
Abstract
Background:
Treatment of a first-time anterior shoulder dislocation (FTASD) is sensitive to patient preferences. The operative or nonoperative management debate provides an excellent opportunity to learn how surgeons apply patient preferences in treatment decisions.
Purpose:
To determine how patient preferences (repeat dislocation risk, recovery difficulties, fear of surgery, treatment costs) and surgeon factors influence a surgeon’s treatment plan for FTASD.
Study Design:
Cross-sectional study.
Methods:
Eight clinical vignettes of hypothetical patients with FTASD (including age, sex, and activity level) were presented to members of the Magellan Society. A second set of matched vignettes with patient preferences and clinical variables were also presented. The vignettes represented scenarios in which evidence does not favor one treatment over another. Respondents were asked how they would manage each hypothetical case. Respondents also estimated the risk of redislocation for the nonoperative cases for comparison with the published rates. Finally, respondents completed a Likert-scale questionnaire to determine their perceptions on factors influencing their decisions.
Results:
A total of 103 orthopaedic surgeons completed the survey; 48% practiced in an academic hospital; 79% were in practice for 10 years or longer; and 75% had completed a sports medicine fellowship. Patient preferences were the single most important factor influencing treatment recommendation, with activity type and age also important. Just 62% of the surgeon estimates of the risk of redislocation were consistent with the published rates. The inclusion of patient preferences to clinical variables changed treatment recommendations in 62.5% of our hypothetical cases. Respondents rated patient treatment preference as the leading factor in their treatment decision making.
Conclusion:
Patient preferences were important when deciding the appropriate treatment for FTASD. Respondents were inconsistent when applying evidence in their decision making and estimates of recurrent instability. Decision support tools that deliver patient preferences and personalized evidence-based outcome estimates improve the quality of decision making at the point of care.
Shoulder dislocations are among the most common injuries with an annual incidence of 11.2 per 100,000 and an estimated prevalence of 2% to 8% in the general population. 1,7 The optimal treatment of a first-time anterior shoulder dislocation (FTASD) remains heavily debated. The 2 main options for initial treatment are operative stabilization and nonoperative rehabilitation with physical therapy and activity modification. 7 The treatment dilemma is in part because of the wide range of reported risks of recurrent dislocation, from 14% to 100%, depending on age, sex, activity, and amount of glenoid bone loss. 2,4,11,13
There has been much work in determining risk factors in a patients’ profile that may influence the rate of a redislocation that may steer treating surgeons to recommend early operative management. 8 In addition, the treatment decision for an FTASD is preference sensitive—in other words, the evidence level 1 and 2 studies have not shown a single treatment to be clearly effective and thus the appropriate decision is driven by patient preferences for risks and benefits of the potential treatments. We have previously measured and characterized patient preferences for treatment of an FTASD, 12 but it is largely unknown how surgeons might utilize patient preferences in their decision making.
Another component of supporting preference-sensitive decision making involves providing accurate evidence-based information on risks and benefits that are most important to patients. We previously demonstrated that risk of a recurrent dislocation is the most important factor influencing a patient’s treatment decision for an FTASD. 12 Evidence level 1 and 2 studies have produced patient-specific estimates for this outcome. 7,10,11 However, the accuracy of the information surgeons might relay to patients is unknown.
The primary purpose of this study was to determine how patient preferences (concern about repeat dislocation, concern about difficulties with rehabilitation and recovery, fear of surgery, and financial cost of treatment) influence an orthopaedic surgeon’s treatment recommendations for FTASD. A secondary objective was to understand the accuracy of surgeon estimates at the individual patient level for the risk of recurrence after an FTASD.
Methods
Study Population
This study was determined to be exempt from institutional review board approval. The study population was made up of the members of the Magellan Society, an international society of orthopaedic sports medicine surgeons trained in various aspects of sports medicine including the management of shoulder injuries (N = 365). Members are past traveling fellows and the guiding godparents who had been preselected by their parent sports medicine societies of North America (American Orthopaedic Society for Sports Medicine [AOSSM]), Europe (European Society for Sports Traumatology, Knee Surgery and Arthroscopy [ESSKA]), the Pacific Region (Asian Pacific Orthopaedic Association [APOA]), and South America (Sociedad Latinoamericana De Artroscopia [SLARD]). The traveling fellowship programs are an annual scientific and cultural exchange among orthopaedic sports medicine physicians in North America, Europe, the Pacific Region, and South America. To obtain provider preferences of both the national (US) and international communities, the survey was sent to all active members of the Magellan Society. All meetings occur in English, and members have a good command of the English language. The Society maintains no specific data regarding the practice patterns of its members. While there were no exclusion criteria, members for whom shoulder surgery was not a large part of their practice were expected to self-select and choose not to participate.
Survey Instruments
Clinical Vignettes
We began by creating clinical vignettes to stimulate clinical decision making for fictitious patients with an FTASD. A small panel of orthopaedic surgeons with fellowship training in sports medicine (n = 3) iteratively reviewed and refined the clinical vignettes. Six orthopaedic surgeons were sent a preliminary version of the survey for review and testing. In constructing the patient preference profiles for the vignettes, a predictive model of shoulder instability after FTASD was used to create balanced preference graphs. Using Markov modeling via a Monte Carlo simulation, 9 the benefits of surgical and nonsurgical intervention were predicted per vignette to establish balanced profiles that did not strongly support either operative or nonoperative management in an effort to better assess the effect of patient preferences on provider recommendations. Additional experts (n = 2), each with >20 years of experience in consumer and health services research, assisted in survey preparation, design, and analysis.
A series of 16 patient vignettes was developed to understand how surgeons evaluate hypothetical patients and which patient characteristics are important in treatment recommendations. The first 8 vignettes laid out clinical data including age, sex, and activity level. An orthogonal design was employed to balance patient characteristics of age, sex, and sports activity associated with higher and lower risks of shoulder dislocation after treatment of FTASD. The patient characteristics of each vignette were defined as binary variables: older versus younger patients, men versus women, and contact sports or sports with heavy use of the upper extremity versus other sports and activities (Table 1). Age ranges were selected to eliminate possibility of overlap. These vignettes have been used in a previous study. 6
Variables Used to Create Vignettes of Hypothetical Patient Situations After First-Time Anterior Shoulder Dislocation

The second 8 vignettes included the clinical data as well as patient preferences. Patient preferences were arbitrarily mapped for each attribute on a scale from 0 to 100. Scores were categorized into a low (10-40) or high preference (60-90) estimate per attribute. The 4 attributes were (1) concern about repeat dislocation, (2) willingness to stop high-risk activities without surgery because of fear of surgery, (3) concern about difficulties with surgery or recovery, and (4) financial cost of treatment. Patient preferences for the second set of 8 patient vignettes (numbers 9-16) were also presented as a graphical depiction of each factor’s importance to the patient in each vignette. An example of 2 comparable vignettes (1 with and 1 without patient preferences) is provided in Table 2. All 16 case vignettes are available in Appendix Table A1.
Sample Vignettes

Physician Questionnaire
A second questionnaire was developed to understand the role of various patient factors (age, sex, and participation in activities; Table 1) and patient preferences (Table 2) in each respondent’s treatment recommendations. Responses were graded on a 5-point Likert scale from 1 (not important) to 5 (extremely important) or fixed-choice responses. Respondents were asked 4 questions on how important they believed each factor was to patients in their current practice. They were also asked to estimate the time they would spend discussing treatment alternatives. Finally, to understand possible routes of implementation, respondents were asked whether they thought patient preferences were important in general, whether the graphic representation was helpful, and whether they would recommend preference collection in their practice. The full questionnaire contained 8 questions.
Study Approach
Once the format and content of the vignettes and physician survey were finalized, we contacted (via email) all members of the Magellan Society with an invitation to participate. In this invitation was a link to REDCap (Vanderbilt University), an electronic data-capture tool in which participants gave their consent to participate and then entered characteristic and practice information, reviewed and responded to all 16 vignettes, and then completed the questionnaire about the role(s) of patient preferences in clinical decision making. Institutional data protection measures ensured respondent confidentiality and data security. 3
For each vignette, the respondents were asked to recommend operative versus nonoperative treatment. For the vignettes in which the respondents recommended nonoperative treatment, they were also asked to estimate the risk of repeat dislocation in the subsequent 2 years using a fixed response list (<15%; 15%-29%; 30%-44%; 45%-59%; 60%-75%; >75%). Respondents’ estimated rates of redislocation for each vignette were compared with the age- and sex-specific rates presented by Robinson. 10 The respondent’s choice was considered to be accurate if the age- and sex-specific risk of redislocation from Robinson was within the chosen category plus or minus 1 category.
Statistical Analysis
Descriptive statistics were used to summarize the characteristic data of the provider population. Treatment recommendations were compared between vignette cohorts including and excluding patient preferences. Estimates of rates of repeat dislocation after nonoperative treatment were compared with the published rates in the literature to gauge accuracy. 10 The Fisher exact test was used to compare treatment recommendations (operative vs nonoperative) for each of the 8 paired vignettes (vignette 1 vs vignette 9, vignette 2 vs vignette 10, etc.). Logistic regression was used to determine which patient characteristics or patient preferences were most important in treatment recommendations (operative vs nonoperative) for the entire group of respondents as well as for various characteristic subgroups of respondents (US vs international, <10 years of experience vs ≥10 years of experience, etc.). Predictor variables assessed included age, sex, high-risk behavior, concern about repeat dislocation, likelihood of activity modification, concern about cost, and concern about surgery and recovery. Statistical significance was set at P ≤ .05.
Results
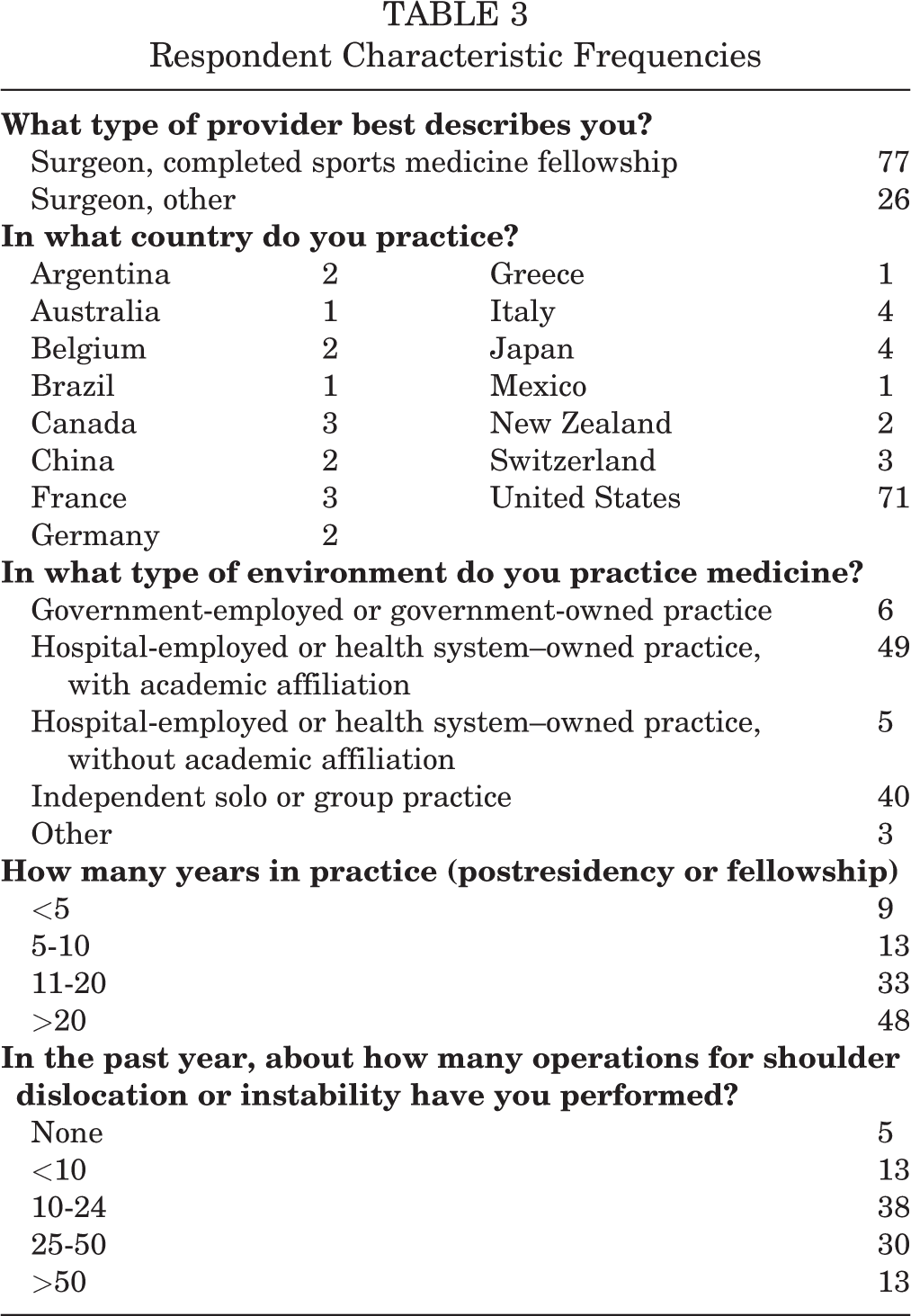
In total, 103 (28%) members of the Magellan Society completed the survey. Of our respondents, 75% had fellowship training; 69% practice in the United States; 48% practice in academic hospital or health system settings; 79% reported being in practice, not including residency or fellowship, for 10 years or longer; and 83% perform operative shoulder stabilization more than 10 times per year. See Table 3 for a summary of participant characteristics.
Respondent Characteristic Frequencies
Vignettes
As stated, participants read each of the vignettes and then made a decision regarding treatment (surgical or nonsurgical). For the vignettes in which nonsurgical treatment was recommended, the respondents were asked to estimate the risk of recurrent instability. Nonoperative management was recommended by 72% of the respondents when patient preferences were not presented and by 66% when patient preferences were presented. Table 4 summarizes the responses of the participants.
Summary of Participant Responses to the Vignettes a
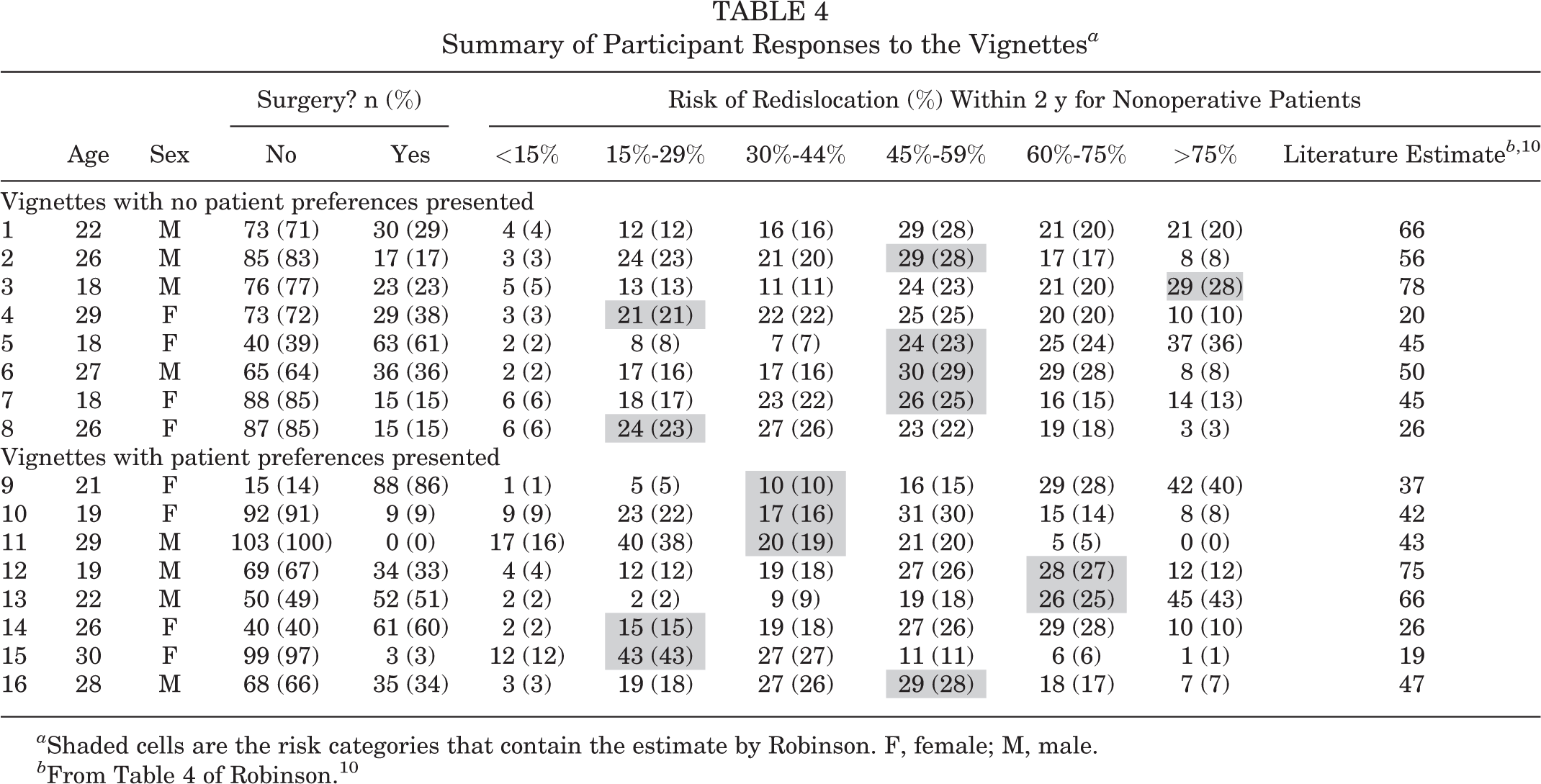
a Shaded cells are the risk categories that contain the estimate by Robinson. F, female; M, male.
Provider Estimates of Risk of Recurrent Dislocation
When asked to estimate the expected rate of recurrence of a shoulder dislocation based on information in the vignettes, respondent estimates were accurate 62% of the time. Additionally, there was no difference in estimations of risk of recurrence based on years in practice (≥10 years vs <10 years in practice; P = .814). Non-US surgeon estimates of rate of recurrence were slightly better than estimates made by US surgeons (61.5% vs 58.4%); however, this difference was not significant (P = .317). There were no differences in estimated time to recurrent injury for the other 3 characteristic factors.
Point decreases in predicted recurrence rates were driven most by age (Table 5). For example, the estimated recurrence rate for a case of a patient older than 30 years of age was estimated by the respondents to be a mean of 11.6 percentage points lower than that reported in the literature.
Percentage Point Difference in Recurrence Estimate From Patient Information a
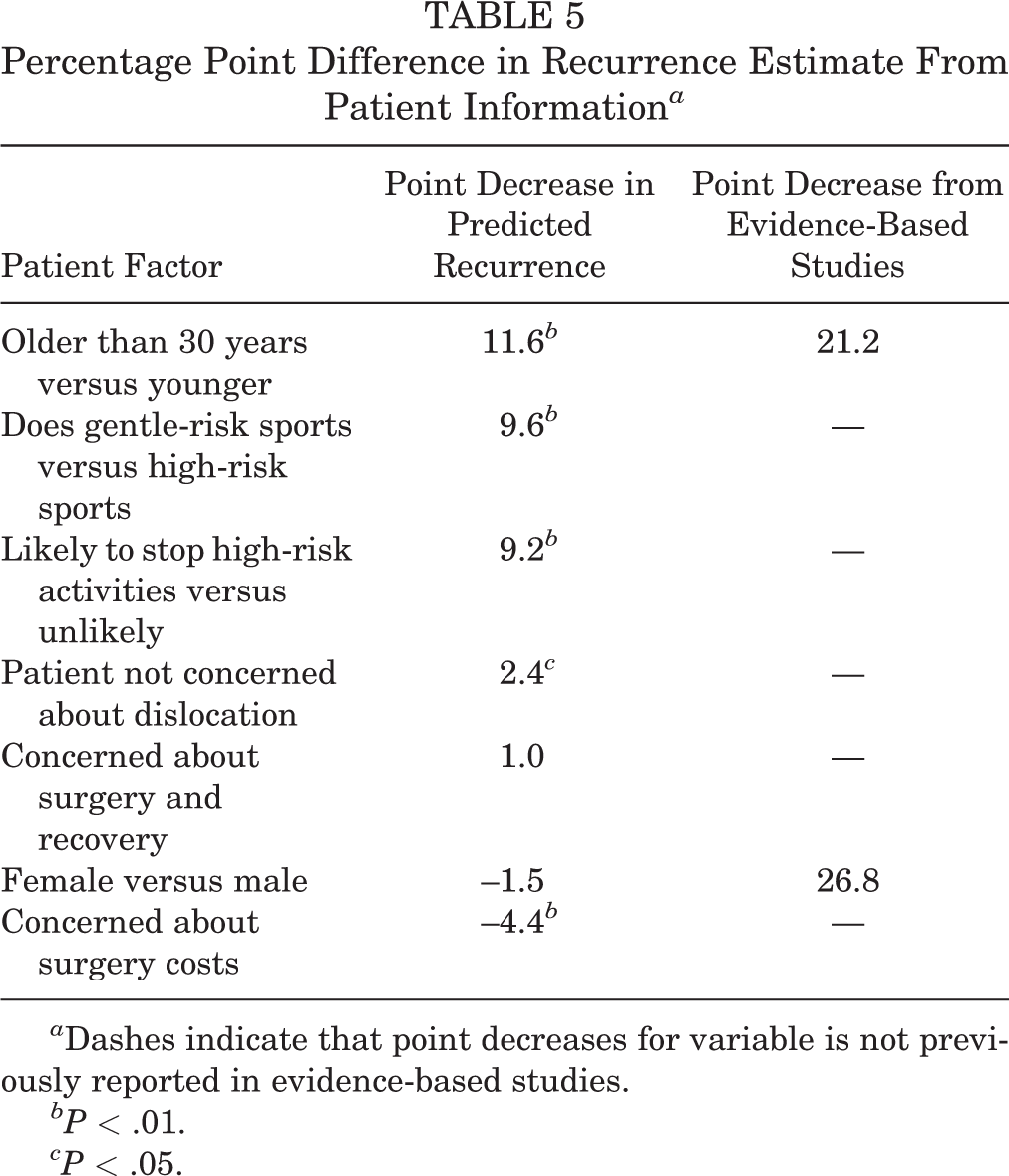
a Dashes indicate that point decreases for variable is not previously reported in evidence-based studies.
b P < .01.
c P < .05.
Factors Favoring Operative Treatment
Two factors seemed to be predictive of a recommendation for surgery: High-volume surgeons (≥25 shoulder stabilization operations in the past year) recommended operative treatment at significantly higher rates than their lower-volume peers (B = 0.130; SE = 0.42; beta = 0.292; t = 3.064; P = .003), and operative treatment was more often recommended by respondents who stated that clinical factors (ie, age, sex, high-risk activities) were important (B = 0.47; SE = 0.21; beta = 0.211; t = 2.258; P = .026).
Factors Favoring Nonoperative Treatment
Three factors appeared to be predictive of a recommendation for nonoperative treatment: Low-volume surgeons (<10 surgeries in the previous year; B = 0.046; SE = 0.024; beta = 0.188; t = 1.919; P = .058), surgeons who thought patient preferences were important (B = −0.048; SE = 0.022; beta = −0.213; t = −2.147; P = .034), and those with <10 years of experience (B = 0.044; SE = 0.026; beta = 0.162; t = 1.728; P =.087) were most likely to recommend nonsurgical management. In addition, surgeons who acknowledged both the patient’s concern about surgery and recovery and the patient’s desire to avoid repeat dislocations was important favored nonoperative treatment (B = −0.031; SE = 0.011; beta = −0.277; t = −2.892; P = .005).
Importance of Patient Preferences
A comparison of matched vignettes from the 2 groups of vignettes in terms of age, sex, and activity level showed that the inclusion of preference information changed treatment recommendations in 62.5% of our hypothetical cases. As stated earlier, nonoperative treatment was recommended by 72% of the respondents. The inclusion of patient preferences reduced this recommendation to 66% of the respondents. When matched vignettes were reviewed, the inclusion of patient preferences resulted in a change in the treatment recommendation in 5 of the 8 pairs of vignettes (62.5%). The inclusion of patient preferences resulted in 3 vignettes (60%) where the recommendation of nonoperative treatment changed to surgical treatment. The recommendation was reversed in the other 2 (40%) vignettes. Respondent characteristics played little role in changing the surgeon’s decision about treatment (Table 6).
Percentage of Respondents Who Changed Their Treatment Recommendation Based on Patient Preferences by Respondent Characteristics

Comparison of US Versus Non-US Surgeons
In comparison with international-based surgeons, US surgeons were more likely to think patient feelings about the financial cost of treatment were important when recommending treatment (P < .001) and indicated that financial costs were an important factor to their patients (P < .001). US surgeons were also more likely to think that patient preferences are important when recommending treatments (P < .001). There was no difference in the rate of operative versus nonoperative recommendations between the 2 cohorts (P = .148).
Physician Questionnaire
Table 7 summarizes the responses to the physician questionnaire. Overall, the majority of respondents agreed or strongly agreed about the importance of patient preferences when recommending treatments (90%), the helpfulness of a graphical representation of patient preferences (58%), and the recommendation of patient preferences in their practice (56%). The graphic representation of the patient preferences was favored mostly by surgeons with fellowship training (60% vs 46%) and by surgeons practicing outside of the US (65% vs 52%). Those who desired additional patient preferences were surgeons concerned with the probability of a repeat dislocation (B = 0.543; SE = 0.083; beta = 0.546; t = 6.546; P < .001) and those taking more than 10 minutes to discuss treatment decisions with their patients (B = 0.348; SE = 0.165; beta = 0.173; t = 2.105; P = .038).
Respondent Answers to Importance Rating and Reflection Questions
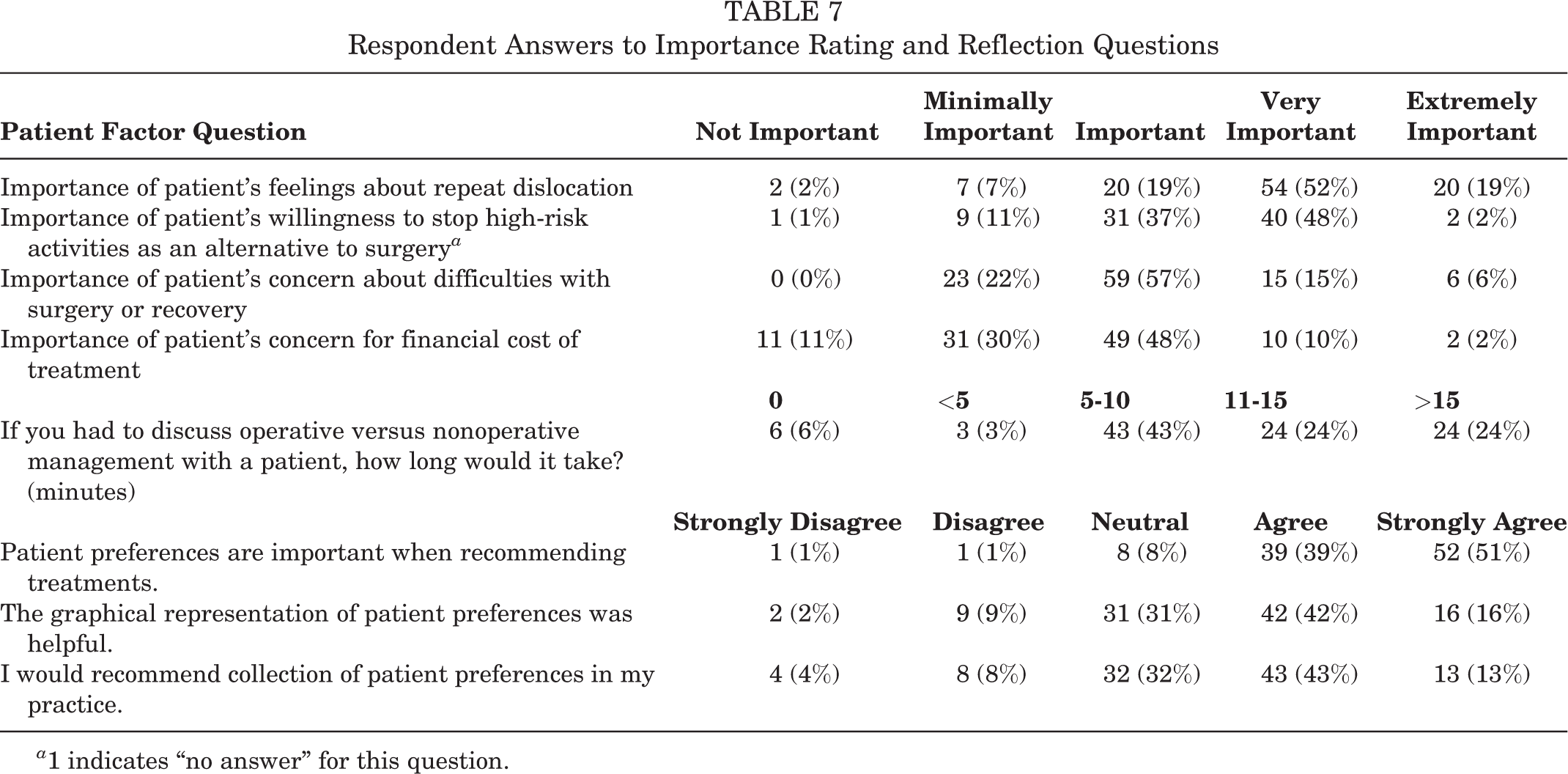
a 1 indicates “no answer” for this question.
Factors Influencing Treatment Recommendations
Patient treatment preferences were the most important single factor influencing treatment recommendation followed by clinical measures, specifically high-risk behavior and age (Table 8). Sex and patients’ concerns about costs were the least important factors for surgeons in making a treatment recommendation.
Means (and SDs) of Factors Physicians Considered Most Important in Making Treatment Recommendations for Patients With First-time Anterior Shoulder Dislocation a

a Values are based on a 5-point Likert scale (1 = not important, 5 = extremely important).
Physicians were more likely to find the top 3 factors (patient’s treatment preference, high-risk behavior, and age) important if the respondent (1) practiced in the United States, (2) considered the patient preference graph helpful, (3) performed ≥25 shoulder instability surgeries per year, (4) recommended more surgeries, or (5) believed that many factors lead to greater likelihood of another dislocation.
Discussion
We were curious about whether patient concerns would have an impact on treatment recommendations for patients with FTASD. We presented a series of hypothetical patient vignettes, with or without patient preferences, to shoulder specialists and asked for their recommendation of surgical or nonsurgical treatment. The inclusion of patient preferences to clinical variables changed treatment recommendations in 62.5% of cases. This study also found that surgeon estimates on the rate of recurrence of redislocation were accurate 62% of the time when compared with the published literature. 10
In our study, surgeons preferred a shared decision-making model for treatment recommendations. For the patient, the most important considerations were concern about repeat dislocation, concern about length or difficulty of rehabilitation and recovery, fear of surgery, and financial cost considerations. Overwhelmingly, surgeons agreed on the importance of patient preferences (90%) as well as the usefulness of the graphical representation of patient preferences (58%). The addition of patient preferences changed treatment recommendations in over half of cases. When patient preferences were considered by surgeons, their recommendation changed in 60% of the cases with tendency toward recommending surgery more.
Hutyra and colleagues 6 recently reported that the most influential factor in a patient’s decision for surgery was the risk of repeat dislocation. The patient’s concern about repeat dislocation was heavily influenced by the surgeon’s accurate portrayal of the potential risks. The current study found that surgeons were accurate only 62% of the time. Moreover, Hutyra et al 6 also noted that surgeons tended to overstate the recurrence rates. This finding suggests that surgeons may not be relaying an accurate representation of the most critical aspect of a patient’s decision making. Interestingly, we found no meaningful differences in estimations of the risk of recurrence based on any characteristic. For example, surgeons who were in practice <10 or ≥10 years were equally as likely to provide inaccurate recurrence rates.
In contrast, the factor that led most surgeons to decrease their predicted recurrence rate was age. For example, in vignettes with patients over 30 years of age, respondents estimated the risk of recurrence to be 11.6 percentage points below literature estimates. These findings are supported by the systematic review and meta-analysis by Olds and colleagues, 9 who reported age to be the largest contributor to risk of recurrence. Their summary showed that patients 40 years of age and younger were 13.46 times more likely to have a recurrent dislocation than patients older than 40 years of age. Our data showed that activity level in a patient’s recreational activities was the second largest contributor to changes in a surgeon’s predicted recurrence rate. This importance of activity level is also supported by previous studies. 10,11 Our data suggest that surgeons are well informed on which factors strongly influence the risk of recurrence, but knowing those factors may not accurately reflect the degree to which these affect the risk when counseling patients.
Other factors may influence a surgeon’s recommendation for surgery. For example, we found that surgeons with a higher volume of shoulder stabilization operations (>25 per year) were more likely to recommend operative treatment. In other words, the more surgeons were comfortable performing a surgery, the more likely they would recommend surgery. This finding is not unexpected but serves as a reminder to clinicians of this inherent bias.
The country of practice also appeared to affect treatment recommendations. The United States follows a fee-for-service model that may have led US surgeons to be more concerned with the financial considerations in their decision making versus their non-US counterparts from countries that provide a universal medical care system. Similarly, US surgeons weighed patient preferences more strongly than their international colleagues, which may also reflect sensitivity to a shared decision-making model or to the higher malpractice risk environment.
In a clinical setting, a physician should be aware of his or her own biases. A bias toward surgery may lead surgeons to cite higher rates of redislocation to their patients than are reflected in evidence-based studies. This may influence the patient’s decision to undergo surgery to decrease the risk of redislocation, which this study found is the largest factor in determining a treatment option. A possible solution is the use of clinical decision support (CDS) tools.
These findings suggest that the application of tools to measure and deliver patient preferences, combined with evidence-based risk of recurrence, could benefit both providers and patients in optimizing individualized treatment.
CDS tools, such as predictive models or decision aids, could be used to help mitigate biases and accurately disseminate evidence-based rates of recurrence while incorporating patient preferences. 5,12 For example, after a history and physical examination which indicates a diagnosis of FTASD then before a discussion of treatment options, the patient may be asked to complete a survey about his or her characteristics and treatment preferences. The results from this survey could then be used to estimate the recurrence risk while displaying patient preferences in a graphical format (see Table 2) for the surgeon to review with the patient. This technology can help patients review the latest evidence-based recommendations, limit surgeon bias, and serve as a starting point for discussion regarding benefits and risks of operative and nonoperative treatment. 5,9,12 Our study suggests that application of tools to measure and deliver patient preferences combined with evidence-based risk of recurrence could benefit both providers and patients in optimizing individualized treatment. Overall, CDS tools can serve as a method to improve communication and enhance outcomes. 5,9,12
There were several limitations of this study. For example, limited information was contained within each case study. In a clinical setting, clinicians will obtain additional information that may influence the ultimate treatment recommendation. Further, each of these case studies presented a hypothetical example. Clinician-stated responses may not mirror actual treatment recommendations in a clinical context. The respondents were primarily shoulder specialists, many of whom had fellowship training, which may lead to differences from other orthopaedic surgery subspecialties or other medical disciplines. Our results do not account for other potential characteristic groupings beyond the 5 we gathered and may not be generalizable to the non--shoulder specialist who could well have far less experience with the shoulder. Finally, this survey was built using an orthogonal rather than an adaptive design. This limited the information obtained from each case study.
Conclusion
Our data show that patient preferences influence treatment decisions for patients with FTASD, particularly patient treatment preference, high-risk behavior, and age. When presenting an estimated recurrent injury rate to a patient, surgeons use their own clinical experience, the medical literature, and their own biases. Our data show that surgeon estimates of a recurrent injury are in line with the published literature, being accurate only 59% of the time. These findings suggest that the application of tools to measure and deliver patient preferences combined with evidence-based risk of recurrence could benefit both providers and patients in delivering the optimal individualized treatment.
Footnotes
Acknowledgment
The authors acknowledge Donald T. Kirkendall, ELS, a contracted medical editor, for his assistance in preparing the manuscript for submission.
Final revision submitted May 22, 2020; accepted June 15, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.C.L. has received educational support from Smith & Nephew and SouthTech Orthopedics and research support from Arthrex. B.S. has received educational support from MVP Orthopedics. D.C.T. has received consulting fees and royalties from DePuy/Medical Device Business Services. R.C.M. has received consulting fees from Stryker and hospitality payments from DJO, RTI, and Trice Medical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by Duke University (protocol No. Pro00049685).
Appendix
The 16 Case Vignettes Used in This Study

| Vignette Number | Description | Preferences a (Low, 10-40; High 60-90) |
|---|---|---|
| 1 | A 22-year-old man presents after the first dislocation of his shoulder. He swims regularly, often 5 times per week. | N/A |
| 2 | A 26-year-old man presents after dislocating his shoulder for the first time. He plays soccer (international: football) recreationally, usually 3 times per week. | N/A |
| 3 | An 18-year-old man presents after dislocating his shoulder for the first time. He does not regularly participate in sports. | N/A |
| 4 | A 29-year-old woman presents after dislocating her shoulder for the first time. She plays ice hockey actively, usually 3 times per week or more. | N/A |
| 5 | A right hand–dominant 18-year-old woman presents after dislocating her right shoulder for the first time. She plays badminton competitively and trains and practices ≥4 times per week. | N/A |
| 6 | A 27-year-old man presents after dislocating his shoulder for the first time. He plays water polo recreationally, about 3 times per week. | N/A |
| 7 | An 18-year-old woman presents after dislocating her shoulder for the first time. She exercises at the gym occasionally and does not participate in other sports. | N/A |
| 8 | A 26-year-old woman presents after the first dislocation of her shoulder. She plays soccer (international: football) in a recreational league 3 times per week. | N/A |
| 9 | A 21-year-old woman presents after the first dislocation of her shoulder. She plays rugby competitively at least 3 times per week. | Repeat dislocation (high), stop high-risk activities (low), concern with surgery/recovery (low), cost (low) |
| 10 | A 19-year-old woman presents after the first dislocation of her shoulder. She plays golf regularly, about 4 times per week. | Repeat dislocation (low), stop high-risk activities (high), concern with surgery/recovery (high), cost (low) |
| 11 | A 29-year-old man presents after the first dislocation of his shoulder. He runs regularly for fitness and occasionally runs marathons. | Repeat dislocation (low), stop high-risk activities (high), concern with surgery/recovery (low), cost (high) |
| 12 | A 19-year-old man presents after the first dislocation of his shoulder. He attends a cycling class at the gym 4 or 5 mornings per week for exercise. | Repeat dislocation (high), stop high-risk activities (low), concern with surgery/recovery (high), cost (high) |
| 13 | A 22-year-old man presents after the first dislocation of his shoulder. He wrestles competitively and practices and trains 3 times per week. | Repeat dislocation (low), stop high-risk activities (low), concern with surgery/recovery (high), cost (high) |
| 14 | A 26-year-old woman presents after the first dislocation of her shoulder. She plays water polo regularly, about 3 times per week. | Repeat dislocation (high), stop high-risk activities (high), concern with surgery/recovery (low), cost (high) |
| 15 | A 30-year-old woman presents after the first dislocation of her shoulder. She does yoga and Pilates for fitness, usually every day of the week. | Repeat dislocation (high), stop high-risk activities (high), concern with surgery/recovery (high), cost (low) |
| 16 | A 28-year-old man presents after the first dislocation of his shoulder. He plays ice hockey actively, about 3 times per week. | Repeat dislocation (low), stop high-risk activities (low), concern with surgery/recovery (low), cost (low) |
a Patient preferences were mapped for each attribute in vignettes 9-16 on a scale from 0 to 100. Scores were categorized into a low (10-40) or high (60-90) preference estimate per attribute. Each vignette displayed 4 attributes: (1) concern about repeat dislocation, (2) willingness to stop high-risk activities without surgery, (3) concern about difficulties with surgery or recovery, and (4) financial cost of treatment. N/A indicates that preferences were not included in the first 8 vignettes per study design.