
Abstract
Background:
Several arthroscopic techniques for the treatment of avulsion tibial spine fractures have been described in the literature.
Purpose:
To evaluate the outcomes of the arthroscopically assisted stainless steel wiring technique in the treatment of avulsed tibial spine in adults.
Study Design:
Case series; Level of evidence, 4.
Methods:
This retrospective study involved 28 patients (28 knees), 16 to 42 years of age, with tibial spine avulsion fracture that was treated using arthroscopic reduction and cerclage wire fixation by a single surgeon between March 2015 and August 2018. The degrees of avulsion in these patients were type II (n = 12), type III (n = 10), and type IV fractures (n = 6). Clinical assessment included International Knee Documentation Committee (IKDC) objective score (which noted swelling), range of knee movement, Tegner activity scale, Lachman test, and pivot-shift test compared with the normal opposite knee.
Results:
The mean follow-up period was 24.1 months (range, 18-30 months). The mean IKDC score was 93.7 (range, 88.5-98.9); the IKDC score was normal in 22 patients and nearly normal in 6 patients. The Lachman test was grade 1 in 25 patients and grade 2 in 3 patients, whereas the pivot-shift test was grade 0 in 26 patients and grade 1 in 2 patients. All patients achieved their preinjury Tegner activity levels. Radiological assessment showed healing in all patients within a mean of 12 weeks after surgery.
Conclusion:
The outcomes of all patients were satisfactory; fixation by cerclage wiring permitted reduction of tibial spine fragment anatomically to its fracture bed, provided stable fixation in displaced tibial spine avulsion, and allowed for early rehabilitation and weightbearing because of stable fixation.
Tibial spine fractures were first described by Poncet in 1875. 25 Based on the classification system proposed by Meyers and McKeever 22 in 1959, these fractures can be classified into 3 types according to their displacement severity. 15 Type I fractures are nondisplaced or minimally displaced fractures; type II fractures refer to displacement of anterior one-third to one-half of the avulsed fragment; and type III fractures refer to full displacement of the fracture. A type IV fracture was later added to the classification system by Zaricznyi, 30 and it involves comminution of the displaced fragment.
Currently, the operative techniques used to manage tibial spine fractures range from arthrotomy with screws, wires, staples, pins, or suture fixation 28,30 to arthroscopic internal fixation with cortical or cannulated screws, percutaneous pins, and suture fixation with and without hardware. 5,19
Interestingly, the outcome of arthroscopic fixation in children and adolescents is usually favorable, but results in adults are less predictable. 4 Most of the previously published studies demonstrated a disturbing amount of residual laxity after arthroscopic treatment of tibial spine fractures. 6,19 This residual laxity may be due to a number of factors. One such consideration is plastic deformation of the anterior cruciate ligament (ACL) before ultimate fracture that may lead to an elongation of the ligament. 24 Another factor might be the technically demanding arthroscopic techniques and imperfect reduction that may result in nonunion and ACL lengthening. 7,8,16,19,21 A third factor for residual laxity might be secondary displacement and malunion of the bony fragment due to insufficient fixation or aggressive rehabilitation. In addition, some of the functionally disabling complications after surgical treatment of tibial eminence fractures include limited range of motion, anterior knee pain, and loss of extension resulting from mechanical block in the intercondylar region. 13,30
Given this background, the present study aimed to evaluate the functional outcome of arthroscopic cerclage wire fixation for tibial spine fracture in skeletally mature adults. We hypothesized that the arthroscopic cerclage wire fixation for tibial spine fracture in adults could restore knee stability and early full range of motion.
Methods
This retrospective study was approved by our institutional ethics committee. The study included 28 adults (28 knees) (27 male and 1 female) with intercondylar eminence fracture who underwent treatment between March 2015 and August 2018 in our arthroscopy unit. Diagnoses were confirmed using clinical findings and radiographic assessment by plain radiography and computed tomography (Figure 1). Based on the classification by Meyers and McKeever 22 and Zaricznyj, 30 12 patients had type II, 10 had type III, and 6 had type IV tibial spine fractures. The mean age of the patients at the time of surgery was 24.1 years (range, 16-42 years), and the mean time of surgery after trauma was 5.25 days (range, 1-16 days). The mechanism of trauma was motorbike accidents in 21 patients and road traffic accidents in 7 patients (pedestrians), as shown in Table 1.
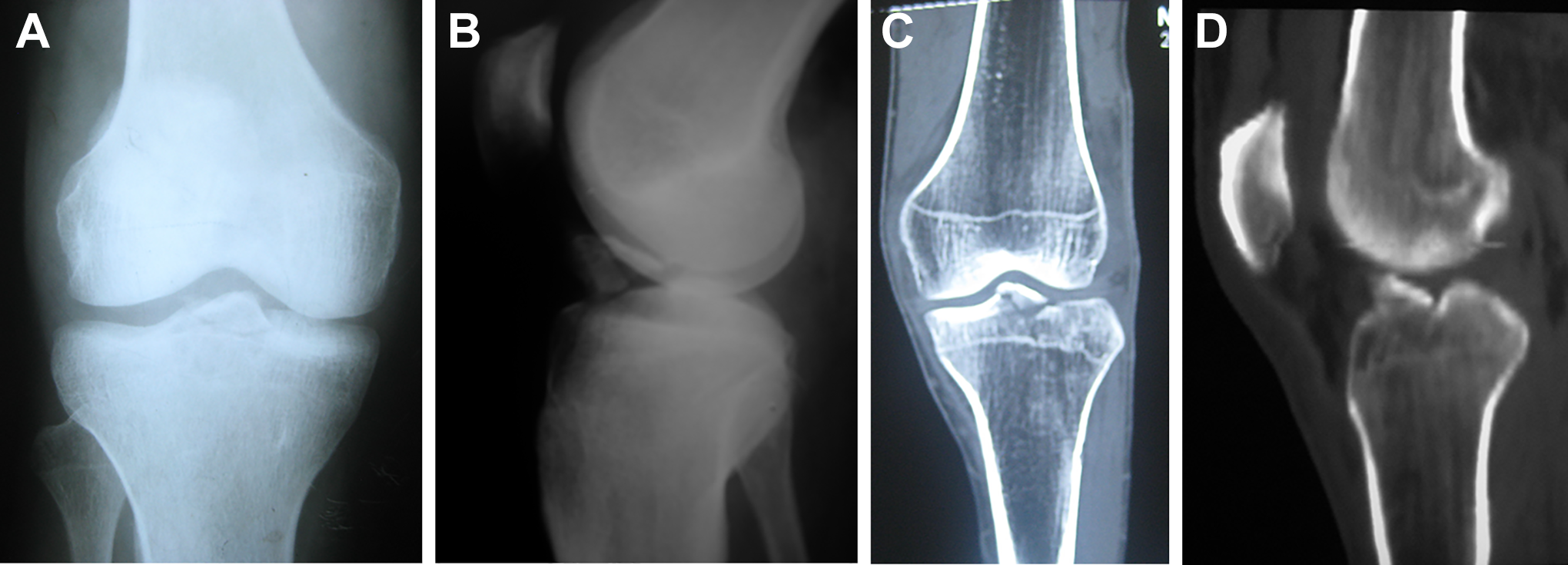
Avulsed tibial spine as shown on (A) anteroposterior and (B) lateral radiographs as well as (C and D) computed tomography.
Characteristics of the Patients a

a MBA, motor bike accident; RTA, road traffic accident.
b Type I, nondisplaced or minimally displaced fractures; type II, displacement of anterior one-third to one-half of the avulsed fragment; type III, full displacement of the fracture; type IV, comminution of the displaced fragment.
Surgical Technique
All surgeries were performed by a single senior surgeon (M.M.A.). For this study, we adopted the treatment technique described by Abdelhamid et al. 1 In brief, we arthroscopically examined the suprapatellar, medial, and lateral compartments of the knee as well as the notch to determine the fracture type and any associated chondral or meniscal injuries.
To determine the degree of displacement, fragmentation, and soft tissue interposition, the tibial spine fragment was probed through the standard medial portal (Figure 2). The medial and lateral menisci were also evaluated, and the intermeniscal ligament was probed to assess the degree of its confinement in the fracture bed. The fracture surfaces were debrided to clean any soft tissue attachment, and the fracture site was abraded to facilitate union (Figure 3).

Arthroscopic view of the right knee through the lateral portal showing a displaced type II tibial fracture.

Arthroscopic view of the right knee through the lateral portal showing debridement of the fracture by shaver to refresh the fracture.
Next, the avulsed fragment was anatomically reduced to its bed, after which preliminary fixation was performed using 2 Kirschner wires (Figure 4). The ACL tibial guide was applied through the medial portal and then aimed at and secured to the avulsed fragment. A guide pin was introduced through the ACL tibial guide from the proximal anteromedial surface of the tibia, and a bone tunnel was drilled using a 4-mm cannulated drill (Figure 5).

Arthroscopic view of the right knee through the lateral portal, showing the fracture reduced and provisionally fixed with a percutaneous Kirschner wire.

(A) Arthroscopic view of the right knee through the lateral portal showing 2-mm guide pin just lateral to the fracture site. (B) Photo of the right knee showing the scope in the lateral portal and the ACL tibial guide in the medial portal and secured to the proximal tibia with a 4-mm drill advanced through it.
A cerclage wire loop (0.5 mm) was then inserted into the knee joint through the drilled tunnel. The procedure was repeated by inserting the ACL tibial guide on the lateral side of the avulsed fragment. After this, another tunnel was developed with a bone bridge on the anteromedial side of the upper tibia between both tunnels at a distance of not less than 1 cm. By tensioning the double cerclage wire loops, the avulsed fragment was anatomically reduced and fixed to the underlying bed (Figure 6A). At the medial side of the proximal tibia, the cerclage wire was tightened and ligated (Figure 6B).

(A) Arthroscopic view of the right knee through the lateral portal showing a horizontal mattress suture of cerclage wire incorporating the avulsed bone fragment. (B) View of the right knee showing the twisted cerclage wire loop.
Postoperative Rehabilitation
Postoperatively, the patients were immobilized for 2 weeks using hinged knee braces with extension. Thereafter, the knee was allowed an initial range of movement of 0° to 30° for 2 weeks; the knee movement was gradually increased by 30° per week. The patient was allowed limited weightbearing as tolerated with crutches for 4 weeks, after which full weightbearing was permitted. From the first day after surgery, the patients followed an isometric quadriceps muscle exercise regimen that was continued through the mobilization period to minimize atrophy. At 6 months postoperatively, the patients were allowed to return to preinjury activity levels.
Postoperative Evaluation
Subjective outcome was obtained using the International Knee Documentation Committee (IKDC) subjective questionnaire that considered symptoms, knee function, and activity levels.
All patients were clinically evaluated by 3 senior observers (H.A.E., M.M.A., M.M.M.). Mean values used for analysis included the Tegner activity scale and IKDC objective forms (which noted swelling), range of knee movement, Lachman test, pivot-shift test, and rotational laxity compared with the normal opposite knee. Plain radiographic investigation included anteroposterior and lateral views to examine the fracture union (Figure 7).
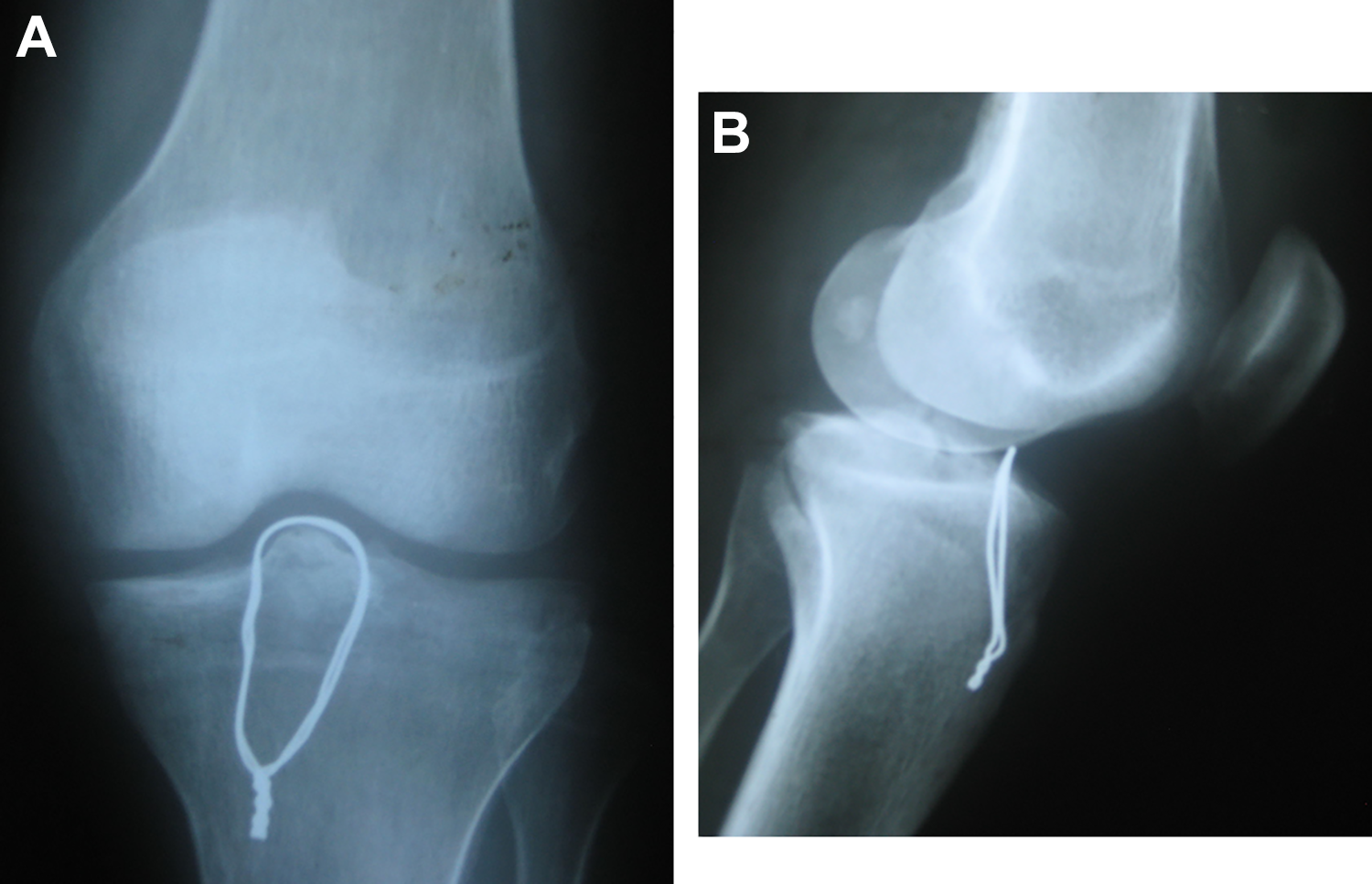
The united tibial spine avulsion fixed by cerclage wire loop as seen on (A) anteroposterior and (B) lateral radiographs.
Statistical Analysis
Data were analyzed with SPSS software (Version 19.0; IBM). Descriptive statistics for categorical variables and measures of central tendency for continuous variables were calculated to summarize the data.
Results
The results of this study are based on clinical and radiological evaluation with a mean follow-up of 24.1 months (range, 18-30 months).
The mean IKDC score at the final follow-up was 93.7 (range, 88.5-98.9). The objective IKDC score was normal (grade A) in 22 patients and nearly normal (grade B) in 6 patients. The Lachman test result was grade 1 in 25 patients and grade 2 in 3 patients, whereas the pivot-shift test was grade 0 in 26 patients and grade 1 in 2 patients. All patients achieved their preinjury Tegner activity levels (level 5 in 21 patients and level 4 in 7 patients). The documented results of subjective and objective knee evaluation scores are presented in Table 2.
Subjective and Objective Scores of Patients a

a A, normal; B, nearly normal; IKDC, International Knee Documentation Committee.
Follow-up radiographs showed union in all patients after 12 weeks. A total of 3 patients showed a slight elevation in tibial eminence (2-5 mm), but the patients were asymptomatic with no history of knee laxity and had returned to their preinjury activity levels.
Complications
We noted that 1 patient with arthrofibrosis underwent an additional procedure of arthroscopic arthrolysis 3 months after surgery. There were 2 patients who had extension lag of <10°, without affecting function. We found that 1 patient had wasting of the quadriceps muscle of 12 mm. A total of 3 patients reported painful irritation to the skin by cerclage wire on kneeling and underwent cerclage wire removal after fracture union. At final follow-up, all patients were very satisfied with their knee function and had resumed their preinjury activity level without any reports of instability.
Discussion
After surgical intervention, all patients in this study were advised to follow a limited rehabilitation regimen due to the fact they had been allowed immediate partial weightbearing but no motion at all for 2 weeks to protect the fixation. The results of this study show that the overall outcomes of all patients were satisfactory, and 26 of 28 patients’ knees were graded as normal or nearly normal. The remaining 2 patients’ knees were abnormal because of a minimal degree of extension loss (<10°) in 1 patient and arthrofibrosis in the other patient. Various studies have showed that long-term functional outcome is more closely related to limited range of motion and pain than it is to instability. Joint laxity is not clinically correlated with poor outcomes. 23
Tibial spine fractures represent a disruption of the ACL complex, 10 and any residual displacement can lead to knee laxity and functional disability. 26 Anatomically reduced tibial spine avulsion fractures have a high risk of displacement with time, and most studies have recommended reduction and rigid fixation of all fracture types. 9
Nevertheless, continued laxity and instability have been reported in 10% of adult patients treated surgically in addition to 22% of patients managed nonsurgically. 3 In addition, positive anterior drawer and Lachman tests have been commonly observed in patients who were satisfied with the clinical result and had functionally stable knees. 17 Two factors are mainly responsible for residual laxity and instability: imperfect reduction (which may result in malunion and ACL lengthening) and plastic deformation of the ligament before ultimate failure and avulsion fracture. 27
In the present study, only 1 patient developed arthrofibrosis. According to the literature, stiffness may occur in as many as 60% of knees that are treated surgically for tibial spine fracture. 3 The limitation in knee movement may occur because of mechanical block of displaced fracture or arthrofibrosis. 18
Muscular weakness has been associated with limited function after these injuries, and it is essential to start early, aggressive postoperative rehabilitation aimed at reestablishing neuromuscular control of the limb. 2 In addition, extension lag can occur secondary to scarring in the anterior compartment of the knee. In such cases, arthroscopic debridement and notchplasty are effective for regaining motion. The loss of full range of motion is due to limited full extension from failure of reduction of a fixed tibial spine or from malunion. 20
Using an arthroscopic technique to treat these injuries is a standard approach that allows for complete evaluation of the other joint structures and management of any associated chondral or meniscal injuries. This technique also allows for early mobilization, quick rehabilitation, and a short hospital stay. 10
Arthroscopic procedures for the management of tibial spine fractures in adults involve ACL reconstruction as well as reduction and fixation with either fiber wire suture or cannulated screws. Early rehabilitation and accelerated range of motion of the knee after any technique are important to avoid arthrofibrosis. 29 Thus, stable solid fixation and early mobilization are the main factors of success.
Both sutures and screw fixation techniques have been well-studied in cadavers. 11 In their retrospective study, Hunter and Willis 14 reviewed patients with tibial spine fractures treated with either screw or suture fixation and reported 44% revision surgeries in the screw fixation group. Removal is often recommended in hardware-related complications. One study reported a 13% reoperation rate in the suture fixation group that resulted largely from limited range of motion due to arthrofibrosis. 13
Gans et al, 12 who reviewed 6 articles that reported repair of tibial eminence fractures, compared fixation by screw versus suture with respect to the degree of laxity. The authors found that 82.4% of patients who received screw fixation had laxity on both the anterior drawer and the Lachman tests compared with 18.8% patients who received suture fixation.
In repairing tibial spine avulsion fractures, Abdelhamid et al 1 used a 0.8-mm cerclage wire hugging the fracture fragment to the underlying bed. Because suture characteristics such as strength and knot security are important for a stable construct, the type of knot used in this technique avoids the possibility of knot slippage, as noted by Pedowitz (unpublished data), who reported on sutures (FiberWire) that were stronger and stiffer than absorbable suture.
The current study entailed 3 limitations related to the rarity of tibial eminence fractures. There was a relatively small number of patients as well as the absence of a control group. Also notable was the short follow-up period. However, this period was considered relatively sufficient (≥6 months) to complete fracture union and gain full range of motion.
Conclusion
An arthroscopically assisted stainless steel wiring technique provided anatomic reduction, stable internal fixation, and stability in all planes, while restoring the original length and kinematic parameters of the ACL. The technique also allowed early postoperative rehabilitation. Standardization of portals and use of a 4-mm drill bit according to the ACL tibial guide made the procedure easier and less time-consuming.
Footnotes
Final revision submitted May 6, 2020; accepted May 18, 2020.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Al-Azhar University, Faculty of Medicine, Assiut, Egypt.