
Abstract
Background:
The stabilization of the femoral head is provided by the distal acetabulum when the hip is in a flexed position. However, the osseous parameters for the diagnosis of hip instability in flexion are not defined.
Purpose/Hypothesis:
To determine whether the osseous parameters of the distal acetabulum are different in hips demonstrating anteroinferior subluxation in flexion under dynamic arthroscopic examination, compared with individuals without hip symptoms. The hypothesis was that the morphometric parameters of the anterior acetabular horn are distinct in hips with anteroinferior instability compared with asymptomatic hips.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
A total of 30 hips with anteroinferior instability in flexion under dynamic arthroscopic examination were identified. A control group of 60 hips (30 patients), matched by age and sex, was formed from individuals who had undergone pelvis magnetic resonance imaging (MRI) for nonorthopaedic reasons. Unstable and control hips were compared according to the following parameters assessed on axial MRI scans of the pelvis: anterior sector angle (ASA), anterior horn angle (AHA), posterior sector angle (PSA), posterior horn angle (PHA), acetabular version, lateral center-edge angle, acetabular inclination (Tönnis angle), and femoral head diameter.
Results:
The coverage of the femoral head by the anterior acetabular horn was decreased in unstable hips compared with the control group (mean ASA, 54.8° vs 61°, respectively; P < .001). Unstable hips also had a steeper anterior acetabular horn, with an increased mean AHA compared with controls (52.5° vs 46.8°, respectively; P < .001). An ASA <58° had a sensitivity of 0.8, a specificity of 0.68, a negative predictive value of 0.87, and a positive predictive value of 0.56 for anteroinferior hip instability. An AHA >50° had a sensitivity of 0.77, a specificity of 0.72, a negative predictive value of 0.86, and a positive predictive value of 0.57 for anteroinferior hip instability. There was no statistically significant difference in the mean PSA, PHA, acetabular version, lateral center-edge angle, acetabular inclination, or femoral head diameter between unstable hips and controls.
Conclusion:
Abnormal morphology of the anterior acetabular horn is associated with anteroinferior instability in hip flexion. The ASA and AHA can aid in the diagnosis of hip instability.
The influence of the ligamentous structures has been the subject of research in most investigations on nontraumatic instability of the native hip in adults. ‡ The morphology of the acetabular dome has a fundamental role to hip stability. 1,13 In contrast, the influence of the distal acetabulum morphology on hip stability is usually ignored in orthopaedic literature. Biomechanical studies reported the importance of the distal acetabulum on stabilizing the femoral head, especially when the hip joint is flexed. 5,8,19,26 The edge of the posterior acetabular horn is reported as the area of maximum pressure during sitting down on a chair, 26 while the anterior acetabular horn has been described as the main osseous stabilizer when the hip is in flexion and abduction. 19
Three parameters are described to assess the morphology of the anterior and posterior horns of the acetabulum: sector angle, horn angle, and acetabular horn width. 2,9 The sector angle is reported to quantify the anterior and posterior acetabular coverage in the axial plane. 2 The acetabular horn angle and width were recently described in a cadaveric study to assess the anatomy of the distal acetabulum. 9
The purpose of this study was to determine whether the osseous parameters of the distal acetabulum were different in hips having anteroinferior subluxation in flexion under dynamic arthroscopic examination compared with a control group of individuals without hip symptoms. The hypothesis was that the morphometric parameters of the anterior acetabular horn were distinct in hips with anteroinferior instability in comparison with asymptomatic hips.
Methods
This case-control study was carried out in an urban academic tertiary care orthopaedic facility and approved by the hospital’s institutional review board. A retrospective review was performed in 413 patients (427 hips) who underwent hip arthroscopy during a 2-year period (between August 2017 and August 2019). The surgical reports were reviewed, and 30 hips (29 patients) unstable in flexion under dynamic intraoperative examination were identified. A control group including 2 controls per case (60 hips in 30 patients), matched by age and sex, was composed from individuals who performed pelvis magnetic resonance imaging (MRI) for nonorthopaedic reasons. Table 1 shows the characteristics of the unstable and control groups. After the groups’ formation, assessment of the acetabular parameters was performed in the MRI studies.
Patient and Imaging Characteristics of the Unstable and Control Groups

Dynamic Intraoperative Examination
The hip arthroscopic procedures were performed with the patient positioned supine on a traction table. Traction was applied, and the anterolateral and midanterior portals were utilized to access the hip joint. A transverse anterior capsulotomy of ≤3 cm in length was performed to communicate the anterolateral and midanterior portals. The central compartment was assessed for abnormalities in the ligamentum teres, acetabular labrum, and cartilage. Radiofrequency was utilized to debride or stabilize unstable fragments of the ligamentum teres or labrum. The traction was then released and a dynamic examination of the hip was performed. With the ipsilateral foot detached from the traction table, an assistant moved the hip into flexion (110°) with neutral rotation and neutral abduction/adduction. Next, the hip was brought into flexion in 45° of abduction, adding external rotation and internal rotation. In sequence, the hip was brought into flexion in 20° of adduction, adding internal rotation and external rotation. The degree of internal and external rotation was variable according to the mobility shown by the patient, primarily determined by the femoral torsion. Utilizing a 70° arthroscope positioned in the anterolateral portal during the hip mobilization, we assessed the joint stability through the limited anterior capsulotomy. When the femoral head and acetabulum were congruent throughout the hip mobilization, the hip was classified as stable. A hip was classified as unstable when subluxation of the femoral head was observed during the dynamic examination (Figure 1; see online Video Supplement). Subluxation was defined as a gap >3 mm between the femoral head and acetabulum with the hip flexed. The degrees of hip flexion, abduction/adduction, and rotation in which the subluxation occurred were recorded, as well as any maneuver leading to the relocation of the femoral head into the acetabulum. Acetabuloplasty, labral repair, and/or femoroplasty were performed when indicated after the dynamic arthroscopic examination. In sequence, a second dynamic examination was performed to assess the adequacy of the acetabuloplasty, femoroplasty, and labral repair.
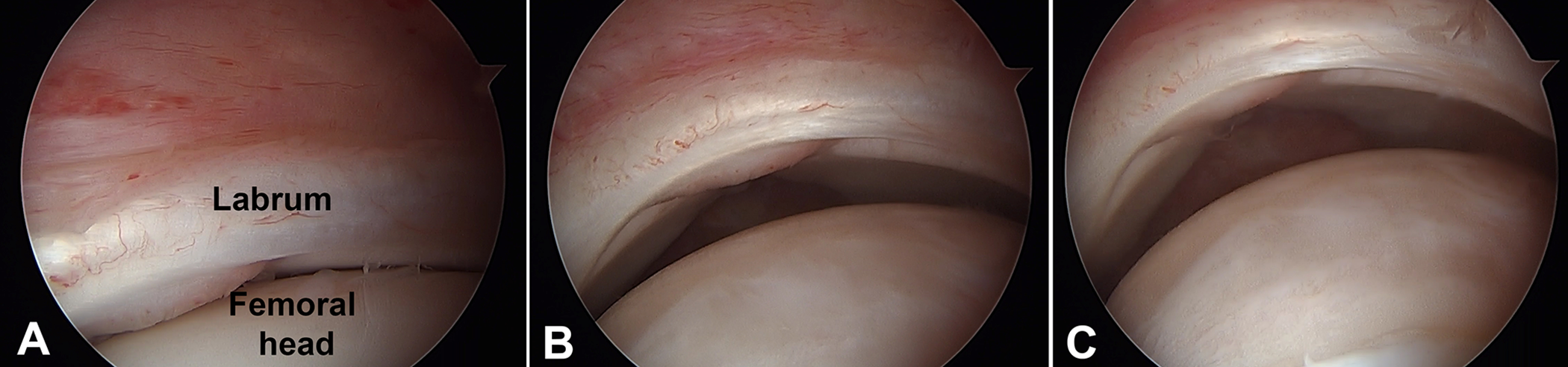
Arthroscopic view of the left hip through a limited capsulotomy demonstrating anteroinferior subluxation of the femoral head. (A) Starting position in 30° of hip flexion. (B) Loss of femoroacetabular congruence secondary to subluxation of the femoral head anteroinferiorly at 60° of flexion. (C) Hip flexion above 90° associated with abduction results in further anteroinferior displacement of the femoral head.
MRI Assessment
A fellowship-trained, board-certified hip surgeon (M.A.H.) screened the MRI studies and performed the imaging measurements while blinded to the stability status in all hips. The following parameters were assessed in axial plane images of the pelvis: anterior sector angle (ASA), posterior sector angle (PSA), anterior horn angle (AHA), posterior horn angle (PHA), acetabular version, femoral head diameter, anterior horn width, and posterior horn width 2,9 (Figure 2). These parameters were assessed in the axial cut 10 mm proximal to the distal limit of the anterior acetabular horn (Figure 3). In addition, the coronal image at the center of the femoral head was utilized to measure the lateral center-edge angle and acetabular inclination (Tönnis angle). 20 The femoral torsion was measured in unstable hips, considering that the MRI studies in the control group were performed for nonorthopaedic reasons and did not include a femoral torsion study.

Axial magnetic resonance of the pelvis demonstrating the acetabular measurements. (A) Anterior sector angle (ASA) and posterior sector angle (PSA). The blue line runs from the center of the femoral head to the edge of the anterior horn. The angle between the blue line and the coronal plane (yellow line) represents the ASA. The red line runs from the center of the femoral head to the edge of the posterior horn. The angle between the red line and the coronal plane represents the PSA. (B) Anterior horn angle (AHA) and posterior horn angle (PHA). The angle between the articular surface of the anterior horn (blue line) and the coronal plane (yellow line) represents the AHA. The angle between the articular surface of the posterior horn (red line) and the coronal plane represents the PHA. (C) Acetabular version, representing the angle between the sagittal plane (yellow line) and a blue line connecting the anterior and posterior limits of the acetabulum. (D) The femoral head diameter is represented by the yellow line. The anterior horn width is represented by the blue line, connecting the medial and lateral limits of the anterior horn of the acetabulum. The posterior horn width is represented by the red line, connecting the medial and lateral limits of the posterior horn of the acetabulum.
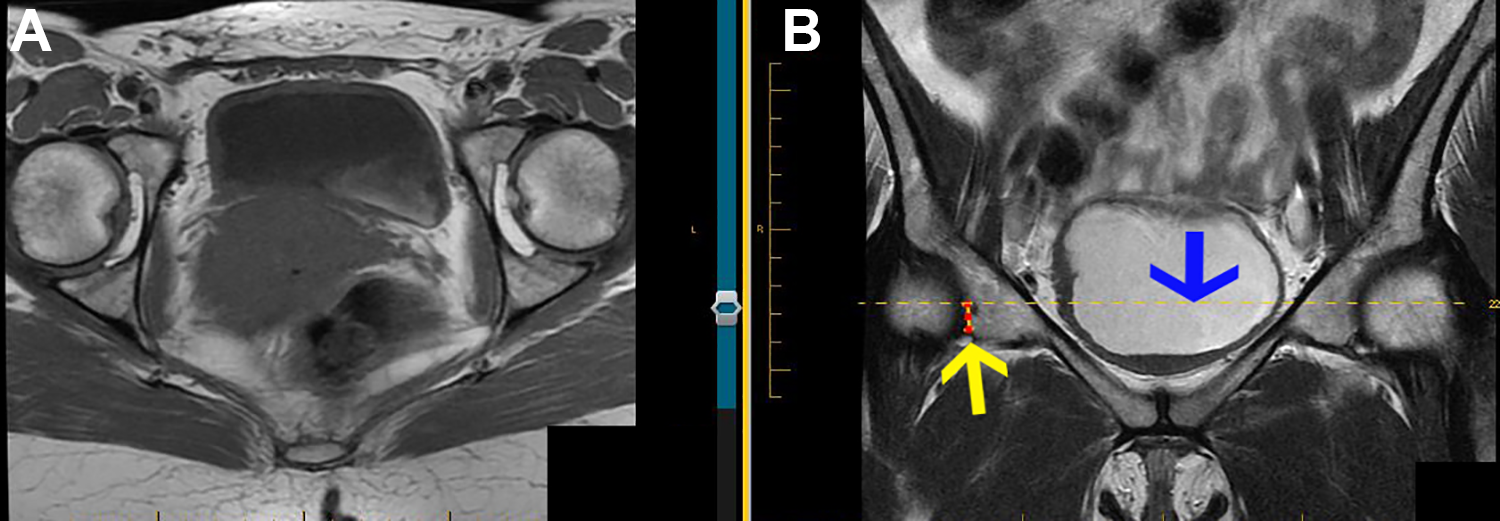
Determining the level of the axial slice at magnetic resonance to measure the inferior acetabular parameters in the right hip. (A) The axial slice chosen according to the coronal slice. (B) The coronal plane image was utilized to identify the distal limit of the anterior acetabular horn (yellow arrow). The axial slice chosen (A) was the slice closest to 10 mm proximal (blue arrow) to the distal limit of the anterior acetabular horn.
Statistical and Reliability Analysis
The normality of data distribution was confirmed utilizing the Kolmogorov-Smirnov test. Unpaired Student t tests were utilized to establish the significance of any noted differences, and P <.01 was considered significant. Pearson correlation coefficients were calculated to examine correlations between variables. The MRI assessments were tested for intra- and interrater reliability in 20 hips (10 hips randomly chosen from both the unstable and control groups). The intrarater reliability was determined based on a second measurement performed by the main investigator (M.A.H.) at least 30 days after the original measurement. The precision of measurement by a single observer (intrarater reliability) and that between observers (interrater reliability) were determined by calculating the 95% CI between the repeated measurements and their average (Table 2). The receiver operating characteristic (ROC) curve, area under the ROC curve, sensitivity, specificity, positive predictive value, negative predictive value, and optimal cutoff by the Youden index were calculated for the ASA and AHA using easyROC. 7
Intra- and Interrater Reliability of the Imaging Parameters a

a ICC, intraclass correlation coefficient.
Results
The mean coverage of the femoral head by the anterior acetabular horn was decreased in the 30 unstable hips (mean ASA, 54.8°; 95% CI, 52.4-57.2) in comparison with the 60 control hips (mean ASA, 61°; 95% CI, 59.4-62.6) (P < .001). Unstable hips also had steeper anterior acetabular horns, with a mean increased AHA (52.5°; 95% CI, 50.5-54.5) in comparison with the control group (46.8°; 95% CI, 45.1-48.5) (P < .001). The ASA and AHA had a strong inverse correlation in both the unstable group (r = –0.72) and the control group (r = –0.69). An ASA below 58° had a sensitivity of 0.8, specificity of 0.68, negative predictive value of 0.87, and positive predictive value of 0.56 for anteroinferior hip instability (Figure 4). An AHA above 50° had a sensitivity of 0.77, a specificity of 0.72, a negative predictive value of 0.86, and a positive predictive value of 0.57 for anteroinferior hip instability (Figure 5). Table 3 shows the area under the ROC curve, sensitivity, specificity, positive predictive value, negative predictive value, and optimal cutoff point for the ASA and AHA.

Anterior sector angle (ASA) receiver operating characteristic (ROC) curve and data distribution in the unstable and control hips.

Anterior horn angle (AHA) receiver operating characteristic (ROC) curve and data distribution in the unstable and control hips.
Performance of the Anterior Sector Angle and Anterior Horn Angle for Anteroinferior Hip Instability a

a ROC, receiver operating characteristic.
Regarding the posteroinferior acetabular parameters, there was no statistically significant difference in the mean PSA (P = .17) or PHA (P = .22) between the unstable group and the control group. The mean acetabular version in unstable hips was not significantly different from the mean observed version in the control group (P = .16). Table 4 summarizes the imaging findings for the unstable and control groups.
Magnetic Resonance Parameters in Hips With Anteroinferior Instability and Control Group a

a Data are reported as mean ± SD (95% CI).—, not assessed.
b Femoral torsion was available only to measure in unstable hips.
Anteroinferior subluxation of the femoral head started at 60° of hip flexion in 65% of the 30 unstable hips during the dynamic arthroscopic examination. Instability starting beyond 80° of hip flexion was observed in 25% of the hips. A labral tear was found in all 30 unstable hips at surgery. In 7 hips (23%), part of the labrum was not in contact with the femoral head and healed proximally to its anatomical base at the acetabular rim, as shown in Figure 1. A ligamentum teres tear was observed in 21 hips (70%), with complete tear observed in 1 hip (3%). Acetabuloplasty was performed in 73% of the hips, femoroplasty in 83% of the hips, and labral repair in 83% of the hips. Two hips (7%) underwent psoas tenotomy at the level of the labrum, 1 hip underwent capsular plication, and 1 hip underwent lesser trochanter plasty. Improvement in hip stability was observed in 46% of the hips after the acetabuloplasty and/or femoroplasty.
Discussion
This study aimed to identify whether the morphology of the anterior acetabular horn is associated with anteroinferior hip instability in flexion. The results indicate that unstable hips have a significantly lower ASA of 54.8°, compared with 61° in age- and sex-matched controls. In addition, unstable hips had more inclined anterior horns (AHA, 52.5°) compared with matched controls (AHA, 46.8°).
The interpretation of the ASA is similar to the center-edge angle of Wiberg 25 measured at the acetabular dome, in which increased angles represent increased coverage and stability (Figure 6). Rather, the AHA is interpreted as the acetabular inclination (Tönnis angle), in which increased angles represent a more open and less stable acetabulum (Figure 7). The ASA and AHA had a strong correlation in the present study. This correlation is similar to the observed in patients with acetabular dysplasia in regard to the parameters of the acetabular roof, in which a decreased center-edge angle is usually associated with increased acetabular inclination. Considering that the acetabulum is usually congruent to the femoral head, differences in the femoral head diameter could influence the AHA and PHA. However, the mean diameter of the femoral head in unstable hips was not different from that in the control group (Table 4). The negative predictive values for the ASA and AHA, 0.87 and 0.86, respectively, were considerably higher than the positive predictive values, 0.56 and 0.57, respectively (Table 3). Therefore, the ASA and AHA are better to rule out anteroinferior instability than to rule it in. In other words, a decreased ASA and excessive AHA are necessary to anteroinferior hip instability, but not enough to cause instability. In that context, the teres ligament function should be considered a stabilizer when the hip is in flexion and may compensate osseous deficiencies. 14

Axial magnetic resonance of the pelvis illustrating the anterior sector angle (ASA), which measures the anteroinferior coverage of the femoral head. (A) Hip (right side) with anteroinferior instability observed arthroscopically, with decreased ASA. (B) Normal ASA in an asymptomatic individual.
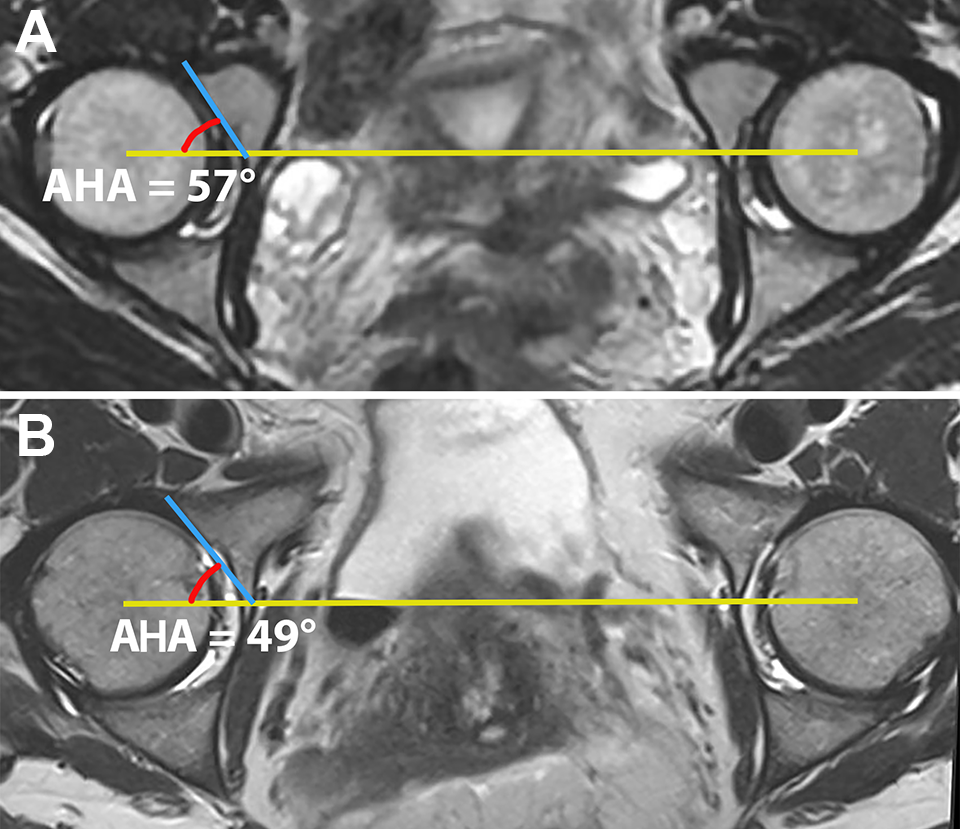
Axial magnetic resonance of the pelvis illustrating the anterior horn angle (AHA), which measures the inclination of the anterior acetabular horn. (A) Hip (right side) with anteroinferior instability observed arthroscopically, with increased AHA. (B) Normal anterior sector angle in an asymptomatic individual.
Of the 29 patients with unstable hips, 25 (86%) were women. This sex disparity is likely multifactorial. The mean acetabular version is reported to be increased in women in comparison with men. 2,9,21 The mean acetabular version of 19° for female patients and 16° for male patients was not significanlty different in the present study. The original studies on the ASA and AHA did not report a significant difference between male and female hips. 2,9 The higher prevalence of unstable hips in women can also be explained by the ligamentous structures, since the prevalence of joint hypermobility is significantly higher in female patients. 17 The stabilization effect of the musculotendinous structures can also explain the sex disparity for hip instability, considering the increased muscular composition of males.
The adult hip joint is considered by many authors to be an intrinsically stable joint because of its ball-and-socket configuration. 6 However, other authors consider the adult hip joint to not be intrinsically stable as it depends on the ligamentous structures. 3,4,10,12,24 Compared with other joints, the diagnosis of hip instability is challenging because of the volume of muscular structures surrounding the hip joint and the consequent difficulty in detecting the dislocation of the femoral head during the physical examination. Hoppe et al 10 reported criteria for the intraoperative diagnosis of hip instability with the hip in extension, according to the response of the hip joint to distraction and the pattern of ligamentum teres, labrum, and chondral damage. The dynamic testing performed in our study involved testing the hip in flexion with variable abduction/adduction and internal/external rotation and was performed before the acetabuloplasty, labral repair, and femoroplasty. A 3-cm anterior transverse capsulotomy without violation of the orbicular ligament was utilized for visualization. The capsulotomy could be considered a factor to cause intraoperative instability in our patients; however, the anterior capsule is loose and does not contribute to hip stability when the hip is in flexion. Cadaveric studies testing the distinct scenarios of capsular release in acetabula with stable and unstable anterior horn morphology may provide further clarification on the contribution of the capsular ligaments to the hip stability in flexion, particularly the role of the capsular ligaments in cases of decreased ASA and increased AHA.
The femoral torsion could not be assessed in the control group. However, the orientation of the femoral neck in the axial plane can influence the positions of hip stability. Decreased femoral torsion directs the femoral head anteroinferiorly when the hip is in abduction and flexed above 90°, as the contact between the femur and the proximal acetabulum lead to a levering mechanism. 23 Increased femoral torsion is associated with anterior instability, particularly when the hip is in an extended position. The orientation of the acetabulum in the sagittal plane may also influence the hip stability in flexion. Patients with increased (more cephalic) sagittal orientation of the acetabulum have decreased femoral head coverage anteroinferiorly and increased coverage posteroinferiorly. Meanwhile, a less cephalic sagittal orientation may indicate a predisposition to posteroinferior instability. The presence of cam and/or pincer morphologic features would also contribute to a levering mechanism with anteroinferior repercussion. 23 In the authors’ experience, the dynamic arthroscopic examination before and after acetabuloplasty and/or femoroplasty is very helpful to guide the arthroscopic treatment as well as to educate the patients regarding unstable positions to be avoided after surgery. The identification of anteroinferior hip instability intraoperatively often guides the surgeon to identify the adequate location of the cam and pincer deformity that may be contributing to anteroinferior hip instability through a levering mechanism. Patients are educated to avoid the positions associated with instability in flexion. For instance, individuals with instability in flexion, abduction, and external rotation are oriented to avoid flexion beyond the instability threshold or to internally rotate the hip when flexing.
There are limitations to this study. First, the ligamentous structures that help to stabilize the hip in flexion and the femoral torsion were not assessed in the present study. The MRI scans of the control group were performed for nonorthopaedic reasons and did not allow assessment of the ligamentum teres or the femoral torsion. Second, while control patients were matched for age and sex, they were not matched for height, weight, and activity level, which may influence hip stability. Third, the sagittal orientation of the acetabulum may also influence the inferior stability of the hip, and this parameter could not be assessed in the MRI studies utilized in this investigation.
Conclusion
Abnormal morphology of the anterior acetabular horn is associated with anteroinferior instability in hip flexion. The ASA and AHA can aid in the diagnosis of hip instability.
A video supplement for this article is available at http://journals.sagepub.com/doi/suppl/10.1177/2325967120965564
Footnotes
Notes
Final revision submitted July 3, 2020; accepted July 29, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: H.D.M. has received research support from Smith & Nephew, educational payments from Pylant Medical, and nonconsulting fees from Smith & Nephew and Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Baylor Scott & White Research Institute (ref No. 328900).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.