
Abstract
Background:
Although there is a higher prevalence of noncontact anterior cruciate ligament (ACL) injuries during a direction diversion maneuver (DDM), no previous studies have reported how foot-planting strategies affect ACL loading.
Purpose:
To investigate the effect of foot-planting strategies on ACL loading in women during a DDM task using a musculoskeletal modeling approach.
Study Design:
Descriptive laboratory study.
Methods:
A total of 13 female participants performed a DDM task, which involved running at 4.5 ± 0.2 m/s and turning left at 35° to 55° under a foot-planting strategy in 3 directions: neutral, toe-in, and toe-out. Kinematic and kinetic data were measured with the use of a 3-dimensional motion capture system and force platform to calculate variables such as joint angle, shear force, and moment. Anterior ACL and posterior ACL forces were extracted using musculoskeletal modeling.
Results:
The peak anterior ACL force was significantly larger for the toe-out condition (31.29 ± 4.02 N/body weight [BW]) compared with the toe-in condition (25.43 ± 5.68 N/BW) (P = .047), with no significant difference in the neutral condition. The toe-out condition had a higher knee valgus angle (2.98° ± 4.20°; P = .041), knee shear force (10.20 ± 1.69 N/BW; P = .009), and knee internal rotation moment (–0.18 ± 0.16 N·m/BW×height; P = .012) than the toe-in and neutral conditions.
Conclusion:
Through musculoskeletal modeling, we were able to conclude that the toe-out condition during the DDM might result in a higher risk of ACL injuries. Athletes and sports practitioners should avoid the toe-out foot-planting strategy when participating in a sporting activity.
Clinical Relevance:
Based on these findings, medical professionals and athletic coaches can gain knowledge on how foot-planting strategy affects ACL loading. Understanding the actual cause of an ACL injury can be useful for designing preventive training programs or strategies to decrease the risk of such injuries.
The anterior cruciate ligament (ACL) is one of the most frequent injury sites, accounting for more than 20.5% of all knee injuries with an injury rate of 6.5 per 100,000 athlete-exposures during different sporting activities. 18,23,31 Although the most common mechanism of injury is player-to-player contact, Joseph et al 23 reported that noncontact injuries account for 37.9% of ACL injuries, at an injury rate of 8.9 per 100,000 athletes, and the prevalence of such injuries is higher among female athletes. Numerous studies have acknowledged the severity of ACL injuries among athletes: Around 76% of ACL injuries require surgery, which ultimately results in a decrease in the quality of life through increasing the risk of secondary injuries or disabilities, leading to financial burden. 23,24,30 Therefore, an understanding of the mechanisms involved in the increased risk of ACL injuries is necessary. 7,23,48
The threshold for an ACL injury has been reported to be at 2000 N. 33,38 From a biomechanical perspective, the risk of ACL injuries increases primarily when there is a smaller knee flexion angle, large ground-reaction force, large knee valgus angle and moment, and greater knee shear force than typically encountered. 29,42 These biomechanical risk factors can increase during sporting situations when an athlete has to change direction to bypass his or her opponents suddenly, also known as a direction diversion maneuver (DDM). 3,8,28 In this situation, the toe is likely to be directed in a neutral, toe-in, or toe-out position depending on the intended movement direction. Various biomechanical risk factors for ACL injury are associated with these 3 movement strategies. The toe-in position is postulated to increase the hip adduction angle as well as the knee internal rotation angle and moment during planting movements. 45 In the case of the toe-out position, studies have reported that it results in an increase in the valgus angle and varus moment of the knee joint during landing and side-cutting movements. 10,42 However, these studies only postulated that there would be an increase in ACL loading, without directly estimating the ACL load.
The purpose of our study was to investigate the effect of a foot-planting strategy on ACL force in a sporting movement using a musculoskeletal modeling approach. This technique has been implemented to directly estimate the ACL force and its relation to an ACL injury during running, 38,40 stop-jump, 25,26 and sidestep cutting. 36,47 Previous studies have postulated the effect of a foot-planting strategy on ACL force and the risk of ACL injuries using a causal relationship with lower limb joint kinematics and kinetics. In our study, we used musculoskeletal modeling to estimate the ACL force directly in addition to the lower limb joint kinematics and kinetics. Hence, our approach allowed us to determine the foot-planting strategy that results in the largest ACL force and thereby the highest risk of ACL injuries. Further, we aimed to determine how the increase in ACL force changes the lower limb kinematics and kinetics to confirm the risk factors of an ACL injury according to the foot-planting strategy mentioned in previous studies. 36,47 Because Teng et al 42 reported knee valgus angle and varus moment as significant risk factors that increase the ACL load compared with other risk factors, we hypothesized that ACL loading during the toe-out condition would be significantly higher than that for the neutral and toe-in conditions.
Methods
Participants
A total of 13 women (mean age, 24.23 ± 3.54 years; mean height, 162.77 ± 5.96 cm; mean weight, 55.31 ± 6.17 kg) participated in the study. Only female participants were selected because of their higher risk for ACL injury compared with men. 11,33 The participants were right foot–dominant, had no known neurological or muscle diseases, and regularly participated in physical activity (at least twice a week). All participants signed informed consent forms regarding the procedure and the risks involved in the study, which were approved by our institutional review board.
Experimental Procedure
The participants were provided with athletic clothing and shoes before the experiment, and a period of stretching and a warm-up session were granted to minimize the risk of injuries. A total of 51 reflective markers were placed on the joints and segments of the body (see Appendix Table A1 for locations of markers). The position of the reflective markers was recorded using 18 infrared cameras combined with motion capture software (Oqus 7+; Qualisys) at a sampling frequency of 200 Hz. The participants were then asked to perform a DDM task. The task involved running toward a force platform (Type 9287BA; Kistler) from a distance of 5 m at a speed of 4.5 ± 0.2 m/s and turning left at 35° to 55° from the direction of travel once the right foot landed on the force platform. 32,33,46 The instant of planting was defined as the point when the right foot landed on top of the force platform. The 3-directional force and moment obtained from the force platform were recorded at a sampling frequency of 1000 Hz.
The DDM task was performed for 3 conditions: when the toe position was neutral, toe-in, and toe-out from the direction of travel at the landing zone. 42,45 A foot-planting position template (nonslippery tape) was pasted on top of the force platform to offer feedback regarding the direction of the toe. 45 The neutral position was defined as 0° of rotation from the anterior line along the sagittal plane of the body, while toe-in and toe-out were defined as 30° of internal and external rotation, respectively. There were 3 trials performed for each condition, and a trial was considered successful when (1) the entire foot landed on top of the force platform and (2) the participant correctly planted her foot on the position template (Figure 1). The running speed was controlled using 2 timing gates (Microgate).
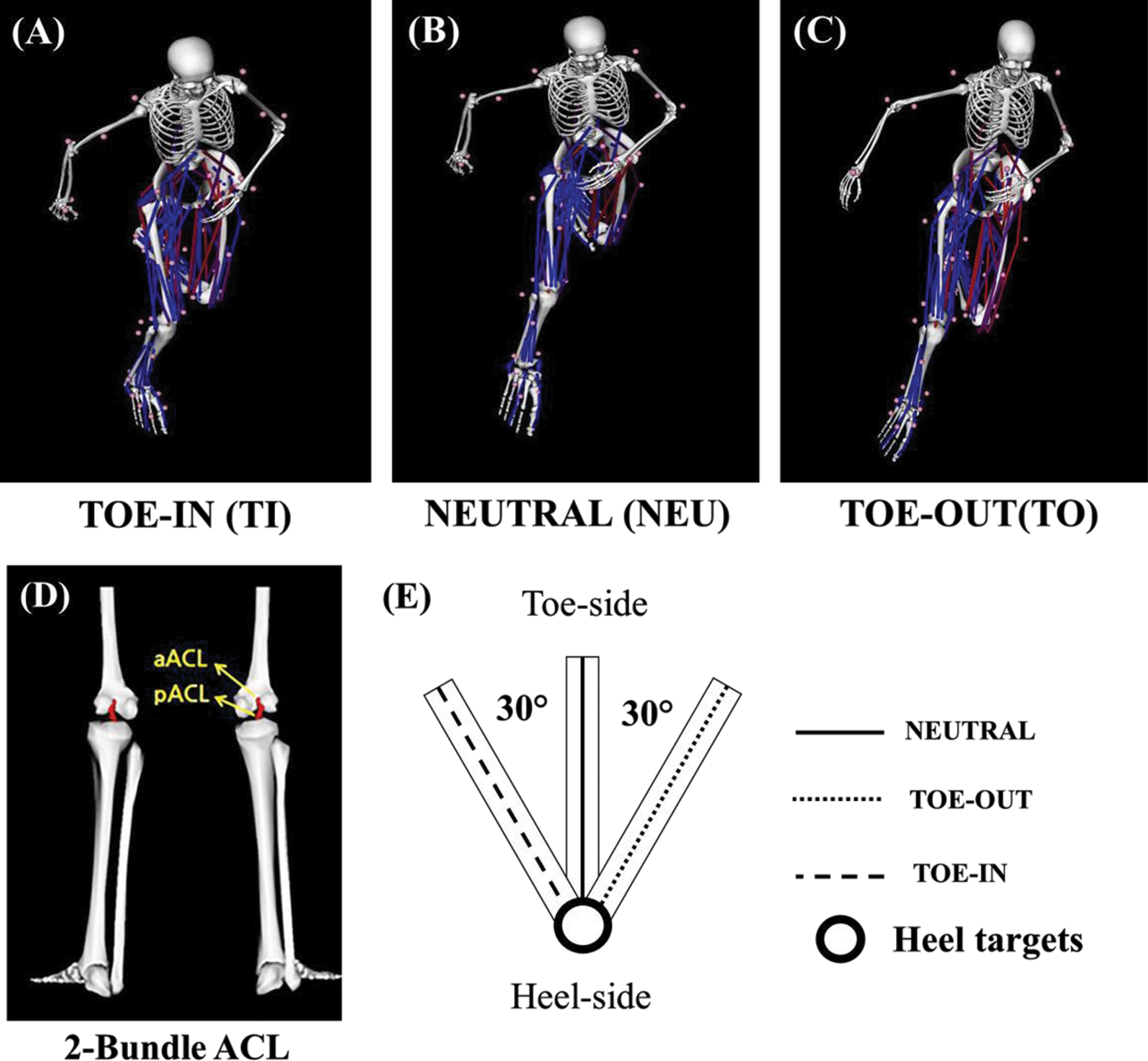
(A-C) The 3 foot-planting conditions performed in the study. The images were extracted at the peak anterior ACL (aACL) load during each condition. (D) The 2-bundle ACL model used in musculoskeletal modeling. The model extracted both aACL and posterior ACL (pACL) forces. (E) The foot-planting position template for the 3 different conditions. Participants were instructed to plant at the neutral, toe-out, or toe-in position. ACL, anterior cruciate ligament.
Data Analysis
The kinematic and kinetic data obtained from the motion capture system and the force platform after labeling were exported as C3D files for processing in Visual3D (V 5.01; C-Motion). Thereafter, a fourth-order, zero-lag low-pass Butterworth filter with a cutoff frequency of 15 Hz was applied to the data. 12
Calculation of Kinematic and Kinetic Variables
The kinematic model was constructed based on the standing trial using Visual3D software. The midpoint of each joint was estimated, and we specified the segments and their orientation from the proximal and distal endpoints. The Cardan sequence (x-y-z) was used to define the rotation of the segments for the local coordinate system. Peak and mean values for different parameters were calculated using inverse kinematics and dynamics algorithms at the instant of planting from each trial, which was identified with a force profile in the vertical direction (F
z
). For interparticipant comparability, all the calculated parameters were also normalized to body weight (BW) and height (HT). The parameters computed for analysis were as follows: Ground-reaction force (N, N/BW): peak force at the instant of foot planting. Center of mass (COM): based on the location of the COM of each segment expressed in meters (m), COMvelocity is the first derivative of the COM expressed in meters per second (m/s). COM–center of pressure (COP) displacement (m/HT): resultant vector obtained by subtracting displacement of the COP from displacement of the COM and normalized to HT. Joint angle (deg): ankle (dorsiflexion/abduction/inversion), knee (valgus/flexion/external rotation), and hip (flexion/adduction/internal rotation). Joint moment (N·m, N·m/[BW×HT]): ankle (plantarflexion/adduction/inversion), knee (extension/varus/internal rotation), and hip (extension/abduction/external rotation), with all moments computed in the study defined as internal rotation moments and normalized to HT and BW. Joint force (N/BW): peak shear force and BW-normalized shear force. ACL force (N, N/BW): anterior ACL (aACL) and posterior ACL (pACL) forces and BW-normalized force.
ACL Model
The musculoskeletal model to calculate the ACL load was developed using OpenSim software (Version 3.3; Stanford University). The skeleton of the model had a total of 14 segments, 23 degrees of freedom, and 92 muscles, with 2 bundles of the ACL (anterior and posterior bundles) to calculate the ACL load. 13 The anterior and posterior bundles are 2 main functional bundles of the ACL that exhibit differing length-change patterns during flexion-extension of the knee (Figure 1). The anterior bundle is the primary restraint against anterior tibial translation, while the posterior bundle is the stabilizer during full extension of the knee and works to prevent rotatory loads. 14,35 A detailed description of the model’s properties is provided in Appendix 2.
ACL Load Calculation
The aACL and pACL forces were calculated using the method developed by Delp et al. 9 The process includes body scaling, inverse kinematics, inverse dynamics, the residual reduction algorithm (RRA), computed muscle control (CMC), and forward dynamics (Figure 2). Body scaling applies the participant’s body information to the musculoskeletal model modified in this study. Inverse kinematics is the process of calculating the joint angle based on coordinate data. Inverse dynamics calculates the force and moment of each joint based on the joint angle calculated through inverse kinematics. The RRA dynamically optimizes the force and moment of each joint using a residual elimination algorithm that minimizes the errors included in the measurement. CMC calculates the excitation of individual muscles by taking into account the maximum muscle force and actual measured motion and force to perform static dynamics. The information calculated through CMC goes through a static dynamics process and becomes a final model, which includes individual muscle and tendon length, active force, and passive force. 9,43,44 The Hill model was used for calculating the ACL force, and the formula is as follows 25,26 :

where
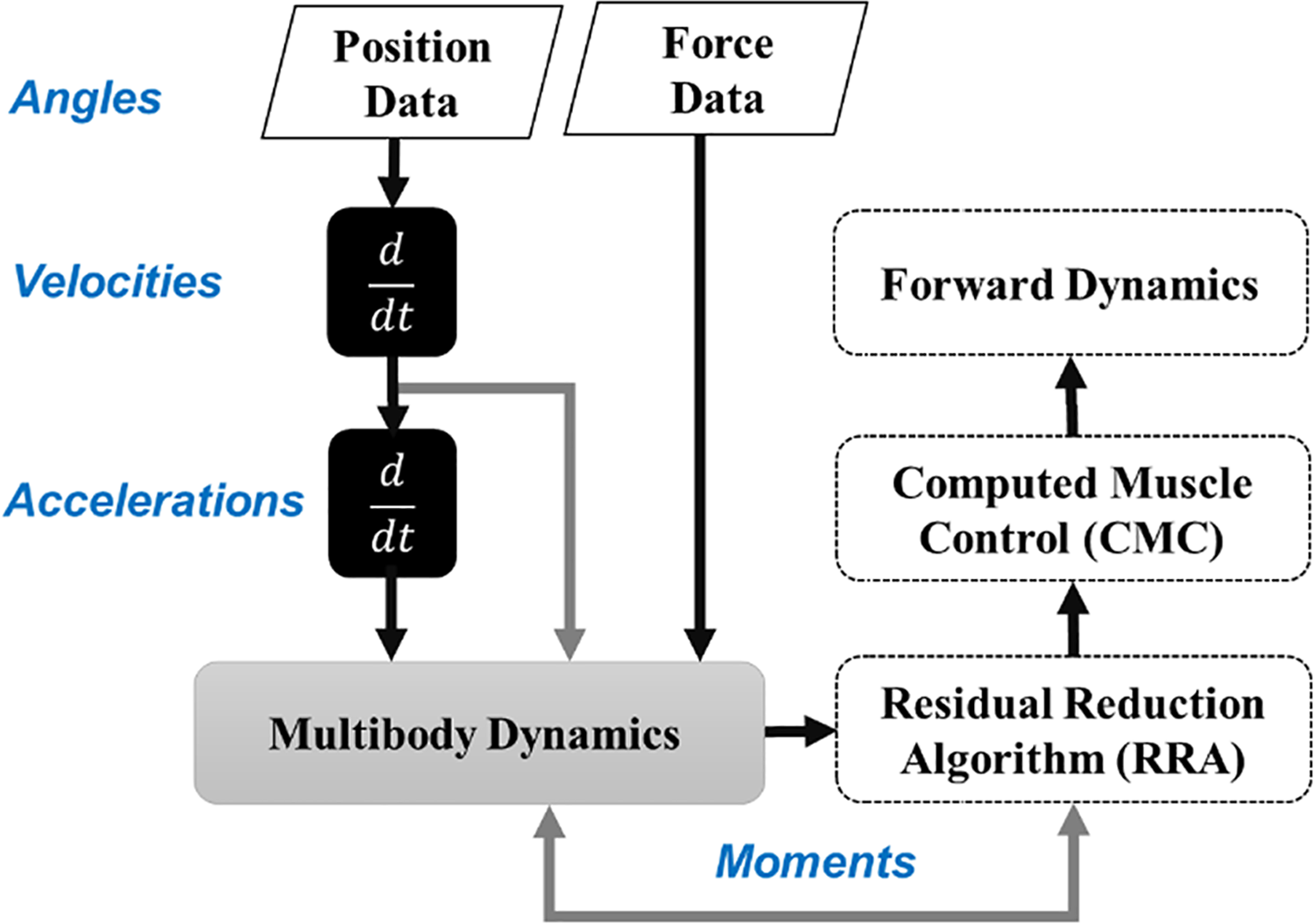
The process of calculating the anterior cruciate ligament load using a musculoskeletal modeling approach. The d/dt denotes differentiation of the position and velocity to calculate velocity and acceleration, respectively.
Statistical Analysis
One-way repeated-measures analysis of variance (ANOVA) was used to evaluate the differences in the dependent variables (validation variables [COMvelocity], joint kinematic and kinetic variables, ACL forces) based on the foot-planting strategy (neutral, toe-in, toe-out). A post hoc test was performed using Bonferroni correction, and the statistical significance level was set at α = .05. All statistical analyses were performed using SPSS 23.0 (IBM).
Results
Validation of the DDM Maneuver
The mean COMvelocity at the instant of planting for the neutral, toe-in, and toe-out conditions was 4.47 ± 0.36, 4.54 ± 0.24, and 4.42 ± 0.38 m/s, respectively (Table 1). The mean COMvelocity for any of the foot-planting conditions was not significantly different from the controlled running speed: 4.5 ± 0.2 m/s (F 2,11 = 3.52; P < .405). Hence, the running velocity was effectively controlled.
Kinematic and Kinetic Variables at the Instant of Foot Planting a

a Data are reported as mean ± SD unless otherwise indicated. aACL, anterior ACL; ACL, anterior cruciate ligament; BW, body weight; COM, center of mass; DDM, direction diversion maneuver; HT, height; pACL, posterior ACL.
b Significant differences revealed after post hoc analysis.
Joint Kinematics, Moment, and Shear Force
Table 1 presents the joint kinematics and kinetics of the lower extremities during the DDM at the instant of planting. One-way repeated-measures ANOVA concluded that there was a significant main effect of foot-planting strategy on ankle dorsiflexion (F 2,11 = 10.39; P = .001) and inversion (F 2,11 = 8.086; P = .007), knee valgus (F 2,11 = 4.325; P = .004) and external rotation (F 2,11 = 8.721; P < .001), and hip adduction (F 2,11 = 10.07; P < .001) and internal rotation (F 2,11 = 8.571; P = .006).
The post hoc analysis showed that ankle dorsiflexion for the toe-in condition was significantly higher than that for the neutral and toe-out conditions. The ankle abduction angle for the toe-out condition was significantly higher than that for the neutral condition, and the ankle inversion angle for the toe-in condition was significantly higher than that of the neutral and toe-out conditions. In the case of the knee joint, the valgus angle was significantly higher (1) for the toe-out condition versus the toe-in and neutral conditions and (2) for the neutral condition versus the toe-in condition. The knee external rotation angle was significantly higher (1) for the toe-out condition versus the neutral and toe-in conditions and (2) for the neutral condition versus the toe-in condition. Regarding the hip joint, the adduction angle was significantly higher (1) for the toe-out condition versus the neutral and toe-in conditions and (2) for the neutral condition versus the toe-in condition. The hip internal rotation angle was significantly higher (1) for the toe-in condition versus the neutral and toe-out conditions and (2) for the neutral condition versus the toe-out condition (Table 1).
The ANOVA results for peak knee shear force indicated that there was a significant main effect of foot-planting strategy on BW-normalized peak shear force (F 2,11 = 8.649; P = .006). The post hoc analysis revealed that the BW-normalized peak knee shear force was significantly higher for the toe-out condition compared with the neutral condition, whereas no significant difference was observed with the peak knee shear force of the toe-in condition.
The ANOVA results for lower limb joint moments indicated that there was a significant main effect of foot-planting strategy on joint moment only for knee internal rotation (F 2,11 = 5.234; P = .045) and hip abduction (F 2,11 = 26.63; P < .001). The post hoc analysis revealed that the knee internal rotation moment for the toe-out condition was significantly higher than that for the toe-in condition, whereas no significant difference was observed with the neutral condition. Further, the hip abduction angle was significantly higher (1) for the toe-out versus the toe-in and neutral conditions and (2) for the neutral versus the toe-in condition (Table 1).
Peak ACL Force
The ANOVA results for ACL forces (Table 1) indicated that there was a significant main effect of foot-planting strategy only on normalized peak aACL force (F 2,11 = 4.133; P = .005). The post hoc analysis revealed that the normalized peak aACL force was significantly higher for the toe-out condition compared with the toe-in condition.
Discussion
The purpose of the study was to investigate the effect of foot-planting strategy (neutral, toe-in, and toe-out) on ACL loading in women during a DDM task using musculoskeletal modeling. We hypothesized that because of kinematic and kinetic differences during the toe-out condition, the ACL load would be larger compared with that in the other foot-planting conditions. Our hypothesis was confirmed, as the peak aACL force was significantly larger for the toe-out condition compared with the toe-in condition, with no significant differences with the neutral condition.
Sporting movements involve phases of rapid deceleration, such as the instant of planting during a DDM and jump. The sudden deceleration causes changes in kinematics and kinetics, particularly at the knee joint; these include increases in flexion and valgus angles, shear force, and varus and internal rotation moments, which increase the risk of ACL injuries. 41,48 The risk further increases when there is a change in the foot direction during planting. 45 Hence, a quantitative understanding of these risk factors can provide guidelines for preventive mechanisms for ACL injury. Previous studies have provided a causal relationship between joint kinematics and kinetics and the risk of ACL injuries according to the foot-planting strategy. Tran et al 45 and Teng et al 42 have provided contradicting views regarding the reason behind the higher risk of ACL injuries during toe-in and toe-out foot-planting strategies, respectively. The musculoskeletal modeling technique used in the current study was novel in that it allowed us to estimate the ACL forces. The significantly higher ACL force and consequent increase in knee shear force and knee internal rotation moment that we found regarding the toe-out condition indicate that this particular foot-planting strategy during a DDM has the highest risk of ACL injuries.
The kinetic chain at the planting phase initiates from the foot and the ankle, which then transfers the forces to the knee joint. 1 Dorsiflexion of the ankle joint has been reported to be positively correlated with knee flexion displacement and restriction in ankle range of motion in the transverse plane; that is, a larger dorsiflexion angle increases the valgus angle of the knee joint. 15,39 Hence, the larger dorsiflexion observed during the toe-out foot-planting strategy compared to the toe-in condition had a kinematic chain effect on the proximal joints, specifically increasing the valgus angle and ACL force (Table 1).
A study conducted by Donnelly et al 11 reported that the dynamics of force distribution varies depending on foot-planting strategy (forefoot vs rearfoot). Those authors reported that forefoot planting requires a large dynamic force on the ankle joint, while rearfoot planting has a large dynamic force on the knee joint, which increases the risk of ACL injuries. Particularly, rearfoot planting during a DDM has been reported to increase knee joint extension and valgus angle, thereby increasing the ACL load. 6 The DDM performed in this study was intended to observe these mechanical changes to the knee joint load by performing rearfoot planting.
The position of the upper body in the sagittal plane, that is, forward leaning, decreases the possibility of ACL injury by increasing the shock absorption volume and flexion angle of the knee joint as well as reducing the activity of the quadriceps. 37 Although we did not measure the trunk angle that corresponds to a forward-leaning posture, we found no significant differences in hip flexion angle between the 3 foot-planting strategies. Nevertheless, hip adduction angle, hip internal rotation angle, and hip abduction moment were statistically different among all 3 conditions. From a similar perspective, a study on sidestep cutting reported that a change in whole-body COM to the medial and forward direction could significantly reduce the valgus moment of the knee joint and decrease the risk of ACL injury. 12 Chaudhari et al 5 reported that the movement of the arm and upper body position during planting could also affect knee varus moment. Therefore, if we assume that there is a shift in the COM that coincides with rotation of the torso, the braking force changes the direction of the COM and contributes to maintaining a constant speed, preventing the body from excessive rotation about the vertical axis when performing a DDM. 22 This may explain the consistency of the DDM. The result of COM-COP displacement in the planting phase confirms the different foot-planting conditions.
Opposing views have been formulated regarding the biomechanical risk factors for ACL injury due to foot direction during planting. The risk factors for toe-in foot planting have been reported as increased hip adduction and knee internal rotation angles and moments and decreased hip and knee flexion angles. 45 In the case of the toe-out foot planting, the biomechanical risk factors are increased knee valgus angles and varus moments. 26,42 Fukuda et al 16 and Hewett et al 20 have shown through cadaveric and clinical studies that larger valgus angles increase anterior tibial translation and consequently increase the ACL force. In our study, we directly estimated the ACL forces and also found that increased valgus angle during a DDM with toe-out foot planting resulted in significantly higher ACL forces. Further, we found that there was an increase in knee shear forces during toe-out foot planting, which is known to result in greater strain on the anteromedial bundle of the ACL. 4,48 Hence, there was a higher risk of ACL injury during the DDM with the toe-out foot-planting strategy because of significantly larger ACL forces, knee valgus angles, and shear forces.
Avoiding toe-out planting during sporting situations can be challenging, as an ACL injury occurs within 50 milliseconds after ground contact and is faster than the time (120∼140 milliseconds) required by our nervous system to generate the reflex mechanisms to protect the knee. 17,21,27 Therefore, ACL injury prevention programs must include not only targeted exercises but also automatic movements that resemble complex unanticipated events observed on the field specific to the type and level of sport, that is, elements of anticipation, perturbation, attention, and visual-motor control. 2,17,19
Limitations
There are several limitations to our study. First, our sample size was quite small (N = 13), and our study was limited to a single sporting movement (the DDM). A future study with a larger sample size and the inclusion of various sporting movements (stop-jump, drop landing, sidestep cutting, etc) might enhance the generalizability of our results. Second, in our study, we focused on noncontact movements because of the difficulty of simulating dynamic contact movements in a controlled experimental setting. Finally, the participants in our study had no known history of ACL injury, so the kinematic and kinetic factors that increase the risk of ACL injury might be different than for those with a history of ACL injuries. Hence, our results should be used to develop ACL injury prevention protocols and training programs for athletes with no history of ACL injury.
Conclusion
This is the first study to use musculoskeletal modeling to estimate the ACL forces for 3 foot-planting strategies (toe-in, neutral, and toe-out) during a DDM. Compared with previous studies, the direct estimation of the ACL forces allowed us to define the relationship between foot-planting strategies and ACL injury; higher ACL forces resulted in a higher risk of injury. Further, the results of our study showed that for the toe-out condition there was a significant increase in knee valgus angle, which is a significant risk factor for ACL injury. No significant differences were observed for knee varus moment, however there were also increases in knee shear force, knee internal rotation moment, and aACL force, which allowed us to conclude that the toe-out foot direction during a DDM might lead to a higher risk of ACL injury. These results can be used by athletes, coaches, and medical professionals to create a preventive training program or strategy to decrease the risk of initial ACL injury.
Footnotes
Final revision submitted April 27, 2020; accepted June 3, 2020.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Korea Institute of Sport Science (No. KISS-1810-044-01).
APPENDIX 1
Marker Locations During Static and Dynamic Trials a

| Participant No. | Marker Location | Participant No. | Marker Location |
|---|---|---|---|
| 1 | Left acromion | 28 | Right acromion |
| 2 | Left ankle: lateral | 29 | Right ankle: lateral |
| 3 | Left ankle: medial | 30 | Right ankle: medial |
| 4 | Left ASIS | 31 | Right ASIS |
| 5 | Left biceps | 32 | Right biceps |
| 6 | Left elbow | 33 | Right elbow |
| 7 | Left heel | 34 | Right heel |
| 8 | Left knee: lateral | 35 | Right knee: lateral |
| 9 | Left knee: medial | 36 | Right knee: medial |
| 10 | Left midfoot: lateral | 37 | Right midfoot: lateral |
| 11 | Left midfoot: superior | 38 | Right midfoot: superior |
| 12 | Left shank: front | 39 | Right shank: front |
| 13 | Left shank: rear | 40 | Right shank: rear |
| 14 | Left shank: upper | 41 | Right shank: upper |
| 15 | Left temple | 42 | Right temple |
| 16 | Left thigh: front | 43 | Right thigh: front |
| 17 | Left thigh: rear | 44 | Right thigh: rear |
| 18 | Left thigh: upper | 45 | Right thigh: upper |
| 19 | Left toe: lateral | 46 | Right toe: lateral |
| 20 | Left toe: medial | 47 | Right toe: medial |
| 21 | Left toe: tip | 48 | Right toe: tip |
| 22 | Left upper arm: rear | 49 | Right upper arm: rear |
| 23 | Left wrist: lateral | 50 | Right wrist: lateral |
| 24 | Left wrist: medial | 51 | Right wrist: medial |
| 25 | Sternum | ||
| 26 | Top of head | ||
| 27 | V. sacrum |
a ASIS, anterior superior iliac spine.