
Abstract
Background:
Gluteus medius (GM) tears are a known cause of dysfunction and disability predominantly in older women.
Purpose
To report on return to activity, patient-reported outcomes (PROs), and a uniquely calculated minimal clinically important difference (MCID) at a minimum 2-year follow-up for active patients who had undergone either an endoscopic or an open GM repair.
Study Design:
Case series; Level of evidence, 4.
Methods:
Patients were considered eligible if they (1) underwent a GM repair with or without concomitant central and peripheral compartment procedures; (2) had baseline preoperative and minimum 2-year scores for the modified Harris Hip Score (mHHS), Nonarthritic Hip Score (NAHS), Hip Outcome Score–Sports Specific Subscale (HOS-SSS), and visual analog scale (VAS) for pain; and (3) participated in a physical activity or sport within 1 year before their surgery. Return to activity was defined as the patient being able to participate in his or her activity at a minimum of 2 years postoperatively.
Results:
Of 87 eligible patients, 84 (96.6%) met all inclusion criteria. The mean follow-up was at 44.5 months. Six patients (7.1%) underwent an open GM repair, while the remaining 78 (92.9%) underwent an endoscopic GM repair. Concomitant central and peripheral compartment arthroscopic procedures were performed in 69 patients (82.1%). All PROs significantly (P < .001) improved as follows: mHHS, from 59.0 to 85.8; NAHS, from 57.9 to 84.0; HOS-SSS, from 32.6 to 63.7; and VAS pain, from 5.4 to 1.9. A total of 57 patients (67.9%) returned to their preoperative activity at the 2-year follow-up. The MCID was calculated for the mHHS, NAHS, and HOS-SSS to be 7.5, 7.4, and 10.9, respectively, with 79.3%, 86.4%, and 70.2% of patients achieving the MCID for each respective PROs.
Conclusion:
Active patients over the age of 50 years may benefit from endoscopic or open repair of GM tears, as the majority of patients in our cohort were able to return to their activity of choice. All measured PROs had significantly improved at a minimum 2-year follow-up, with high survivorship, satisfaction, and clinical effectiveness. Patients with partial-thickness tears compared with full-thickness tears and those who underwent isolated GM repair compared with GM repair with concomitant procedures had similar return to activity rates and PROs at the latest follow-up.
Physical inactivity in the elderly is related to many noncommunicable chronic health conditions globally. 4,30 According to a World Health Organization report, approximately 3.2 million deaths each year are attributable to physical inactivity. 43 As the population older than 60 years is expected to be nearly 28% of the total population by 2100, it is becoming increasingly important to help older people maintain a healthy and active life. 40
In total, 21 muscles cross the hip, which provides strength, control, and stability for the body’s central pivot point. 27 When these muscles are injured, many routine movements involving both functional and recreational activities can be affected. 27 The gluteus medius (GM) is one of the essential hip muscles that maintain coronal plane stability in the upright position. 36 This function is especially crucial for those who adhere to an active lifestyle. In activities, such as running, the GM produces the most significant mean peak muscle force and abduction torque of all hip muscles and absorbs ground-reaction forces in the loading phase. 36 Therefore, tears of the GM can lead to physical impairment from inadequate coronal plane pelvic control.
GM tears tend to be degenerative and commonly occur in women between the ages of 40 and 60 years. 2 The prevalence in the general population ranges from 10% to 25%. 39 GM tears are part of a larger entity known as greater trochanteric pain syndrome, with symptoms of chronic lateral hip pain, abductor weakness, and gait dysfunction. 13,38 It has been shown that some patients with greater trochanteric pain syndrome are less likely to be employed full time and show levels of disability and quality of life similar to the levels associated with end-stage hip osteoarthritis. 12 Additionally, activities of daily living, such as sleeping, walking, or stair climbing, are commonly disrupted because of GM tears. 26 As a result, physical activity may decline and lead to negative implications for the general health and well-being of patients with GM tears. 12
Treatment for GM tears initially begins with activity modification, anti-inflammatory pain medications, physical therapy, extracorporeal shock therapy, corticosteroid injections, and platelet-rich plasma injections. 15,16,22,23,32 Surgery is indicated when treatment with these conservative measures for at least 3 months has failed. Use of both open and endoscopic GM repair techniques has been successful, with improvements in patient-reported outcomes (PROs) at short- and midterm follow-ups. 1,6,31 However, there is a paucity of literature regarding return to activity for patients undergoing surgical repair of GM tears.
The purpose of this study was to report on return to activity, PROs, and a uniquely calculated minimal clinically important difference (MCID) at a minimum 2-year follow-up for active patients who had undergone either an endoscopic or an open GM repair. We hypothesized that the majority of patients would be able to return to their activity of choice and demonstrate improved PROs at the latest follow-up, with high satisfaction after their surgery.
Methods
Patient Selection
Patients were considered eligible for inclusion if they (1) had undergone a GM repair with or without concomitant central and peripheral compartment procedures; (2) had baseline preoperative scores for the modified Harris Hip Score (mHHS), Nonarthritic Hip Score (NAHS), Hip Outcome Score–Sports Specific Subscale (HOS-SSS), and visual analog scale (VAS) for pain; and (3) had participated in a physical activity or sport within 1 year before their surgery. Patients were excluded if they had undergone previous ipsilateral hip surgery; had previous ipsilateral hip conditions, such as Perthes, avascular necrosis, slipped capital femoral epiphysis, or femoral head or acetabulum fractures; had Tönnis classification >1; were younger than 50 years; were unwilling to participate in research; or had missing data regarding their return to preoperative activities. Patients who met all inclusion criteria and had a minimum 2-year follow-up were analyzed.
All patients participated in the American Hip Institute Hip Preservation Registry. While the present study represents a unique analysis, data on some patients in this study may have been reported in other studies. All data collection received institutional review board approval.
Clinical Evaluation
A comprehensive physical examination was performed on all patients preoperatively and postoperatively by the senior author (B.G.D.). Femoroacetabular impingement (FAI) was evaluated using anterior, lateral, and posterior impingement tests. 19 A positive test suggestive of labral pathology was considered when deep anterior groin pain was reported using these maneuvers. Abductor strength was measured with the patient lying on the contralateral side with the affected leg abducted, extended at the hip and knee, and slightly internally rotated. The patient’s gait was examined for a positive Trendelenburg sign. Sway to the contralateral side during a single-leg stance was also recorded. Additionally, peritrochanteric pain and tenderness were evaluated. When present, GM and labral pathology were confirmed using magnetic resonance imaging (MRI) for all patients. 20
Surgical Indications
Patients underwent a minimum of 3 months of nonsurgical treatment (rest, nonsteroidal anti-inflammatory drugs, physical therapy, corticosteroid injections, or platelet-rich plasma injections). If conservative treatment failed, surgery was recommended for the patient. If the MRI scan showed a partial- or full-thickness GM tear without substantial retraction or fatty atrophy, the patient was indicated for an endoscopic repair. If retracted tears or fatty atrophy was present, patients were indicated for open repair. Concomitant hip arthroscopy to address central and peripheral compartment pathology was indicated when preoperative evaluation was suggestive of symptomatic FAI.
Endoscopic Surgical Technique
All surgeries were performed by the senior author. After all central and peripheral compartment procedures were completed when indicated, the GM was assessed. The arthroscope was placed in the peritrochanteric space through the distal anterolateral portal for viewing, while anterolateral and posterolateral accessory portals were utilized as working portals. A trochanteric bursectomy was performed to fully visualize the peritrochanteric space and assess the GM pathology.
The GM insertion was probed to confirm undersurface destabilization from its attachment on the lateral facet when a partial-thickness tear was suspected. Low-grade partial-thickness tears were repaired using a suture staple technique. 18 A transtendinous window with side-to-side repair was employed for high-grade partial-thickness tears. 11 Full-thickness tears were repaired using a double-row suture bridge construct to re-create the normal footprint. 10
Open Surgical Technique
An incision centered over the posterior one-third of the greater trochanter was utilized for an open repair in patients with a full-thickness tear with suspected retraction and/or fatty infiltration. The fascia lata was incised in line with its fibers, and the gluteus maximus was bluntly split. A trochanteric bursectomy was performed to remove any inflamed tissue and expose the GM. Scar tissue around the tendon was debrided, and the area of the greater trochanter was decorticated using a bur to create a bleeding bed of bone for healing. The GM tendon was repaired using a double-row suture bridge technique in a similar fashion to the endoscopic repair. 21
Rehabilitation
Patients who had a suture staple repair were instructed to wear a fitted X-act ROM hip brace (DJO Global Vista) and use crutches with partial weightbearing (20 lb [9 kg]) for 2 weeks. Physical therapy began immediately after surgery. Patients who underwent a transtendinous repair or double-row suture bridge were instructed to wear the brace and adhere to partial weightbearing restrictions for 6 weeks. 21 Physical therapy began 6 weeks postoperatively in these patients. Flexion was restricted to 0° to 90° with no abduction while in the brace. Patients were permitted to begin using a stationary bicycle immediately after surgery. Patients were allowed to return to activity after 6 to 8 months at the discretion of the physical therapist.
Surgical Outcome Measurement
Patients were given baseline questionnaires preoperatively that assessed the following PROs: mHHS, NAHS, HOS-SSS, and a VAS pain scale of 0-10, with 0 representing no pain and 10 representing worst pain possible. At 3 months after surgery, 1 year, and annually after that, patients were given similar questionnaires to assess the following: mHHS, NAHS, HOS-SSS, VAS pain, international Hip Outcome Tool (iHOT-12), and the physical and mental components of the Veterans RAND 12-Item Health Survey (VR-12P and VR-12M, respectively) and 12-Item Short Form Health Survey (SF-12P and SF-12M, respectively). Patient satisfaction on a VAS scale of 0-10, with 10 representing extreme satisfaction, was also collected.
In order to determine meaningful clinical improvement for GM repairs, a unique MCID was calculated for mHHS, NAHS, and HOS-SSS by taking half the baseline SD for each PROs as previously reported by Norman et al. 28
Patients’ respective preoperative activities were collected. Return to activity was defined as the patient being able to participate in his or her activity at a minimum of 2 years after the repair.
Statistical Analysis
All statistical analyses were performed using Microsoft Excel with the Real Statistics Add-in package (Microsoft Corporation). Normality and equality of variance were measured using the Shapiro-Wilk test and F test, respectively. All continuous data were assessed using the 2-tailed t test or its nonparametric equivalent. All categorical data were calculated using the Fisher exact test or chi-square test. A threshold of P = .05 was considered statistically significant.
Results
Patient Characteristics
The patient selection process is outlined in Figure 1. After all inclusion and exclusion criteria were employed, a total of 87 patients were deemed eligible, of which 84 (96.6%) had a minimum 2-year follow-up. The average age at the time of surgery was 60.9 ± 7.0 years (range, 50.5-75.9 years). Of the 49 patients who reported a specific date of symptomatic onset, the average period of symptoms before surgery was 58.0 ± 7.5 months (range, 45.1-76.6 months). The mean follow-up was 44.5 ± 19.3 months (range, 24.0-96.2 months). All patient characteristics are summarized in Table 1. A breakdown of the patient cohort’s preoperative activities is represented in Figure 2.
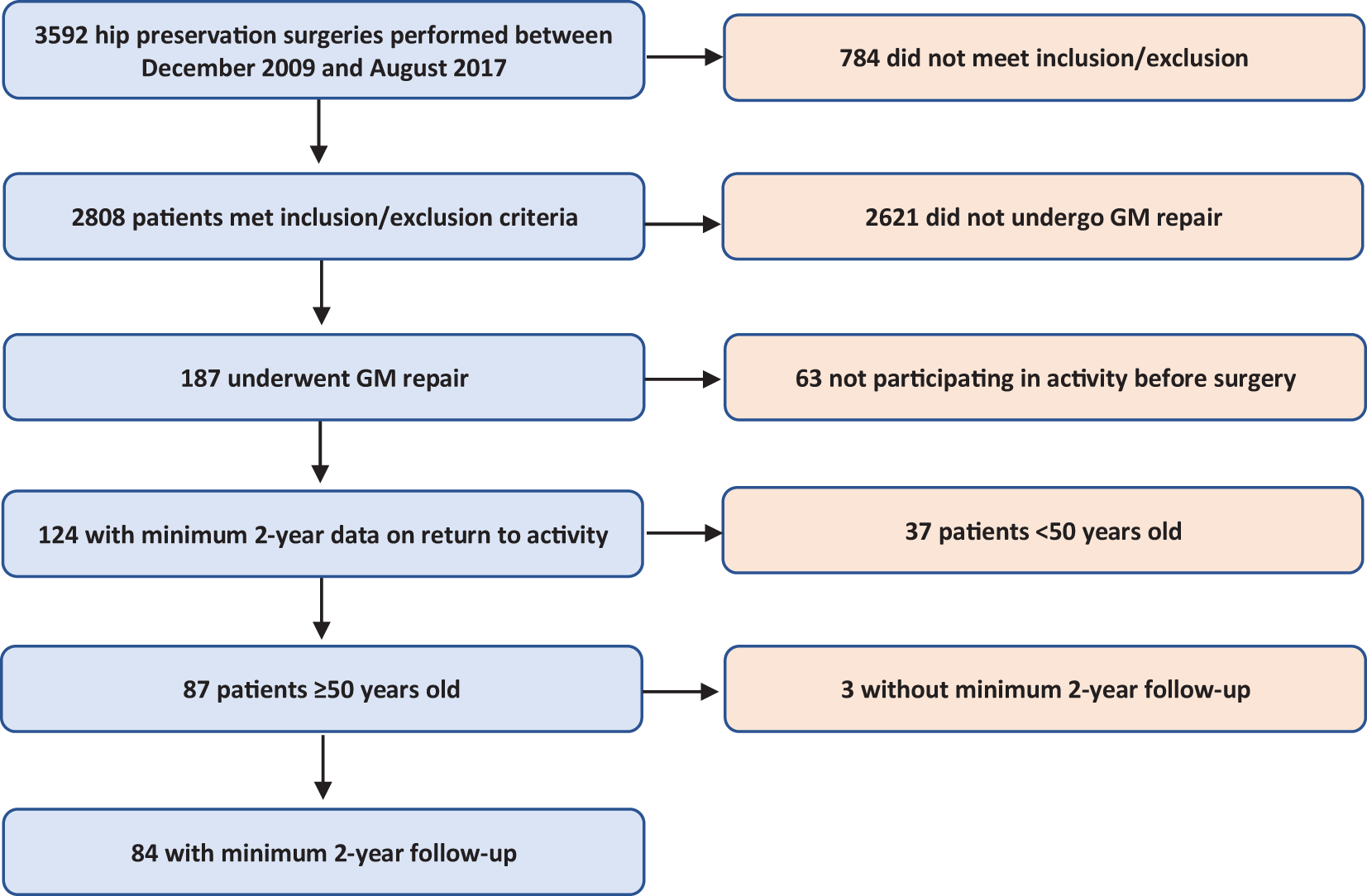
Patient selection process. GM, gluteus medius.
Participant Characteristics a
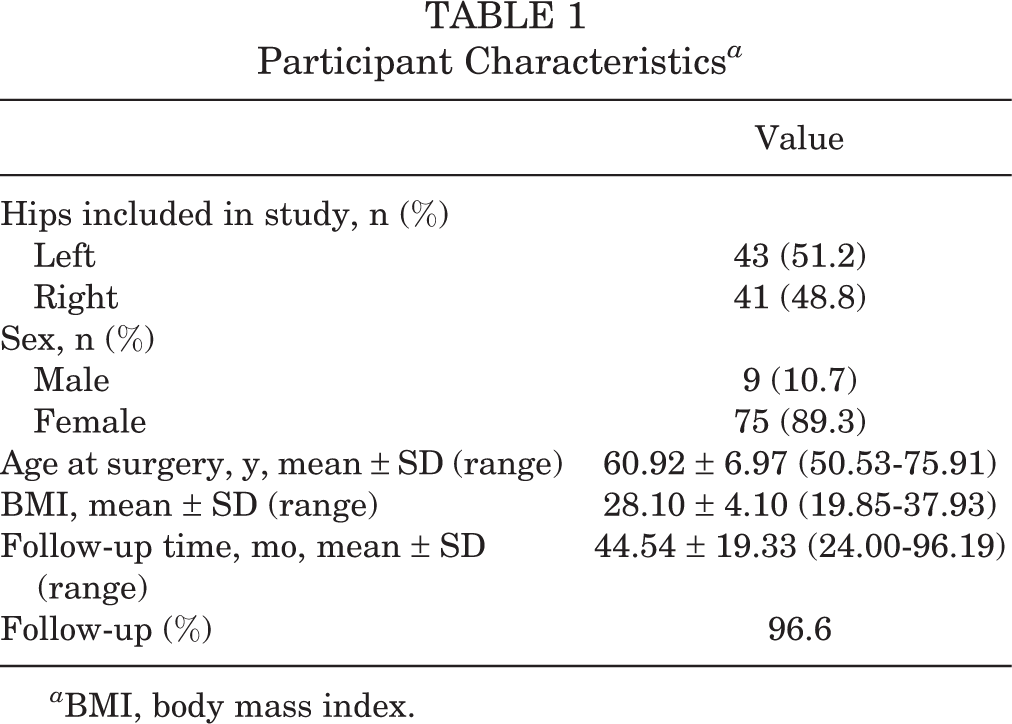
a BMI, body mass index.

Breakdown of preoperative activities.
Intraoperative Findings
The intraoperative findings of GM pathology are summarized in Table 2. The majority of patients (77.4%) had partial-thickness GM tears compared with full-thickness tears. Fifteen patients (17.9%) had low-grade partial-thickness tears, defined as having <50% of tendon involvement within the tear. Fifty patients (59.5%) had high-grade tears with >50% tendon involvement.
Intraoperative Findings a
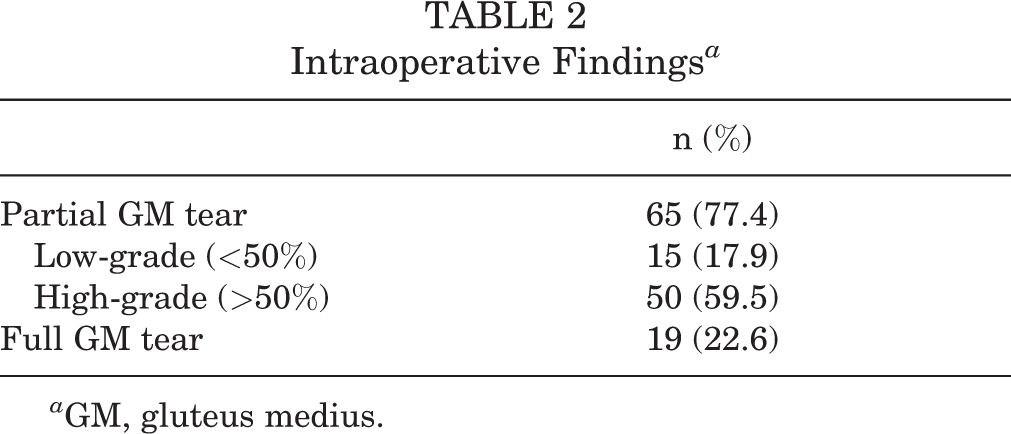
a GM, gluteus medius.
Procedures Performed
Tables 3 and 4 summarize all concomitant central and peripheral compartment procedures as well as GM treatment, respectively. Fifteen patients underwent isolated GM repair and thus did not have any concomitant procedures performed. Six patients (7.1%) underwent an open GM repair, while the remaining 78 (92.9%) underwent an endoscopic repair of their GM.
Central and Peripheral Compartment Procedures Performed

a Fifteen patients underwent an isolated endoscopic or open gluteus medius repair without concomitant hip arthroscopy.
Gluteus Medius Treatment a

a GM, gluteus medius.
Patient-Reported Outcomes
All of the PROs (mHHS, NAHS, and HOS-SSS) and VAS pain scores significantly improved from baseline at latest follow-up (P < .001) (Figures 3 and 4). The latest PROs for all other recorded outcomes are summarized in Figure 5. Additionally, the MCID was calculated for the mHHS, NAHS, and HOS-SSS to be 7.5, 7.4, and 10.9, respectively. The proportion of patients achieving MCID is reported in Table 5. Patient satisfaction was 8.0 ± 2.6 (95% CI, 7.4-8.6) on the 10-point scale.
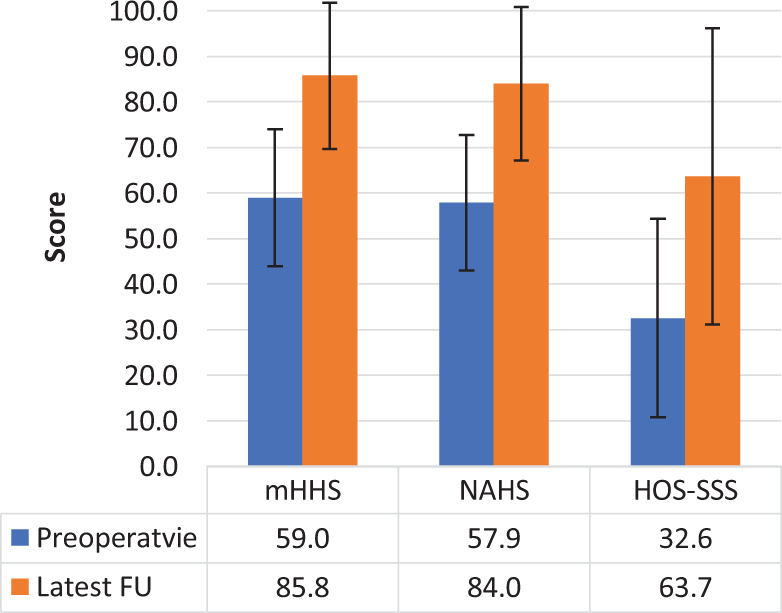
Preoperative versus latest follow-up patient-reported outcome scores. FU, follow-up; HOS-SSS, Hip Outcome Score–Sports Specific Subscale; mHHS, modified Harris Hip Score; NAHS, Nonarthritic Hip Score.

Visual analog scale (VAS) scores for pain (0-10 points; 0 = no pain, 10 = worst pain possible) and satisfaction (0-10 points; 10 = highest satisfaction) at the preoperative (Preop) and latest follow-up (FU).

Latest follow-up for additional patient-reported outcomes (PROs). FU, follow-up; iHOT-12, international Hip Outcome Tool; M, mental summary; P, physical summary; SF-12, 12-Item Short Form Health Survey; VR-12, Veterans RAND 12-Item Health Survey.
MCID a
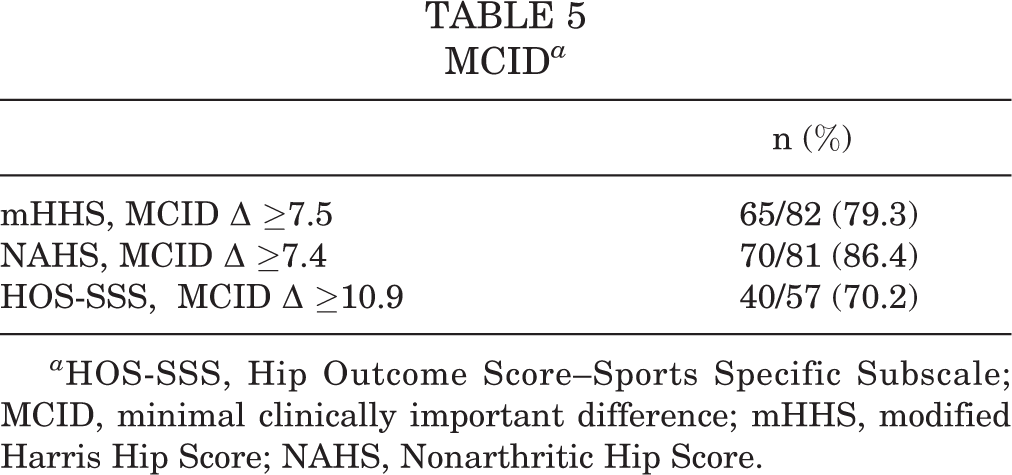
a HOS-SSS, Hip Outcome Score–Sports Specific Subscale; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; NAHS, Nonarthritic Hip Score.
A subanalysis was performed to analyze PROs between patients with full-thickness and partial-thickness tears. At the latest follow-up, both groups achieved a patient satisfaction score of 8.0 (P = .598), and the VAS for the full-thickness tear group was 1.8 compared with 1.9 for the partial-thickness tear group (P = .624). As demonstrated in Figure 6, PROs were similar between groups for mHHS (P = .608), NAHS (P = .969), iHOT-12 (P = .821), HOS-SSS (P = .199), SF-12P (P = .542), VR-12M (P = .364), and VR-12P (P = .558) at the latest follow-up. The only PROs that differed was SF-12M (P = .049). The 2 groups also returned to activity at similar rates (P = .100).
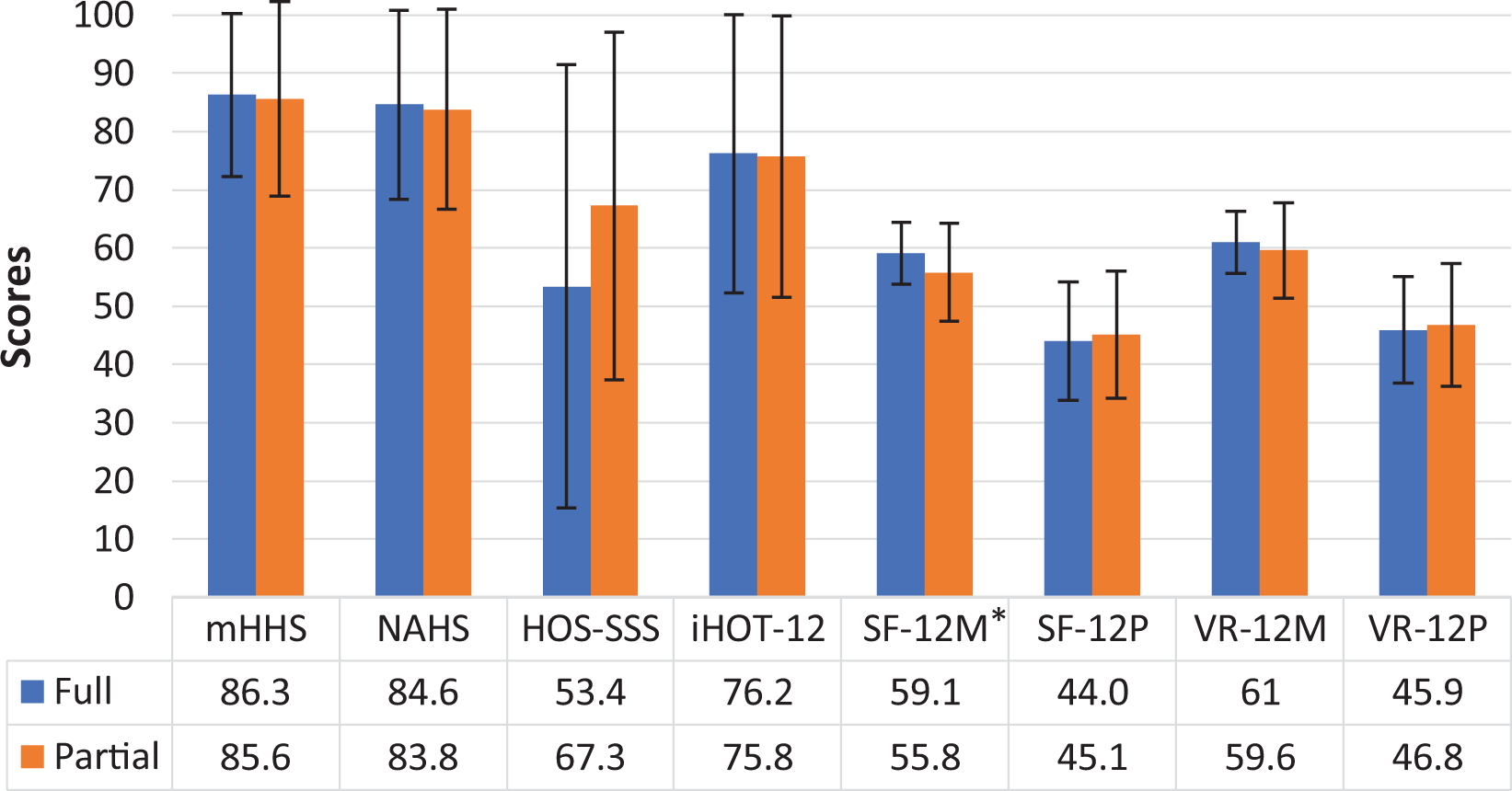
Full-thickness versus partial-thickness gluteus medius tear patient-reported outcomes. *Statistically significant difference (P < .05). HOS-SSS, Hip Outcome Score–Sports Specific Subscale; iHOT-12, international Hip Outcome Tool; M, mental summary; mHHS, modified Harris Hip Score; NAHS, Nonarthritic Hip Score; P, physical summary; SF-12, 12-Item Short Form Health Survey; VR-12, Veterans RAND 12-Item Health Survey.
An additional subanalysis was performed to analyze PROs between patients who underwent isolated GM repairs and those who underwent GM repairs with concomitant central and peripheral compartment procedures. As demonstrated in Figure 7, all PROs were similar between these groups for mHHS (P = .091), NAHS (P = .211), iHOT-12 (P = .151), HOS-SSS (P = .201), SF-12M (P = .232), SF-12P (P = .054), VR-12M (P = .070), and VR-12P (P = .071) at the latest follow-up. Patient satisfaction rates for the concomitant and isolated procedure groups were 8.2 and 7.1, respectively (P = .266). The VAS values for the 2 groups were 1.6 and 3.0, respectively (P = .116). The 2 groups returned to activity at similar rates (P = .472).
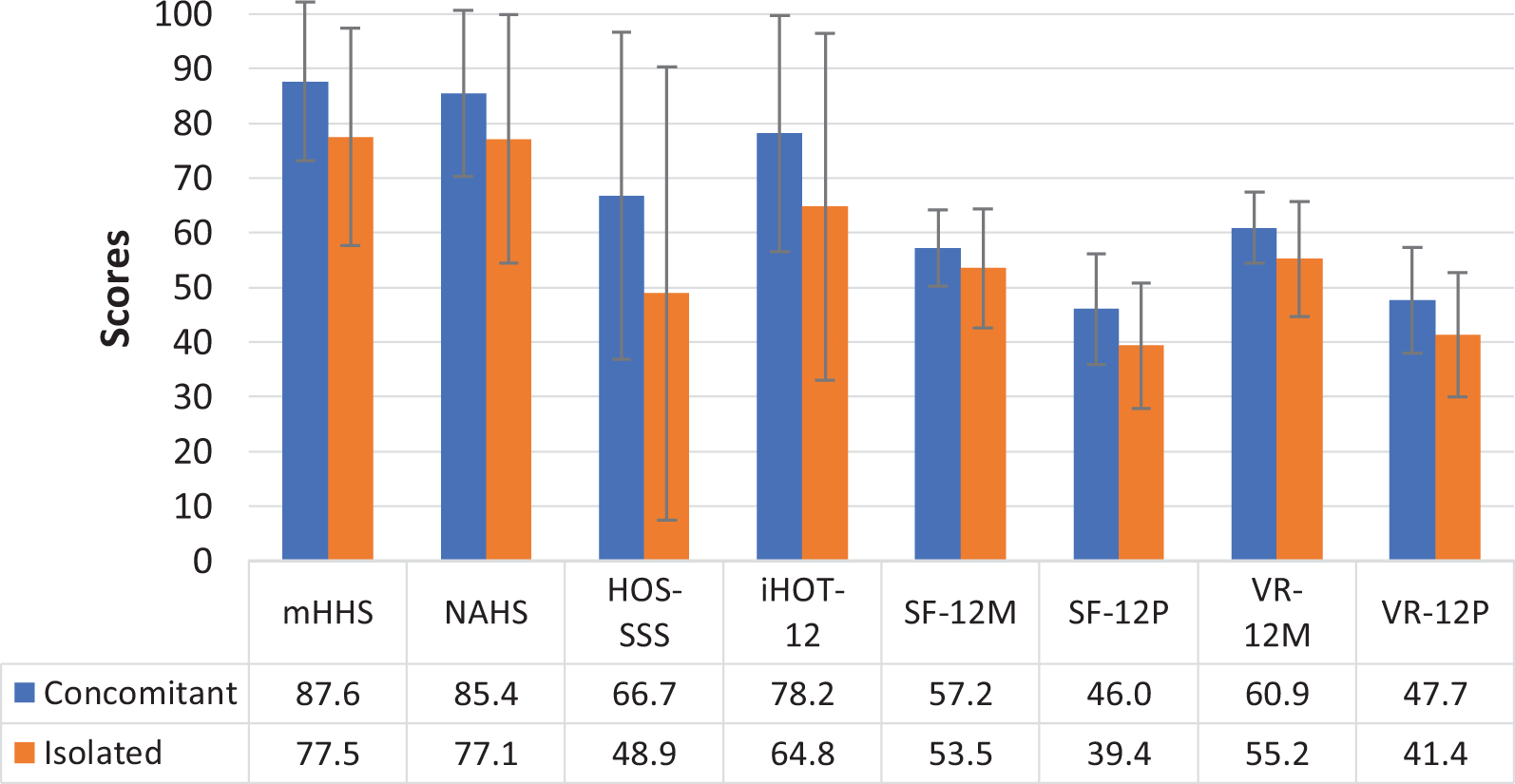
Concomitant versus isolated gluteus medius repair patient-reported outcomes (PROs). HOS-SSS, Hip Outcome Score–Sports Specific Subscale; iHOT-12, international Hip Outcome Tool; M, mental summary; mHHS, modified Harris Hip Score; NAHS, Nonarthritic Hip Score; P, physical summary; SF-12, 12-Item Short Form Health Survey; VR-12, Veterans RAND 12-Item Health Survey.
Return to Activity
Of the 84 patients, 57 (67.9%) returned to their preoperative activity at the 2-year follow-up. Of these 57 patients, 39 returned to the same or a higher level than that before their injury, while the remaining 18 returned to their previous activity but at a lower reported level. Twenty seven patients (32.1%) were unable to return to activity. Eight (9.5%) patients reported they were unable to return to activity because of issues, such as back pain, contralateral hip pain, loss of interest, or lifestyle transition. Nineteen patients (22.6%) were unable to return because of issues regarding their surgically repaired hip. All 27 patients who did not return to activity were women, while the 57 who did return were made up of 48 women and 9 men (P = .029). Additionally, there were no differences (P > .05) between the patients who returned to activity and those who did not in terms of age (60.8 vs 61.2 years, respectively), body mass index (27.6 vs 29.1, respectively), type of repair, or concomitant procedures performed. Table 6 summarizes the rate of return based on activity.
Type of Activity a

a RTA, return to activity.
Secondary Surgeries
Two patients (2.4%) required revision arthroscopy at a mean of 12.2 ± 7.7 months (range, 6.8-17.7 months) because of a retear of their GM. Both patients initially underwent an endoscopic transtendinous repair for a high-grade partial-thickness tear. There were 5 patients (6.0%) who converted to total hip arthroscopy at a mean of 20.23 ± 16.14 months (range, 9.2-48.2 months). Three of these 5 patients initially underwent an endoscopic transtendinous repair, 1 underwent an endoscopic double-row suture bridge repair, and 1 underwent an open double-row suture bridge repair.
Discussion
Physical activity in an older population is attributed to many possible health benefits, including lower rates of cardiovascular and metabolic disease, a lower risk of dementia, improved cognition, less depression, and a lower mortality risk. 14,17,24,25,33 After adjusting for age and socioeconomic status, it was shown that sedentary people older than 50 years had twice the risk of death compared with those with high levels of physical activity. 3 As the population older than 50 years of age is expected to increase in the next 50 years, health care providers need to be able to help these individuals maintain an active lifestyle. 40 In our cohort, 68% of active patients older than 50 years were able to return to their activity or sport at a minimum of 2 years after GM repair. Those involved in bicycling, running, golf, and volleyball experienced the highest rates of return to activity.
Nineteen patients (22.6%) were unable to return to activity because of issues regarding their surgically repaired hip. All 19 patients were women, which demonstrated a significant disproportion compared with those who returned to activity. In general, women have a higher predilection to GM tears than do men. One suggested theory for this is that women have wider pelvic girdles, which can lead to increased forces acting on the GM tendon. 35 Because of this biomechanical disadvantage, increased tears and reduced return to activity rates in women may result from dissimilarities in bony anatomy.
Dysfunction and disability can result from GM tears. Fortunately, many previous studies have demonstrated success using endoscopic GM repair. Voos et al 41 first reported successful outcomes after endoscopic GM repair at a 2-year follow-up. Recently, midterm success has also been shown. 31 In both of these studies, concomitant intra-articular procedures were performed in every patient before the GM repair. Likewise, in this present study, 69 of the 78 patients undergoing an endoscopic GM repair had concomitant procedures performed. This method ensures that all hip pathology can be treated when preoperative workup is suggestive of FAI and peritrochanteric pathology. Akin to arthroscopic rotator cuff repairs where intra-articular pathology is evaluated and treated before entering the subacromial space, we believe a similar approach can be applied when treating GM tears with clinical evidence of FAI.
GM tears can present as partial- or full-thickness tears, both of which are amenable to endoscopic repair. Domb et al 9 showed that endoscopic repair through a transtendinous or double-row suture bridge technique was effective in treating partial- or full-thickness GM tears in 15 patients. Chandrasekaran et al 5 reported similar results in a larger cohort of 34 patients. In our study, there were 65 patients with partial-thickness and 13 with full-thickness tears who underwent endoscopic repair. Outcomes of both groups, including the 6 additional patients with open full-thickness repairs, were compared, and similar results in PROs were noted. Additionally, the 2 groups returned to activity at similar rates. This demonstrates that patients with variable GM pathology can be adequately treated using endoscopic surgery and can return to their activity of choice after surgery.
Two systematic reviews comparing open versus endoscopic repair showed that both techniques result in similar improvements in PROs, pain scores, and abduction strength, with open repairs having a higher complication rate, including increased retear rate. 1,6 The majority of patients (93%) in our study underwent an endoscopic repair. Two patients in the endoscopic cohort had a reoperation because of an atraumatic retear, while no patients who had an open repair had a retear. The sample size between these 2 cohorts was not sufficient enough to detect a difference; however, the retear rate in our entire active cohort was low. We suspect that possible poor tissue quality or biologic response in this older population led to the retear. Further research needs to be done to determine if there is a clinical difference between open and endoscopic repairs, as suggested by the aforementioned systematic reviews.
The calculation of MCID helps illustrate clinical improvement instead of just solely relying on statistical significance. A large percentage of our cohort achieved MCID for the mHHS, NAHS, and HOS-SSS, suggesting the clinical efficacy of both endoscopic and open GM repair. In this study, a unique MCID was calculated based on half the SD of preoperative scores. This distribution-based calculation, as described by Norman et al, 28 is based on a psychological and empirical foundation that most often represents the threshold of discrimination for changes in health-related quality of life. 28 An anchor-based calculation has also been described; however, it was unable to be used in this study, as not all patients answered an anchor question. There is no clear consensus on the best approach to determining MCID because of the various methods of its calculation. 7,34,37 Okoroha et al 29 calculated the MCID for mHHS and HOS-SSS after isolated endoscopic GM repair using the change in pre- and postoperative scores. For this reason, our values for MCID are smaller than what has been previously reported. Nevertheless, MCID is dependent on context, including patient characteristics, such as socioeconomic status, disease severity, or patient expectations; therefore, it should be unique to each study. 8,34,42
The strengths of this study include an analysis of a large cohort of active patients older than 50 years undergoing endoscopic or open GM repair with a minimum 2-year follow-up. The clinical utility of our results was established through a calculation of the MCID for the mHHS, NAHS, and HOS-SSS. Finally, multiple validated functional hip outcome scores, including the mHHS, NAHS, HOS-SSS, and iHOT-12, as well as the VAS for pain and patient satisfaction ratings, were used for evaluation.
Limitations
There are inherent limitations to this study. First, selection bias is possible because of the retrospective nature of this study. Second, 82.1% of patients underwent concomitant procedures with central and peripheral compartment pathology addressed. It may be conceivable that a significant portion of clinical improvement can be attributed to the heterogeneity in procedures, which possibly cofounds our results. Still, we believe it is useful from both a diagnostic and a therapeutic standpoint to treat all pathology accordingly to optimize clinical outcomes and avoid reoperation. Third, there was not a quantitative measurement of hip abduction strength before and after surgical repair. Fourth, these results may not be generalizable, as they are from a single institution with exclusivity toward hip preservation.
Conclusion
Active patients over the age of 50 years may benefit from endoscopic or open repair of GM tears, as the majority of patients in our cohort were able to return to their activity of choice. All measured PROs had significantly improved at a minimum 2-year follow-up, with high survivorship, satisfaction, and clinical effectiveness. Patients with partial-thickness tears compared with full-thickness tears and those who underwent isolated GM repair compared with GM repair with concomitant procedures had similar return to activity rates and PROs at the latest follow-up.
Footnotes
Final revision submitted June 12, 2020; accepted June 30, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.B.M. has received educational support and hospitality payments from Arthrex, Stryker, and Smith & Nephew. P.J.R., J.S., and D.R.M. have received hospitality payments from Arthrex, Stryker, and Smith & Nephew. A.C.L. has received research support from Arthrex, Stryker, and Medacta; educational support from Medwest and Smith & Nephew; consulting fees from Arthrex and Graymont Medical; and hospitality payments from Arthrex, Smith & Nephew, Stryker, and Zimmer Biomet. B.G.D. has received research support from Arthrex, ATI, the Kauffman Foundation, Stryker, and Pacira Pharmaceuticals; educational support from Arthrex, Breg, and Medwest; consulting fees from Adventist Hinsdale Hospital, Arthrex, MAKO Surgical, Medacta, Pacira Pharmaceuticals, and Stryker; speaking fees from Arthrex and Pacira Pharmaceuticals; and royalties from Amplitude, Arthrex, DJO Global, MAKO Surgical, Medacta, Stryker, and Orthomerica and has had ownership interests in Hinsdale Orthopaedics, the American Hip Institute, SCD#3, North Shore Surgical Suites, and Munster Specialty Surgery Center. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Advocate Health Care (study ID: 5276).