absence of concomitant procedures was reported in 3 studies. 29,37,39 Two studies 29,39 excluded patients with concomitant procedures, while Valenti et al 37 included patients who had concomitant meniscal repair (23%), partial meniscectomy (19%), or microfracture (3%).
The graft type used for ACLR was reported in 5 studies 13,28,29,37,39 (Table 2). Bone-patellar tendon-bone (BTB) autograft was used exclusively in 1 study, 13 while in the study by Valenti et al, 37 all patients received a hamstring (HS) autograft. In the study by Nguyen et al, 28 a majority of patients (90%) received HS tendon autografts while the remaining 10% received BTB autografts. Wasserman et al 39 performed a subgroup analysis based on the various graft types including BTB autograft (33%), HS tendon autograft (33%), and tibialis anterior allograft (33%). Last, participants in the study by Obermeier et al 29 received a variety of autografts and allografts including BTB autograft (46%), HS tendon autograft (38%), and various allografts (15%).
Surgical Details a

a ACL, anterior cruciate ligament; BTB, bone--patellar tendon--bone autograft; HS, hamstring tendon autograft; TA, tibialis anterior autograft.
The graft-fixation method was reported in 4 studies. 28,29,37,39 Among these studies, Nguyen et al 28 and Valenti et al 37 used similar fixation techniques: a suspensory system on the femoral side and interference screw on the tibial side, respectively. In the other 2 studies, 29,39 the fixation method was surgeon dependent.
Postoperative Rehabilitation
A postoperative rehabilitation protocol was reported in 3 studies. 29,37,39 Weightbearing status and range of motion after the ACLR varied among the studies. Two studies allowed immediate postoperative weightbearing. 29,39 Valenti et al 37 allowed immediate full weightbearing, except in patients who underwent concomitant meniscal repair. In these patients, the knee was immobilized in extension, and weightbearing was restricted for 2 weeks. Range of motion restrictions were implemented for the first 7 to 10 days in 1 study 39 and for the first 2 weeks in another. 37
Pain medication usage was reported in 3 studies. 13,29,37 Gotlin et al 13 asked patients to avoid taking pain medications on the day of testing. In the study by Valenti et al, 37 none of the patients required any narcotic pain medications at the 5-week mean time period in which they were evaluated. Obermeier et al 29 reported that the median time for discontinuation of narcotic pain medication was 9 days. Moreover, the median time to discontinuation of pain medication was significantly longer in patients who received autografts (10 days; range, 1-57 days) compared with allografts (6.5 days; range, 1-20 days).
Method of Evaluation
Four studies evaluated brake response time (BRT). 13,28,37,39 Among these, 2 studies 13,37 utilized a simple reaction time test to simulate an emergency-stopping situation. Patients were timed as they lifted their foot from the fully depressed accelerator and pressed on the brake as quickly as possible when a green signal changed to red at random intervals. Three studies 13,28,39 used an automobile simulator with automatic transmission requiring use of only the right leg. Conversely, Valenti et al 37 employed a manual transmission simulator incorporating a clutch pedal operated by the left leg. The test circuit by Valenti et al further assessed the driving skills of ACLR patients 4-6 weeks postoperatively compared to healthy controls. The driving ability in each group was evaluated by the number of collisions, the number of traffic violations, and brake use behavior on a manual transmission driving simulator in urban, highway, and mountain scenarios.
The protocol to measure the reaction time varied among studies. Total braking time (TBT), which is defined by the time between the display of the red signal to when the brake pedal is fully pressed, is reported in 3 studies. 28,37,39 Among these, 2 studies 37,39 measured BRT (the time between stimulus and initial contact with the brake pedal), and brake travel time (the time between initial contact with the brake pedal and when it was fully depressed). BRT was also reported in the study by Gotlin et al, 13 but the method by which it was evaluated was not clearly defined.
Nguyen et al 28 used an automobile simulator constructed by the Department of Electrical and Computer System Engineering of Monash University. Wasserman et al 39 used STISIM Drive automotive simulator (Systems Technology Inc.). Gotlin et al 13 used a brake reaction timer (Model 3548; American Automobile Association [AAA] Department of Traffic Safety and Engineering) and compared the results with normative data from the AAA Department of Traffic Safety and Engineering. Valenti et al 37 utilized the SIGNOS software (Prometeo Innovations) for all assessments. Each study 13,28,37,39 incorporated a practice run to familiarize patients with the equipment, and multiple test trials were recorded and averaged. Two studies 7,17 evaluated the patients every second week postoperatively to assess the progression of reaction time, and 1 study performed evaluations every third week beginning on postoperative week 1 (Table 1). 39 Valenti et al evaluated patients once, at 4 to 6 weeks after they underwent ACLR.
Driving Simulator
Two studies 28,37 compared the reaction time between patients with right- and left-sided ACLR. Nguyen et al 28 reported that compared with the controls, TBT was not affected in left-sided ACLR as early as 2 weeks postoperatively. However, a statistically significant difference in mean TBT was observed in patients who underwent right-sided ACLR (1503 ± 954 ms) compared with the controls (590 ± 145 ms) at 2-week follow-up (95% CI, 0.5 to 1.3; P < .001). Four weeks postoperatively, mean TBT was 805 ± 241 ms in patients with right-sided ACLR, and 590 ± 169 ms in controls (95% CI, 0.1 to 0.8; P = .013). Finally, no significant difference in mean TBT was detected between patients with right-sided ACLR (733 ± 209 ms) and controls at 6-week follow-up (587 ± 168; 95% CI, –0.005 to 0.7; P = .054). 28 Valenti et al 37 reported no significant differences in TBT (P = .069), BRT (P = .205), or brake travel time (P = .071) between controls and patients who underwent right-sided ACLR at 4- to 6-week follow-up (P > .05). Wasserman et al 39 reported the effect of different ACL grafts on BRT. They found that BRT returned to normal values by 3 weeks postoperatively in patients who underwent allograft ACLR compared with 6 weeks in patients with HS tendon and BTB autografts. 39 Gotlin et al 13 compared BRT with normative data from the AAA Department of Traffic Safety and Engineering, concluding that BRT returned to normal values approximately 4 to 6 weeks after ACLR.
The circuit test by Valenti et al 37 did not demonstrate significant differences between patients who underwent ACLR and controls in any of the measurement indices including test time (P = .21), collision with another vehicle (P = .813), collisions with a fixed object (P = .65), pedestrian impacts (P = .53), red traffic light violations (P = .49), sidewalk invasions (P = .58), brake use (P = .13), brake use >75% (P = .11), number of brake uses longer than 5 s (P = .79), and number of brake uses longer than 10 s (P = .30). Patients with right-sided ACLR had a higher number of collisions with fixed objects (2.82 vs 1.84; P = .239), more pedestrian impacts (0.23 vs 0.00; P = .221), and slower BRTs (585.69 ms vs. 456.02 ms; P = .069), but none of these outcomes reached statistical significance.
Survey
According to the results of the survey administered by Obermeier et al, 29 the mean time at which patients resumed driving after ACLR was 11 days. Subgroup analysis demonstrated that the mean time at which patients resumed driving after ACLR was slightly increased after right-sided ACLR (13 days) compared with left-sided ACLR (10 days). 29 Factors that predicted faster return to driving were increased age (OR, 1.06; 95% CI, 1.02-1.09; P < .01), male sex (OR, 3.33; 95% CI, 1.54-7.14; P < .01), and left-sided ACLR (OR, 4.06; 95% CI, 1.89-8.72; P < .01).
Clinical Evaluation
Nguyen et al 28 attempted to validate a clinical surrogate for evaluating driving ability by comparing BRTs with the results of 2 clinical tests: the stepping test and the standing test. The stepping test was meant to simulate BRT. Patients were seated with both knees and hips flexed at 90°, and a paper box measuring 2.5 × 2.5 × 30 cm was placed beside the patient’s right foot. Patients were instructed to step across either side of the box and firmly plant the heel without touching the box. The standing test was meant to simulate patients’ ability to fully straighten the leg for depressing the brake pedal. Patients were instructed to stand from a sitting position until the knees were fully extended before sitting down again. Each test was performed by counting the number of times each activity could be carried out in a 10-s period. It was found that the stepping test correlated significantly with BRT preoperatively (r = −0.468; P = .002), at 2 weeks (r = −0.786; P < .001), 4 weeks (r = −0.680; P < .001), 6 weeks (r = −0.654; P < .001), and 8 weeks (r = −0.572; P < .001). The standing test was also found to be significantly correlated with reaction time preoperatively (r = −0.519; P = .001), at 2 weeks (r = −0.504; P = .001), 4 weeks (r = −0.540; P < .001), 6 weeks (r = −0.553; P < .001), and 8 weeks (r = −0.398; P = .011).
Discussion
Based on our review of the current literature, it appears that after ACLR, patients resume driving before their BRT returns to preoperative levels. In the survey administered by Obermeier et al, 29 the mean time at which patients resumed driving after ACLR was 11 days. According to the 2 included studies 13,28 that evaluated BRT at multiple intervals in the early postoperative period, these patients would not have recovered adequate reaction time to safely return to driving. Nguyen et al 28 reported that patients who underwent left-sided HS tendon autograft ACLR demonstrated BRTs similar to controls within 2 weeks. However, those with right-sided ACLR had significantly slower response times until the sixth postoperative week. Although the mean differences in reaction time may appear to be minor (913 ms at 2 weeks and 215 ms at 4 weeks), a vehicle traveling at 60 mph travels 80.3 feet in 913 ms and 18.9 feet in 215 ms.
Wasserman et al 39 provided further insight regarding differences in reaction time based on the graft type. While all patients in their cohort underwent right-sided ACLR, graft type appeared to have an effect on BRT. It was found that BRT returned to normal values 3 weeks postoperatively in patients who underwent allograft ACLR. However, in the setting of autograft ACLR, 6 weeks elapsed before BRT was not significantly different from controls. In the other study that exclusively evaluated patients after right-sided ACLR, Gotlin et al 13 concluded that BRT returned to normal values at approximately 4 to 6 weeks postoperatively. Valenti et al 37 included patients with right- and left-sided ACLR, but unlike the other studies, a manual transmission automobile simulator was employed. The authors concluded that ACLR with HS tendon autograft does not impair driving performance at 4 to 6 weeks postoperatively with regard to skill, ability to drive, or BRT.
As a result of individual differences in patients’ abilities to recover functional capacity after ACLR, some may be able to resume driving safely before others. However, evaluating BRT using an automobile simulator before clearance is not a reasonable means of making this assessment, since it is not widely available to all patients. Nguyen et al 28 addressed this limitation by comparing BRTs with the results of 2 clinical tests: the stepping test and the standing test. The authors reported that each of the tests correlated significantly with BRT as measured by the driving simulator. They suggested that return to driving can be evaluated in the outpatient setting by administering these tests 24 hours before surgery and again 6 weeks postoperatively. When the results of either test return to the patient’s preoperative level, patients may be cleared to drive. Future studies should evaluate the utility of these tests as clinical surrogates for return to driving ability after ACLR. In addition, researchers should attempt to develop and validate other clinical surrogates for evaluating postoperative driving ability. By doing so, a more comprehensive evidence-based protocol can be implemented for functional evaluation of driving ability in a clinical setting.
It is well-known that recovery of functional ability varies among patients who undergo ACLR. 1,10,14 Thus, it would not be appropriate to apply a predetermined time line for a return to driving without considering patient-specific differences. Factors such as preoperative rehabilitation, intraoperative analgesia protocols, concomitant surgeries, and postoperative rehabilitation have been shown to influence functional outcomes. 12,22,23,34,36,38 Intuitively, the laterality of surgery is also an important variable. Moreover, studies 21,30 have shown differences in pain levels and pain medication requirements among patients who underwent ACLR with various grafts. The implications of postoperative pain on safe driving are two-fold. One, increased pain levels in patients who undergo ACLR have been shown to be associated with strength and proprioceptive deficits in the first postoperative year. 7 Two, patients who experience more pain may consume more narcotic pain medication, and prescription opioid use is an independent risk factor for fatal motor vehicle collisions and crash culpability. 5,6,24 Based on the questionnaire administered by Obermeier et al, 29 discontinuation of narcotic pain medication occurred at a median of 9 days but at up to 44 days postoperatively among surveyed patients. In addition to the aforementioned patient-specific factors, it is important to ensure that patients are no longer using narcotic pain medication before they are cleared to resume driving.
Return to driving after various orthopaedic surgeries has been reported extensively in the literature. ‡ DiSilvestro et al 11 performed a systematic review to determine when patients can safely return to driving after 20 common orthopaedic procedures. However, 3 of the 5 studies 29,37,39 in the current review were not yet published at the time that their study was performed. Similar to our findings, the authors reported that survey data suggest patients return to driving before observer-reported outcome measures have normalized to preoperative or control-arm levels. Therefore, physicians should closely monitor the time at which patients resume driving and attempt to implement clinical tests that can predict safe driving ability.
The current review has several strengths. To our knowledge, this is the first attempt to consolidate all the available data on return to driving after ACLR. To minimize the introduction of bias by a single reviewer, 2 independent reviewers performed the literature search, and after agreeing upon the included studies, each extracted data separately.
Limitations also exist in our study. Because we aimed to investigate a measure that is not commonly reported after ACLR, a relatively small number of studies was included in our analysis. Furthermore, the included studies evaluated a relatively small number of patients. In addition, there were no preinjury or preoperative measurements of BRT, making it difficult to assess the true influence of ACL injury and ACLR on reaction time. Only 1 study in this review attempted to determine the predictive value of in-office functional tests as related to driving ability. Lastly, meta-analysis was not feasible because of the heterogeneity among the included studies.
Conclusion
BRT returns to normal values at approximately 4 to 6 weeks after right-sided ACLR and approximately 2 to 3 weeks after left-sided ACLR. According to 1 study 37 reviewed, ACLR laterality should be disregarded for patients who drive manual transmission automobiles, as a 4- to 6-week time period was required for driving ability to reach the level of healthy controls. The stepping test and standing test are clinical surrogates for driving ability, which may be used to evaluate patients before driving is permitted. However, further studies are needed to validate these clinical tests and evaluate other functional measures that are predictive of driving ability. In addition, future studies should aim to elucidate the influence of graft choice and transmission type on return to driving after ACLR.
Footnotes
Notes
Acknowledgment
The authors thank Emily Jaramillo for her assistance with the literature search.
Final revision submitted June 12, 2020; accepted June 30, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.T.B. has received consulting fees from DJO, Encore Medical, and Smith & Nephew; nonconsulting fees from Mitek, Smith & Nephew, and Stryker; and royalties from Shukla Medical. E.C.M. has received educational support from Mitek, Smith & Nephew, Stryker, and Zimmer Biomet; consulting fees from Zimmer Biomet; speaking fees from Arthrex and Stryker; and royalties from Zimmer Biomet. R.M.F. has received grant support from Arthrex, educational support from Arthrex/Medwest and Smith & Nephew, speaking fees from Arthrex, and royalties from Elsevier. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.