
Abstract
Background:
The use of hip arthroscopic surgery in the treatment of femoroacetabular impingement (FAI) is increasing, but it is universally known as a technically demanding procedure with a “steep” learning curve. There are limited data investigating the correlation between surgeon experience and patient-reported outcomes (PROs) as well as procedure and traction times.
Purpose:
To prospectively evaluate the relationship between surgeon experience and PROs after hip arthroscopic surgery for the treatment of FAI.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
A total of 190 patients undergoing primary hip arthroscopic surgery for FAI were prospectively enrolled during a sports medicine fellowship–trained surgeon’s first 36 months of practice. A radiographic evaluation as well as PRO surveys including the 12-Item Short Form Health Survey (SF-12), the modified Harris Hip Score (mHHS), and the Hip disability and Osteoarthritis Outcome Score (HOOS) were administered preoperatively and at 2 years postoperatively. Logistic regression as well as analysis of variance was performed to evaluate for correlations between surgical experience and PROs, procedure time, and traction time.
Results:
Of the 190 patients, 168 (88%; mean age, 35.3 ± 9.6 years; mean body mass index, 25.07 ± 3.98) completed a 2-year follow-up and were included for analysis. The mean procedure time was 91.5 ± 23.9 minutes, and the mean traction time was 54.0 ± 17.7 minutes. Patients demonstrated significant improvements at 2 years after surgery for all PRO scores (mHHS, HOOS, and SF-12 physical component summary; P < .001), except the SF-12 mental component summary, which had no change (P = .43). The procedure time significantly decreased after 70 cases, while the traction time continued to decrease until 110 cases (R 2 = 0.99; P < .0001). There was no correlation between increasing case volume and 2-year PRO scores (P > .2 for mHHS, HOOS, and SF-12). There was also no difference with increasing case volume and amount of improvement from preoperative to 2-year postoperative PRO scores for the SF-12 and HOOS. Case volume did not affect the complication rate, as this cohort experienced 4 minor cases of neurapraxia.
Conclusion:
Surgical efficiency in hip arthroscopic surgery for the treatment of FAI was maximized after 110 cases in this cohort. However, significant PRO improvements can be achieved early in a surgeon’s practice prior to maximizing surgical efficiency.
Keywords
Femoroacetabular impingement (FAI), as first described by Myers et al 19 in 1999, has become commonly treated using hip arthroscopic surgery. The number of procedures being performed in the United States to address intra-articular hip abnormalities is increasing rapidly. 27 A study to evaluate the trends in patients undergoing hip arthroscopic surgery in the United States using Current Procedural Terminology codes and the PearlDiver patient records database found a 250% increase in the rate of hip arthroscopic surgery between 2007 and 2011. 25 Colvin et al 8 evaluated the American Board of Orthopaedic Surgery database and found that 7.4% of candidates performed hip arthroscopic surgery in 2009 compared with only 1.2% in 1999. Correspondingly, there has been a 500% increase in the scientific literature reporting on hip arthroscopic procedures, as reported by Ayeni et al. 3 The increasing trend of hip arthroscopic surgery in practice and training of new surgeons points to a greater awareness of the benefits and value of this surgical procedure.
Although hip arthroscopic surgery continues to increase in popularity, it is a technically challenging procedure with numerous and inherent potential complications that surgeons must recognize. The most common complications are attributed to traction applied against a post and portal placement. 16 These include pudendal nerve palsy, lateral femoral cutaneous nerve palsy, and scrotal necrosis. In a retrospective review of 194 hip arthroscopic procedures, Souza et al 26 attributed 58.3% of their complications to traction. Byrd 6 found an incidence of pudendal nerve palsy in 10% of 20 consecutive cases. Other complications described in the literature include intra-abdominal compartment syndrome, deep vein thrombosis, femoral neck fractures, iatrogenic hip dislocation, avascular necrosis of the femoral head, chondrolabral injuries, and heterotopic ossification. 1,2,5,13,17,22 –24 In a systematic review of 81 studies that included 6277 hips, Gupta et al 14 found a major complication rate of 0.41%.
Currently, there is a lack of consensus on the minimum number of cases before surgical competency reported in the literature. An arbitrary number of 30 cases was first suggested by a panel of experts at the Second International Hip Arthroscopy Meeting in Hamburg, Germany. 20 However, a recent systematic analysis of 6 studies with a total of 1063 patients by Hoppe et al 15 found insufficient evidence to quantify a learning curve to validate 30 cases. A threshold study identifying hip arthroscopic procedures performed through a New York State database and following these cases for additional hip surgery found a significantly lower risk of subsequent hip surgery when hip arthroscopic surgery was performed by surgeons with a career volume ≥519. 18 A prospective review of a single surgeon’s learning experience found increased complications in the first 30 cases compared with the next 70 cases. 16 Conversely, another prospective analysis found no difference in complication rates between a single surgeon’s initial 30 cases and subsequent 30 cases. 11 Further, a retrospective review of 194 patients over the course of 2 years found no change in the incidence of complications with time or number of cases, although the nature of the complications changed with time. 26 Overall complication rates for hip arthroscopic surgery remain low; Clarke et al 7 reported a 1.4% complication rate in a prospective study of 1054 patients undergoing hip arthroscopic surgery. Therefore, measuring patient-reported outcomes (PROs) may be a better indicator of a patient’s postoperative functional status and a surgeon’s competence.
The purpose of our study was to perform a prospective analysis of a sports medicine fellowship–trained surgeon’s initial hip arthroscopic experience in independent practice to evaluate the relationship between surgeon experience and PROs in the treatment of primary FAI with a minimum of 2-year follow-up. The primary outcome measurements were PRO scores, and secondary measurements included procedure and traction times as well as revision surgery rates. We hypothesized that with increasing case volume, PRO scores would increase over time, and that conversely, the procedure and traction times would decrease.
Methods
Patient Selection and Data Collection
Patients undergoing primary hip arthroscopic surgery for FAI by a single sports medicine fellowship–trained orthopaedic surgeon (A.L.Z.
During the surgeon’s first 36 months of practice from October 2014 to October 2017, there were 190 cases (56 in year 1, 66 in year 2, and 68 in year 3) of hip arthroscopic surgery for FAI performed on patients who met the inclusion and exclusion criteria. This period included the 6-month collection period for part II of the American Board of Orthopaedic Surgery certification examination. Baseline data and survey results were collected before surgery, and postoperative outcome data were analyzed at 2 years. Only patients with a minimum 2-year follow-up were included. A 2-year follow-up was utilized because of previous studies demonstrating continued improvement in PROs through 2 years. 12 Patient demographics such as age, sex, and body mass index were recorded. A detailed physical examination on the affected hip was conducted both preoperatively and at the 2-year postoperative visit. The radiographic evaluation included preoperative magnetic resonance imaging as well as both pre- and postoperative anterior-posterior pelvis views and Dunn lateral 45° views. Radiographic measurements including the alpha angle, lateral center-edge angle, Tönnis grade, and crossover sign were recorded.
All procedures were performed in the ambulatory surgery center of a tertiary referral academic medical center. Overall, 2 arthroscopic portals (anterolateral and midanterior) were utilized and established using fluoroscopic guidance. Limited periportal capsulotomy was performed. The acetabular, femoral, and labral conditions were recorded using the classification by Beck et al. 4 The chondrolabral junction was assessed, and the presence or absence of a wave sign was recorded. 10 Other intraoperative data that were recorded included procedures performed, procedure time (skin incision to closure), and traction time. Adequate cam and pincer resection were confirmed intraoperatively using fluoroscopy.
Patient-Reported Outcomes
PRO scores were prospectively collected for each patient preoperatively and at 2 years postoperatively. Patients completed 3 PRO surveys: the 12-Item Short Form Health Survey (SF-12), the modified Harris Hip Score (mHHS), and the Hip disability and Osteoarthritis Outcome Score (HOOS). The SF-12 contains both a physical component summary and a mental component summary. The mHHS provides a single score assessing hip function and has been commonly used in previous hip arthroscopic studies, so data from this cohort can be compared with those from other institutions. The HOOS is an in-depth score that provides information on specific functional outcomes after hip surgery and includes 5 subscales: Symptoms, Pain, Activities of Daily Living, Sport, and Quality of Life. Pain was also rated both preoperatively and 2 years postoperatively using a visual analog scale (VAS). These PRO surveys have been validated 12 in past studies of hip arthroscopic surgery outcomes to assess a patient’s pain, functional status, and quality of life. All data were recorded in REDCap (Version 7.0.19; Vanderbilt University).
Statistical Analysis
An a priori power analysis was performed based on results of a previous study analyzing preoperative and 2-year postoperative mHHS scores in patients undergoing hip arthroscopic surgery. To adequately power the study to 1 – beta = 0.95, a total of 42 hips were needed. 9 A paired Student t test was used to calculate the statistical significance between preoperative and postoperative PRO scores. A logistic regression analysis was then performed with preoperative, 2-year postoperative, and change from preoperative to 2-year postoperative PRO scores. The analysis was performed to evaluate for significant trends in PROs with increasing surgical experience and case number. A similar analysis was performed on procedure and traction times. The correlation coefficient was used to provide information on the strength and direction of a relationship between the 2 continuous variables. Analysis of variance was also used to compare differences in mean procedure and traction times between cases categorized in groups of 10, with post hoc pairwise comparisons with Bonferroni correction performed when appropriate. A nonlinear regression analysis was performed to fit a curve for the predicted traction time relative to the case number in groups of 10. A P value <.05 was considered statistically significant for all calculations. All statistical computations were conducted in Excel for Mac (Version 16.30; Microsoft) and Stata (Version 14.2; StataCorp).
Results
Patient Characteristics
Patient characteristics are provided in Table 1. A total of 168 (88%) patients completed a 2-year follow-up after surgery and were included for analysis. The study included 91 female and 77 male patients with a mean age of 35.3 ± 9.6 years and mean body mass index of 25.07 ± 3.98. Of the 168 patients, 167 patients had a labral tear, and 166 patients had a cam lesion.
Patient Characteristics and Intraoperative Findings (n = 168) a

a Values are reported as mean ± SD unless otherwise indicated.
Intraoperative Findings and Procedures
Intraoperative findings are provided in Table 1. There were 163 patients who underwent labral repair (mean, 2 anchors) for full-thickness tears and 4 patients who underwent labral debridement for partial tears. Femoroplasty was performed in all 168 patients. The mean procedure time was 91.5 ± 23.9 minutes, and the mean traction time was 54.0 ± 17.7 minutes. Logistic regression demonstrated that the procedure time and traction time were significantly longer for initial cases relative to later cases (P < .0001). An inverse relationship between case number and procedure and traction times was observed (Figures 1 and 2). The R 2 value for the nonlinear regression analysis was 0.99 for procedure and traction times (P < .0001) (Table 2). Procedure times were analyzed in groups of 10 cases and found to be significantly shorter after 70 cases (P < .05). Traction times were significantly shorter after 110 cases (P < .05).
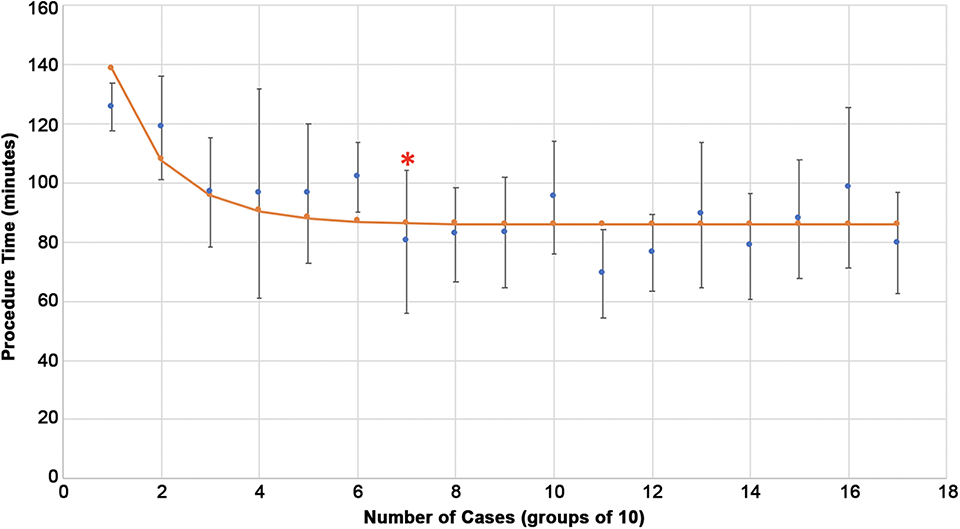
Change in procedure time with increase in case volume. The asterisk denotes the number of cases (groups of 10) at which there was a significant decrease in the mean and further changes plateaued.

Change in traction time with increase in case volume. The asterisk denotes the number of cases (groups of 10) at which there was a significant decrease in the mean and further changes plateaued.
Correlation of Procedure and Traction Times With Increasing Case Number

Patient-Reported Outcomes
The preoperative, 2-year postoperative, and change from preoperative to 2-year postoperative PRO scores are provided in Tables 3 to 6. There was no relationship noted with increasing case number and 2-year postoperative scores. With increasing case number, there was an increase in preoperative scores, with the exception of the SF-12 mental component summary and VAS. There was no correlation noted between increasing case volume and improvements from preoperative to 2-year postoperative PROs for all scores, with the exception of the mHHS in which there was a minor decrease in the score change with increasing case number (P = .044). Of note, there was no trend found between increasing case volume and postoperative complications, as there were no reoperations and no major complications in this cohort and only 4 cases of minor complications (2 pudendal neurapraxia and 2 lateral femoral cutaneous neurapraxia that lasted less than 3 weeks in each case).
Change From Preoperative to Postoperative PRO Scores a
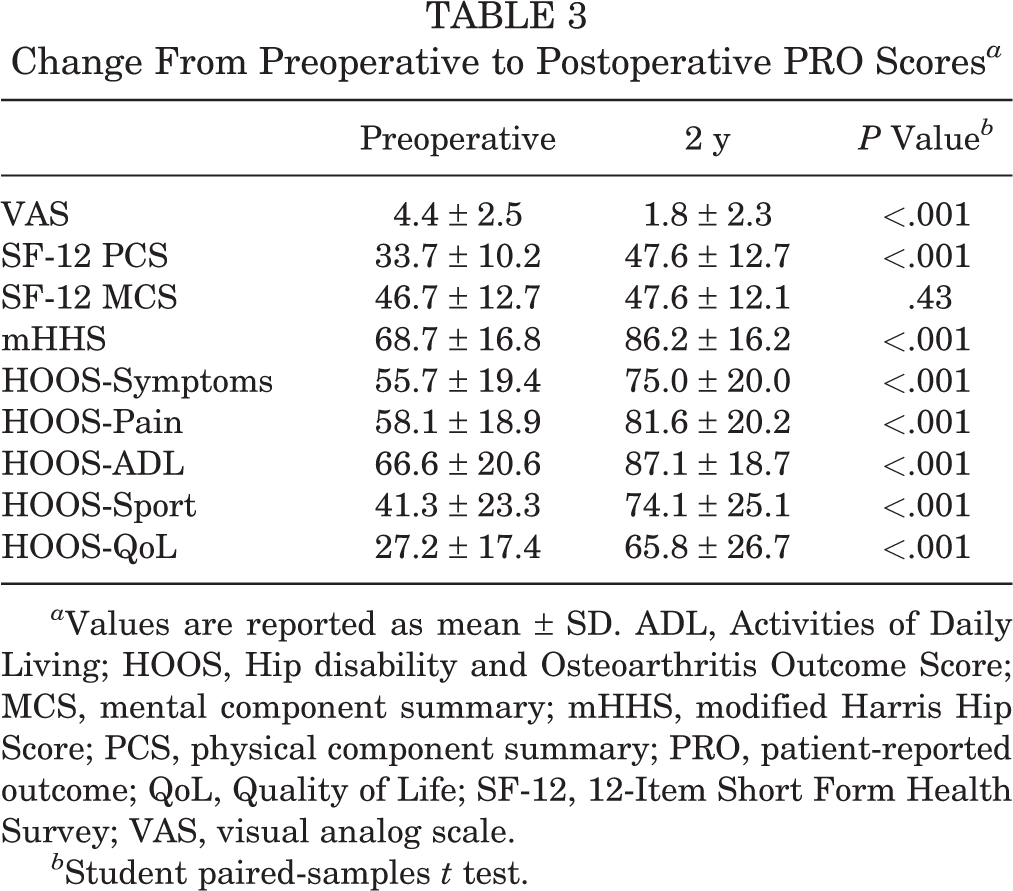
a Values are reported as mean ± SD. ADL, Activities of Daily Living; HOOS, Hip disability and Osteoarthritis Outcome Score; MCS, mental component summary; mHHS, modified Harris Hip Score; PCS, physical component summary; PRO, patient-reported outcome; QoL, Quality of Life; SF-12, 12-Item Short Form Health Survey; VAS, visual analog scale.
b Student paired-samples t test.
Correlation Between Preoperative PRO Scores and Increase Case Number a
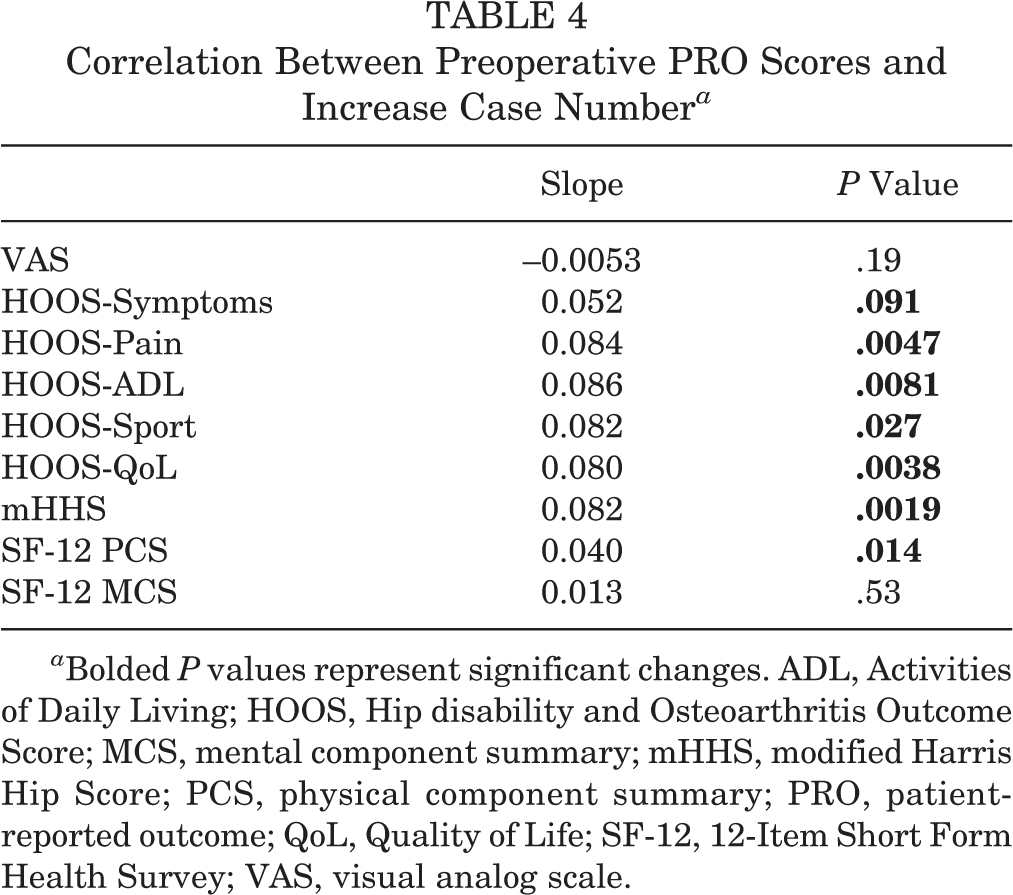
a Bolded P values represent significant changes. ADL, Activities of Daily Living; HOOS, Hip disability and Osteoarthritis Outcome Score; MCS, mental component summary; mHHS, modified Harris Hip Score; PCS, physical component summary; PRO, patient-reported outcome; QoL, Quality of Life; SF-12, 12-Item Short Form Health Survey; VAS, visual analog scale.
Correlation Between 2-Year Postoperative PRO Scores and Increasing Case Number a

a ADL, Activities of Daily Living; HOOS, Hip disability and Osteoarthritis Outcome Score; MCS, mental component summary; mHHS, modified Harris Hip Score; PCS, physical component summary; PRO, patient-reported outcome; QoL, Quality of Life; SF-12, 12-Item Short Form Health Survey; VAS, visual analog scale.
Change From Preoperative to Postoperative PRO Scores a

a Bolded P values represent significant changes. ADL, Activities of Daily Living; HOOS, Hip disability and Osteoarthritis Outcome Score; MCS, mental component summary; mHHS, modified Harris Hip Score; PCS, physical component summary; PRO, patient-reported outcome; QoL, Quality of Life; SF-12, 12-Item Short Form Health Survey; VAS, visual analog scale.
Discussion
Many studies have recognized the technically challenging nature of hip arthroscopic surgery and suggested a learning curve in which a large number of cases are needed before achieving surgical proficiency. Although many studies correlate complication rates with the learning curve, PROs may provide a better assessment of a surgeon’s competency and understanding of a patient’s pain and function. The purpose of this study was to prospectively assess the relationship between surgeon experience in hip arthroscopic surgery for the treatment of FAI and PRO scores after surgery. In doing so, we found that as surgeon case volume increased, both procedure and traction times during hip arthroscopic surgery decreased, especially after 110 cases. However, PRO scores did not change with increasing surgeon experience, with significant improvements in all aspects for early and later cases.
It is difficult to define the learning curve in hip arthroscopic surgery, as evidenced by a lack of consensus in the literature. Conceptually, a learning curve is defined as a graph represented with consecutive cases on the horizontal x-axis and a measure of proficiency on the vertical y-axis. 21 Proficiency can be assessed by patient outcomes including complication rates and functional outcome scores or a measure of efficiency (operative time). Although simplistic, operative time may be an indirect measure of a surgeon’s skill. Maximal proficiency improvement occurs at the point where the learning curve plateaus. 21 Our finding that procedure and traction times decreased with increasing case volume does agree with results in previous studies. A systematic review by Hoppe et al 15 found decreased operative times when 30 cases were used as a cutoff. Another previous study found decreasing procedure and traction times after a surgeon’s first 30 cases. 11 However, the current study found that procedure and traction time decreased in a logarithmic curve, reaching a plateau after 70 and 110 cases, respectively. The procedure time plateaued before traction time, which indicates that efficiency in joint access and intra-articular labral repair needed for traction time proficiency takes longer to master compared with other aspects of the case that factor into the procedure time including patient setup, which can be time-consuming for hip arthroscopic surgery. Helping to define the “steepness” of the learning curve with respect to traction time is important, given that the majority of the minor complications such as skin necrosis and neurapraxia related to hip arthroscopic surgery can be attributed to traction injuries. 26
Our findings also suggest that surgeons may be able to obtain good outcomes with hip arthroscopic surgery for the treatment of FAI early on in their careers. Significant improvements in postoperative PROs were found in patients regardless of surgeon case volume in this study. Previous literature is in mixed agreement with these findings. One previous study demonstrated similar patient improvements between a surgeon’s first 30 cases and subsequent 30 cases. These results were using 1-year outcomes and a small cohort size. 11 These findings are in contrast to a prospective study of a single surgeon’s first 100 hip arthroscopic procedures by Konan et al, 16 which showed the highest patient satisfaction and improvement in postoperative Non-Arthritic Hip Score values in the past 30 patients compared with the first 30. The authors also noted a 40% decrease in operative time after the first 30 cases, leading them to quantify a learning curve of 30 cases. We believe that for surgeons starting hip arthroscopic surgery, proper patient selection and utilization of a safe and reproducible surgical technique can allow for good patient outcomes even early in their practice.
In this study, as surgeon experience increased, preoperative patient PROs increased slightly. This may indicate that as a surgeon’s comfort level with hip arthroscopic procedures grows, they may offer surgical management to patients with higher baseline functions instead of waiting for more severe clinical symptoms. The expansion of patient selection to include patients with higher baseline PROs coupled with unchanged postoperative PROs over time may have led to a slight decrease in mHHS improvement over time. As no other PRO improvement changed in the cohort and final 2-year postoperative PRO scores remained stable, this further demonstrates that surgical experience and increased technical proficiency did not change patient outcomes, and surgeons may achieve good outcomes early in their hip arthroscopic careers despite slower surgery times.
Limitations
The main limitation of this study was the use of a single surgeon’s experience. While this can standardize certain confounding factors such as surgical technique, the generalizability of the results may be limited, as it is dependent on the training and skill level of the surgeon. Larger studies with multiple newly trained surgeons are needed to determine whether our results are unique to the surgeon in our study. The inclusion period could be lengthened even further to see if further proficiency is achieved at midcareer or late-career stages. Complex cases such as labral reconstruction could be included for future studies. Additionally, our study’s 2-year follow-up prevented us from examining long-term outcomes. However, previous studies have shown that patients undergoing hip arthroscopic surgery for FAI achieve clinically significant improvements by 2 years after surgery. 12 Future longitudinal studies are needed to determine the risk for revision surgery or conversion to total hip arthroplasty based on surgeon experience.
Conclusion
Surgical efficiency in hip arthroscopic surgery for the treatment of FAI was maximized after 110 cases in this cohort. However, significant PRO improvements can be achieved early in a surgeon’s practice prior to maximizing surgical efficiency.
Footnotes
Final revision submitted April 11, 2020; accepted May 7, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.A.L. has received research support from Arthrex, educational support from Medwest and Smith & Nephew, and hospitality payments from Wright Medical. A.L.Z. has received research support from Zimmer Biomet, educational support from Arthrex, and consulting fees from Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of California, San Francisco (No. 14-14742).